
Abstract
Introduction
W
In this study, early superficial cancer of tongue is defined as a T1 or T2 tumor [TNM classification: NOMO (Union Internationale Contre le Cancer classification); type: superficial spread or exophytic; depth: <5 mm] (Fig. 1). The purpose of this study is to evaluate the results of CO2 laser treatment in patients with superficial tongue cancer.
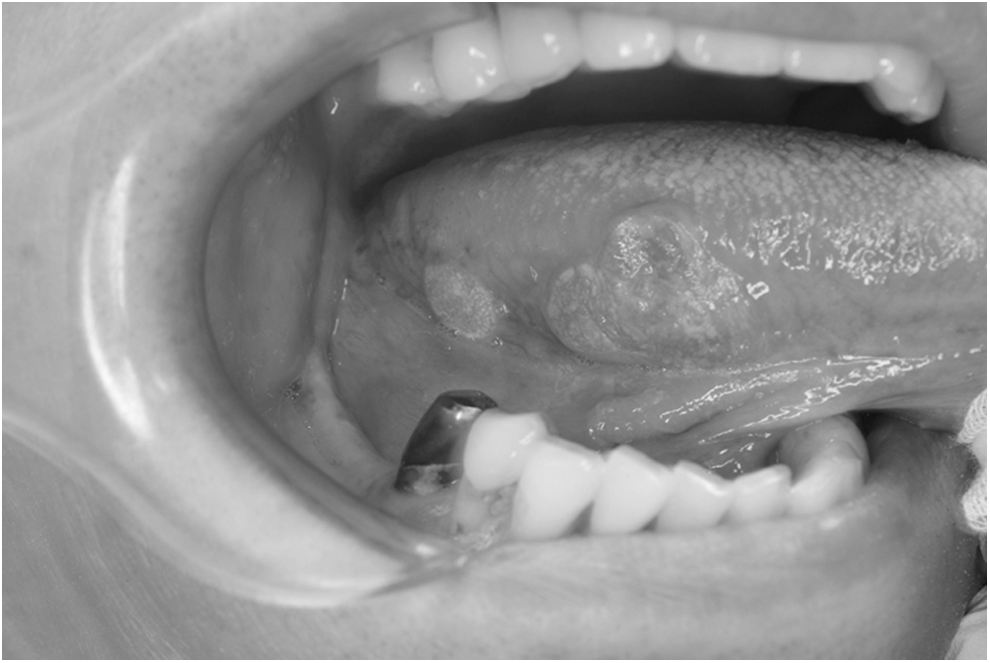
Early superficial cancer of the tongue, superficial spread type.
Materials and Methods
We retrospectively reviewed 31 primary cases of early superficial tongue cancer. The characteristics of the subjects are summarized in Table 1. This study population included 18 males and 13 females (mean age, 65.8 years; range, 40–90 years). Twenty-four patients were classified as stage I; 7 were classified as stage II. The results of the pathological diagnoses were Grade 1 (well-differentiated type; n = 21), Grade 2 (moderately-differentiated type; n = 6), and Grade 3 (poorly-differentiated type; n = 1); oral verrucous carcinoma (n = 2), and unclear (n = 1). All patients provided informed consent to participate in this study. This study conformed to the tenets of the Declaration of Helsinki study and did not require approval from the Medical Ethics Committee of Kobe University because of its retrospective nature. A total of 31 patients who were treated at the Department of Oral Surgery, Kobe University Hospital between October 2008 and May 2013 were included in this study. The patients were diagnosed with squamous cell carcinoma on the basis of biopsy results, and the absence of lymph node metastasis was confirmed by a computed tomography (CT) scan before partial glossectomy. The period from the biopsy until the operation was <8 weeks. In all the cases, treatment was performed under general anesthesia by nasotracheal intubation. Five of the patients had a history of cardiac failure, abnormal cardiac rhythms, or arterial sclerosis. They also showed a bleeding tendency due to taking anticoagulants or antiplatelet drugs (1 taking warfarin 100 mg per day, 1 taking warfarin 350 mg per day, 2 taking aspirin 100 mg per day, and 1 taking aspirin 200 mg per day.) No patients were taking anticoagulant and antiplatelet drugs at the same time. We do not ask patients undergoing partial glossectomy for early tongue cancer using a CO2 laser under general anesthesia to stop taking anticoagulant or antiplatelet drugs. The lesions were stained with 10% Lugol's solution and then were excised with a 5- or 10-mm safety margin from the nonstained area or induration using a CO2 laser (Bel Laser®, TAKARA BELMONT CORPORATION, Osaka, Japan) (Fig. 2). The parameters for the CO2 laser were a 10.6 μm wavelength, continuous wave mode, 5 kHz of frequency, and 3 W of the power (Table 2). In most cases, the raw surface was covered with a polyglycolic acid (PGA) sheet (NEOVEIL; GUNZE Ltd, Osaka, Japan) using fibrin glue spray. PGA is an absorbent material, which is used to reinforce sutures, to close pulmonary fistulas during lung surgery, to prevent pancreatic fistulas after pancreatectomy, to prevent the leakage of lymph from a fistula, and to prevent the leakage of bile. 5,6 We therefore used a PGA sheet with fibrin glue (Bolheal; Chemo-Sero-Therapeutic Research Institute, Kumamoto, Japan) as an adhesive. In the patients with known bleeding disorders, the wound was partially or completely sutured. All patients took nonsteroid anti-inflammatory drugs three times a day after every meal. During the first postoperative week (mean length of hospitalization), a pain assessment was performed. After discharge from the hospital (around postoperative day 14), another assessment was performed. We used a visual analog scale to assess the degree of postoperative pain. Follow-up examinations were performed every one and a half months. All patients were alternately examined by CT and ultrasonography once every 3 months.

The lesions were stained with 10% Lugol's solution and were excised with a 5- or 10-mm safety margin from the nonstained area or induration.
Results
In all cases, excision was performed using a CO2 laser. The raw surface was covered with a PGA sheet using fibrin glue spray (n = 23), sutures (n = 6), or both (n = 2) (Fig. 3). There were no cases of postoperative bleeding. Regarding the degree of postoperative pain, 17 patients showed less need for analgesic drugs at 2 weeks after surgery. By 1 month postsurgery, all patients were able to stop taking analgesic drugs. At the point where they stopped taking analgesic drugs, all patients indicated a 0–2 pain value. Regarding the postoperative swallowing difficulty, all patients were able to start swallowing rice gruel 2 days after the operation. The surgical margin was positive in 1 case, and negative in 28 cases. Epithelial dysplasia was observed on the surgical margin in three cases, while it was unclear in two cases because of the thermal denaturation of the excisional margin. Lymphatic, vascular, and nerve invasion were evident in three patients, two patients, and three patients, respectively. Additional resection was performed in the case with a positive margin after the first operation. Subsequent cervical lymph node metastases occurred without local recurrence in two patients. The duration of follow-up was 31–84 months. Subsequent cervical lymph node metastasis occurred after 6 and 17 months and modified radical neck dissection was performed. With the exception of one patient who died as a result of natural death, all of the patients remain alive.

The raw surface was covered with a polyglycolic acid sheet using fibrin glue spray, and partially closed with a suture.
Discussion
The dramatic developments in laser therapy have led to lasers being used in the treatment of oral lesions. Burkey et al. 7 noted that the literature on head and neck oncology continues to support the use of lasers in the surgery of malignant and premalignant lesions of the oral cavity. CO2 lasers are well suited for use in the transoral resection of premalignant lesions and early carcinomas of the oral cavity. The local control, 5-year survival rates, and postoperative function following CO2 laser treatment are at least comparable to those obtained using other surgical methods. 7 We began using CO2 lasers in the surgical treatment of precancerous oral epithelial lesions in the 1990s. At present, we also use them in the treatment of early superficial tongue cancer. The advantages of laser excision are said to include rapid and precise tissue dissection, bleeding control, good patient acceptance, low rates of morbidities and complications, and favorable healing. 8 Another report noted that the advantages of laser therapy in the management of benign oral mucosal lesions include minimal postoperative pain, conservative site-specific minimally invasive surgery, and the elimination of the need for sutures. Laser excision is well tolerated by patients with no intraoperative or postoperative adverse effects. 9 If partial glossectomy for early superficial tongue cancer using CO2 laser is proven to be associated with an equal or superior prognosis to traditional operation methods (i.e., procedures using scalpels and electric scalpels), then there will be many possible applications of laser therapy in the treatment of tongue cancer.
In this study, no patients required postoperative bleeding management, despite this study population containing patients who received antithrombotic therapy without drug cessation. In our hospital, we usually make a point of allowing patients undergoing partial glossectomy to continue to take their drugs at the time of the operation. If the extent of surgery is beyond partial glossectomy, we usually operate after heparinization. In most patients, the raw surface is covered with a PGA sheet because it allows for the sufficient control of any postresection bleeding. 10 Although 5 of the 31 patients took antithrombotic, antiplatelet, or anticoagulant drugs, only one of these patients was sutured. The other four who received antithrombotics were partially sutured. Examining the wound surfaces at the end of partial glossectomy to determine whether or not a patient has a bleeding tendency allows for good control of postoperative bleeding. However, in patients taking anticoagulant and antiplatelet drugs at the same time, we stop both drugs and require whole-body heparinization because of the high risk of bleeding. In such cases, we must be extremely careful about potential postoperative bleeding and the timing for restarting antithrombotics, and these patients require complete or partial suturing. Regarding concerns about intraoperative bleeding, the perioperative blood loss was lower in the patients in the CO2 laser group than in those in the cutting diathermy group (mean blood loss: 28.7 ± 9.2 vs. 52.9 ± 6.9 mL, respectively). The thermal damage zone with the CO2 laser has been shown to be less than 500 μm. Therefore, it is a relatively poor hemostatic technique, and is not very effective in controlling bleeding from vessels >0.5 mm in diameter. 2 When treating early superficial cancer of the tongue, a CO2 laser might be sufficient to control bleeding; however, for cases of invasive tongue cancer, an electric scalpel might be better for controlling bleeding.
Regarding the postoperative pain, all patients were able to stop taking analgesic drugs by 1 month after the operation. Using a PGA sheet with fibrin glue spray may exacerbate the postoperative pain compared to sutures, due to the tendency of wound to become stimulated. Therefore, laser surgery may result in greater postoperative pain than scalpel-based surgery, which is completed with sutures. However, postoperative pain was found to be 1.3 times less in patients in the CO2 laser group than in the diathermy group (p = 0.005). 2 As such, laser surgery itself may reduce the postoperative pain compared with diathermy.
Regarding postoperative swallowing difficulty, all patients were able to start swallowing rice gruel 2 days after the operation. We always deliver meals via infusion or enteral nutrition until 2 days after surgery to keep the PGA sheet stable. There was no risk of postoperative difficulty swallowing in any patients.
The margin could not be evaluated in two cases. There are concerns that the thermal denaturation of the excisional margin may prevent the histopathological diagnosis of specimens excised using CO2 lasers. However, tissue excised by a CO2 laser has been demonstrated to be more suitable for this purpose than tissue excised by an electrotome. 11 A scalpel causes less histological damage than a CO2 laser. It is possible that CO2 laser treatment will therefore result in a margin that is not evaluable. As a result, a frozen section diagnosis is often necessary in such cases.
There were no cases of local recurrence, and lymph node metastasis only occurred in two cases (Table 3). The 2-year local control rate was 100% and the subsequent cervical lymph node metastasis rate was 6.5%. This rate is better than that in other studies, except for those that involved laser therapy (Table 4). 12 –15 The reason for this finding is considered to be due to the fact that the other studies were geared toward all types of cancer, including endophytic type. Almangush et al. noted that the depth of invasion (DOI) is the strongest histopathological predictor of locoregional recurrence; the hazard ratio for a 4-mm DOI was 1.67 (95% confidence interval 1.07–2.60). 16 Another reason may be related to the shorter follow-up period of this study. In the one case with lymph node metastasis, the horizontal and vertical margins were over 5 mm, and the pathological grade was 1. There were no cases of lymphatic, vascular, or nerve invasion. Given that the secondary cervical lymph node metastasis intervals ranged between 6 and 17 months, a careful clinical follow-up is therefore necessary, regardless of the presence of invasion, to detect recurrence and metastasis.
Conclusions
In terms of recurrence, metastasis, postoperative bleeding, postoperative pain, and swallowing, partial glossectomy for early tongue cancer using a CO2 laser might help improve the postoperative course.
Footnotes
Author Disclosure Statement
No competing financial interests exist.