
Abstract
Introduction
A
Low-level laser therapy (LLLT) has been used for longer than half a century for several purposes, such as the treatment of periodontal inflammation, bone healing, and pain reduction. 14,15 Mester was the first researcher who studied the effects of low-intensity lasers on the acceleration of wound healing. 16 LLLT biostimulates and accelerates wound healing by altering the cellular behavior of fibroblasts and keratinocytes and by enhancing collagen synthesis, angiogenesis, and growth factor release, in a dose-dependent manner. 17 –19 These influences resulted in the stimulation of regeneration and epithelialization in human and animal tissue. 20 There are several studies that show the positive effects of LLLT on inflammation, soft tissue, and bone healing and side effects such as postoperative pain. 14,15,19,21 –24 LLLT not only accelerates wound healing by acting on the inflammatory process but also improves microangiogenesis. 25 It has been reported that lasers also reduce pain. 26
The aims of this study are to evaluate the effects of LLLT therapy on early wound healing and on a patient's complaints such as bleeding, pain, and burning sensations after the FGG procedure.
Materials and Methods
Subjects and study design
Approval was obtained from Karadeniz Technical University Faculty of Medicine Ethic Council with number 24237859-545 and date 08.09.2014 at the beginning of this single-center, randomized, double-blinded, prospective, and controlled clinical study (see supplementary Table S1 at
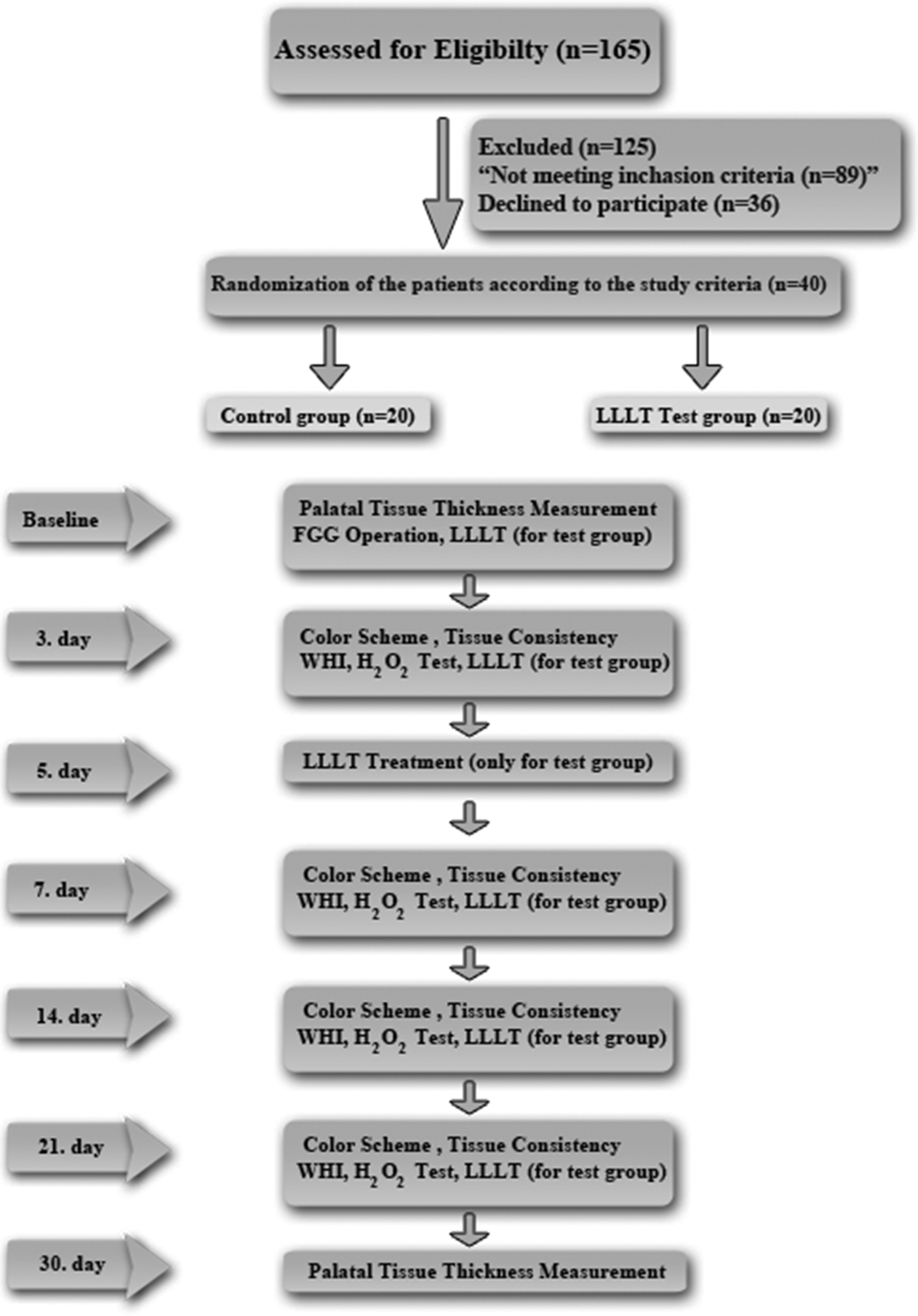
Flow-chart of study. LLLT, low-level laser therapy.
The trial was conducted between September 2014 and August 2015 at the Department of Periodontology, Karadeniz Technical University. Forty patients requiring FGG were selected. Each participant provided written informed consent after receiving detailed verbal and written information about the technique. The patients were randomly assigned to one of the groups by the periodontists with the toss of a coin.
The inclusion criteria were as follows: 1. The absence of systemic factors (no systemic disease, no coagulation disorders, no medications affecting periodontal status, and no pregnancy or lactation) 2. No smoking 3. Patients who had a full mouth plaque score <20% and a full mouth bleeding score <20% 4. No periodontal surgery on the experimental site 5. No nauseal reflection
To minimize the differences related to the surgical technique, all surgical procedures were carried out by one experienced clinician (G.U.)
Presurgical treatments
All selected patients underwent a professional periodontal prophylaxis phase, and all patients were given proper oral hygiene instructions. The patients were assigned to the control or test groups by the coin toss method.
Surgical procedure
After a regional local anesthesia that was applied around palatinum majus, the FGG was harvested as follows: The donor site extended from the distal line angle of the canine to the mesial line angle of the maxillary first molar by a conventional scalpel. An ∼1.5 mm split-thickness and rectangular-shaped (7 × 12 mm) gingival graft was obtained. The FGG was sutured to the prepared recipient bed by using size 5–0 resorbable sutures.
Test group—LLLT
The Ga-Al-As laser was used for LLLT at a wavelength of 940 nm and an intensity that has been previously calibrated by the manufacturer (Ezlase; Biolase® Technology, Inc., İstanbul, Turkey).
The wounds in the experimental group received laser stimulation at doses of 8.6 J/cm2, very close to a previously described dose (10 J/cm2) in the literature. 12 The power output was maintained at a constant 3 W in continuous-wave mode; the pulse interval size was 0.10 msec, and the pulse length was 0.05 msec. Laser energy was applied via a 400-μm optical fiber with a Whitening and Pain Relief Handpiece® (Table 1). The handpiece was positioned at a distance of ∼1 mm above the wound area, perpendicularly in noncontact mode. The area of the handpiece covered the entire wound area (Fig. 2), with a beam size of 2.8 cm2. The wound area was 7 × 12 = 0.84 cm2. Thus, the area of the probe was wider than that of the wound. The wound area was irradiated with a dose of 8.6 J/cm2, with an irradiation time of 8 sec. The total applied energy was 24 J, but the energy over the actual wound area was 7.2 J. LLLT was initiated directly after surgery and was repeated on the third, fifth, and seventh days after the operation. The cumulative dose was 34.4 J/cm2 in total.

The application of Ga-Al-As laser.
Control group—LLLT sham
Sterile wet gauze was pressed to the FGG donor site for 5 min in the control group. The LLLT was performed in the same manner with the test group. However, no irradiation occurred because of not pushing the start button.
Postoperative care
A noneugenol pack was placed over the sutured FGG (Coe-Pak™ Periodontal Dressing; GC America, Inc., IL). An acrylic stent was prepared to protect the palatal donor site, was placed after surgery, and was recommended to patients to wear for 7 days (Fig. 3). Patients were prescribed 500 mg of paracetamol (if needed) and a 0.12% chlorhexidine oral rinse (Kloroben, Drogsan, Turkey) twice a day for 2 weeks. The patients were advised to report any adverse outcomes and were recalled at 3rd, 7th, 14th, 21st, and 30th days (the 5th day for the LLT group). The sutures were removed after 2 weeks.

Acrylic stent.
Evaluated parameters
All evaluations were acquired by one of the authors (E.E.) who was blinded to the treatment assignment. The following parameters were recorded: H2O2 bubbling test for screening complete epithelialization, the Landry Wound-Healing Index (WHI), pain and burning sensations by a Visual Analog Scale (VAS) score, bleeding (yes/no), palatal tissue consistency, color match, tissue thickness (TT), and the number of analgesics.
Intra-surgical measurements of soft TT
The thickness of the palatal soft tissue in the harvesting area was measured after local anesthesia. The measurement was made ∼5 mm apical to the gingival margin of the first premolar by means of a #20 endodontic reamer with a silicon stopper (Güney Dis Malz, Trabzon, Turkey). The thickness of the palatinal tissue was measured in the test and control groups. The penetration depth was measured with a digital caliper (Astor, China). The dimensions of the graft were standardized by a sterile aluminum foil template that was 7 × 12 mm in dimension.
Subjective assessments
During the 7 days after the FGG procedure, the patients were asked to keep a diary of pain and burning sensations by using a VAS to evaluate the intensity of the given event. The VAS score for pain ranged from 0 (no pain) to 100 (severe pain), represented by a continuous line of 10 cm length; whereas the burning sensation was scored as follows: 0 (absent) to 100 (severe burning). In addition, the patients were asked to report their postoperative bleeding for 7 days as “Bleeding present (+)” or “Bleeding absent (−).”
Palatal tissue consistency
The consistency of the palatal mucosa was assessed on the 3rd, 7th, 14th, and 21st days by palpation with a blunt instrument and was scored as soft or firm by a clinician who was blinded to the treatment assignment.
Color match
On the 3rd, 7th, 14th, and 21st days, the color of the palatal mucosa was assessed by comparing it with that of the adjacent and opposite side by using the objective VAS (VAS score 0–100) represented by a continuous line of 10 cm length, by a clinician blinded to the treatment group assignment. A score of 0 indicated no color match, and a score of 100 indicated a very good color match with the adjacent tissues.
Wound epithelialization
Complete wound epithelialization (CWE) was evaluated clinically by the peroxide bubbling test. 27 This was the primary outcome of this study. This test is based on the principle that if the epithelium is discontinuous, then H2O2 diffuses into the connective tissue, and the enzyme catalase acts on H2O2 to release water and oxygen, which is clinically observed as the production of bubbles on the wound. The area to be evaluated was dried, and 3% H2O2 was sprinkled on the wound with a syringe, followed by a period of waiting (∼10 sec) for the appearance of bubbles, which suggest that the surgical site was not completely epithelialized.
Landry WHI
The palatal wounds were scored by using the Landy WHI on the 3rd, 7th, 14th, and 21st days postoperatively. 28 This index evaluated the wounds based on the following criteria: tissue color, response to palpation, incision margins, and suppuration. The scores range from 1 to 5 and correspond to very bad to excellent healing.
The number of analgesics
Patients were asked to record the number of analgesics taken for pain relief during the first 7 postoperative days.
Statistical analysis
The homogeneity of the data was tested by the Shapiro–Wilk test. Nonparametric tests were used. SPSS v.17.0 (SPSS, Inc., Chicago, IL) was used for the analysis. The Mann–Whitney U test was used to analyze intergroup differences. Time-dependent alterations were analyzed by the Wilcoxon test. The Binary Logistic Regression Analysis was performed to analyze the factors that affect epithelialization. Significance level was p < 0.05.
Power calculation
The primary outcomes of this study were the H2O2 test results on the 14th day. The power analysis was performed with
Results
The experimental groups were balanced by age and gender (p > 0.05, Table 2). Two patients in the control group and three patients in the LLLT group were dropped from the study, because they did not regularly attend the follow-up visits.
The Mann–Whitney U test was used to analyze intergroup differences.
LLLT, low-level laser therapy; NS, non-significant.
Postoperative pain, burning sensation, and the number of analgesics did not differ during the first week (data not shown).
All patients in the control group and 52.9% of patients in the LLLT group reported palatal bleeding on the first day. The prevalence of bleeding was 66.7% for the controls and 5.9% for the LLLT group by the second day. The differences between the two groups were statistically significant (p < 0.05 for the first day; p < 0.001 for the second day, Fig. 4).

Self-reported bleeding prevalance.
Tissue consistency did not differ significantly between groups at any of the clinical follow-up visits (data not shown).
The LLLT group had better color matching as assessed by VAS scale scores compared with the control group on the 3rd, 7th, and 14th days. However, this discrepancy disappeared on the 21st day (Table 3).
The Mann–Whitney U test was used to analyze intergroup differences.
All groups had incomplete epithelialization on the third and seventh days according to the H2O2 bubbling test results. However, the LLLT group had a significantly faster CWE than the control group on the 14th day (p < 0.001). All patients in the two groups showed CWE on the 21th day (Fig. 5).
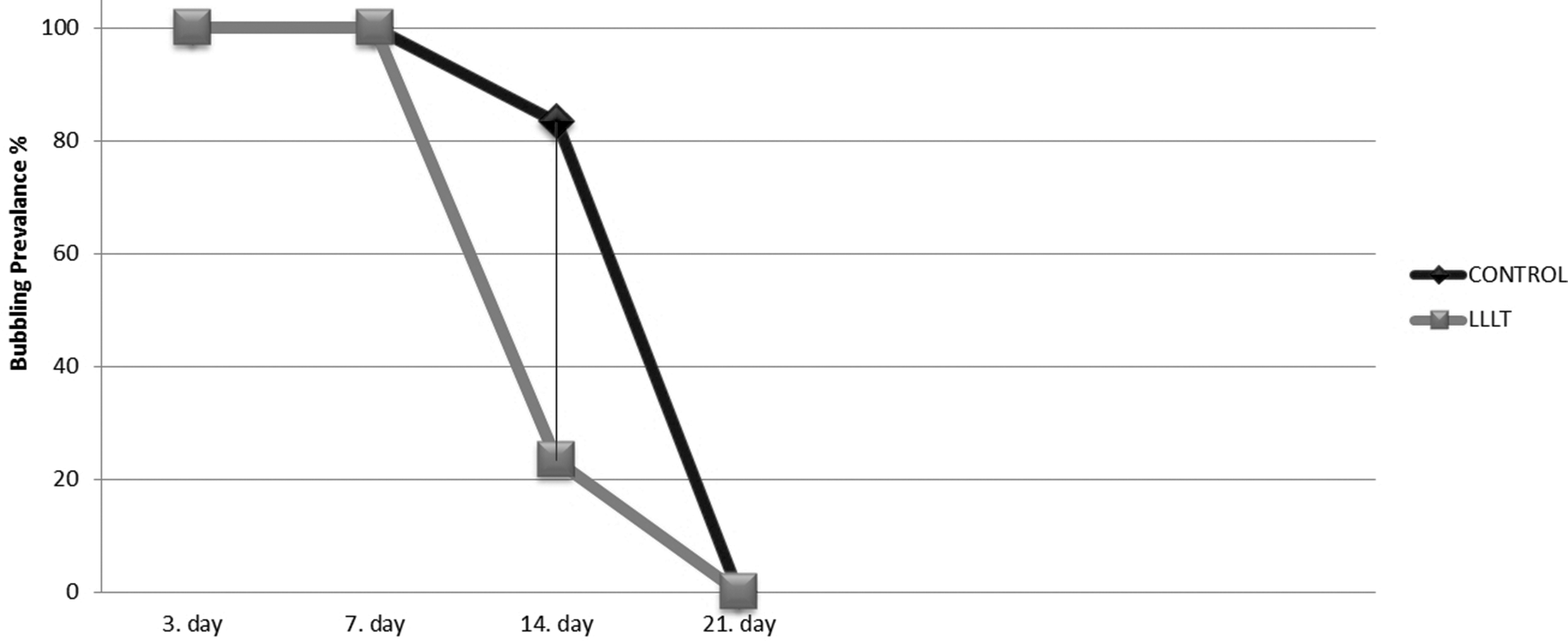
H2O2 test results.
The primary outcome of this study was the H2O2 bubbling test results on the 14th day. From the Binary Logistic Regression Analysis, we concluded that there was a significant relationship between LLLT and CWE (p < 0.001, 95% confidence interval; 0.062 [0.012–0.32]).
The LLLT group had better WHI scores than the control group throughout the follow-up period (p ≤ 0.001) (Table 4). The time-dependent clinical healing patterns are shown in Fig. 6.

Clinical healing patterns of groups.
The Mann–Whitney U test was used to analyze intergroup differences.
The mean baseline donor site TT was 4.23 ± 0.62 mm in the controls and 4.62 ± 0.79 mm in the LLLT patients. The baseline TT did differ significantly between the groups. After 4 weeks of healing, the average postpalatal TT was 4.01 ± 0.68 mm in the controls and 4.71 ± 0.82 mm at the LLLT-treated sites. When time-dependent alterations were analyzed by palatal TT, the differences did not reach statistically significant levels according to the Wilcoxon test results (Fig. 7).
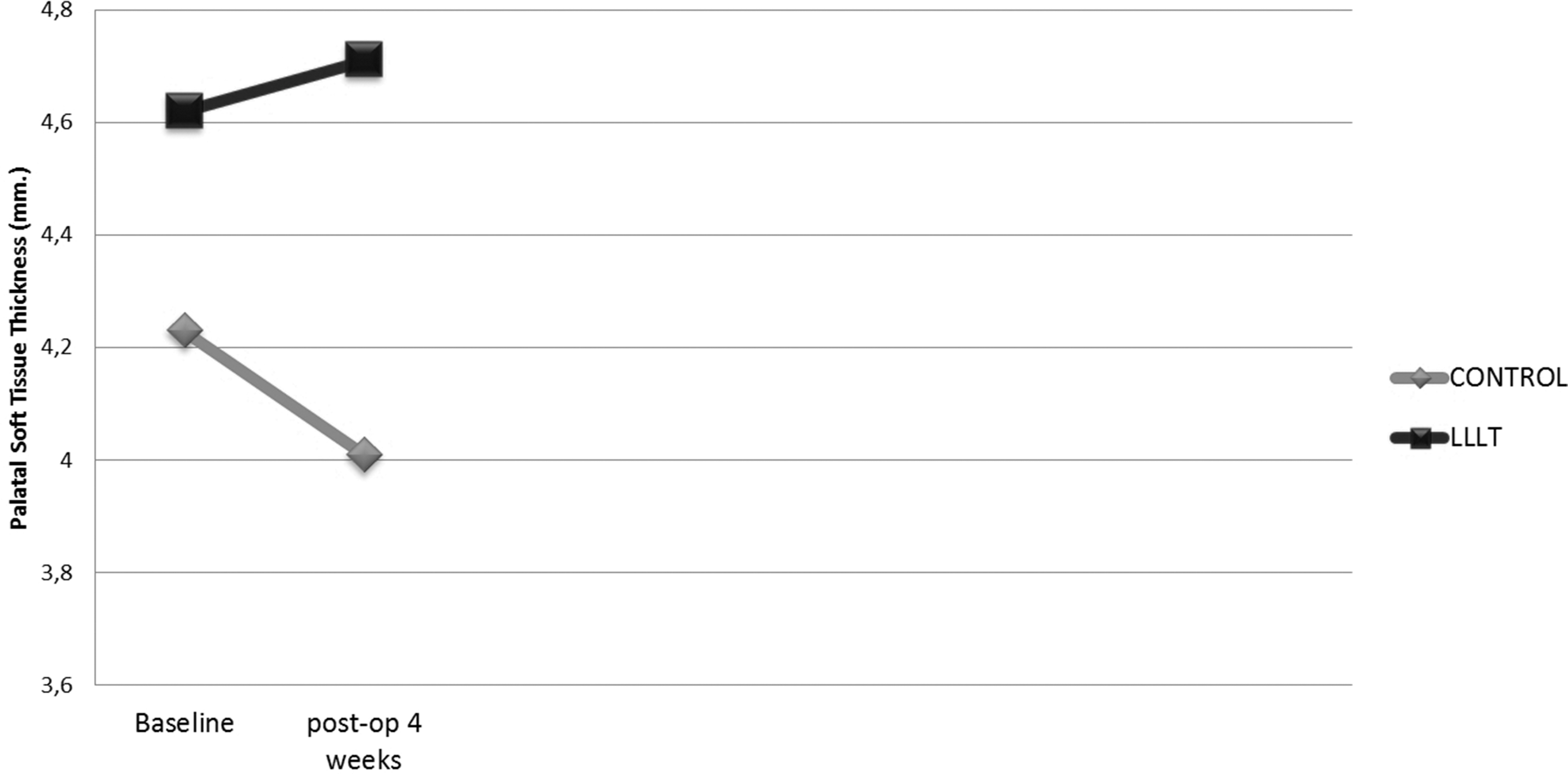
Time-dependent alteration of palatal tissue thickness.
Discussion
There are many studies about the effect of LLLT on wound healing. 12,19,24,29,30 However, there are few human studies that research the effect of LLLT therapy on palatinal donor sites. 29,31 Dias et al. showed the positive effects of LLLT on human palatal donor site healing. 31 In a recent study, Ozcelik et al. concluded that LLLT therapy decreased postoperative morbidity after FGG harvesting. 29 We analyzed FGG donor site as a secondary wound healing human model and according to the results of our study, LLLT enhanced wound epithelization and secondary wound healing, preserved palatal soft tissue thickness (PSTT), and decreased postoperative donor site bleeding compared with the control group.
Different laser procedures were reported in the literature. There is no consensus about the most appropriate laser wavelengths and doses to accelerate healing. As per our knowledge, laser energy has a “window effect.” High-energy densities result in the inhibition of cellular functions, and low-energy densities result in no observable effects. 32 Recently, by irradiation with a 10 J/cm2 Ga-Al-As laser, the healing of palatal mucoperiosteal wounds was promoted, which was presumably associated with the increased mitogenesis of fibroblasts. 12 Similarly, we were able to show that most patients (76.5%) in the LLLT group had complete wound epithelialization on the 14th day compared with the control group (p < 0.001).
The differences for the Landry WHI were significantly different between two groups. Higher scores were recorded for the LLLT group. In a study published by Dias et al., they reported positive effects of laser irradiation on the palatal donor site of CTG. 31 These positive effects of LLLT on wound healing were reported in another study that used an animal model. 12 Our laser type, wavelength, energy density, application intervals, and follow-up times were very close to those used in this study. They reported a higher fibroblast activity in the LLLT group compared with the control group on day 14. Also, a thicker epithelium was observed on day 21 compared with the control group, and a higher rate of papillae was demonstrated. According the histological and biochemical experiments, LLLT had beneficial effects on the inflammatory response and increased fibroblast proliferation. The limitation of our study was that we did not histologically evaluate the wound areas.
We also evaluated postoperative morbidity during the first 7 postoperative days. There are only few studies that showed the effects of LLLT on postoperative palatal donor site morbidity after soft tissue graft harvesting. 29,31 In one of them, Ozcelik et al. used a diode laser with wavelength 810 nm, at a total dosage of 4 J/cm2 for 5 min for palatal wound irradiation. 29 They concluded that LLLT decreased postoperative morbidity at the palatal donor site. On the other hand, Dias et al. did not show any statistically significant difference between the LLLT group and the control group after CTG harvesting in terms of patient discomfort. They used Ga-Al-As diode laser with a wavelength of 660 nm and a total dosage of 15 J/cm2. 31 The treatment procedures differed between studies. There is no consensus on the ideal protocol. In addition, pain is a subjective sensation. Therefore, split-mouth studies with standardized LLLT protocols are needed to evaluate and to observe the effects of LLLT on postoperative morbidity at the palatal donor site.
The patients also reported less bleeding during the first 2 days. However, no data have described the anticoagulant effect of LLLT, and only one study has reported that LLLT may enhance platelet procoagulant activity. 33 This difference between the control and treatment groups may be attributed to this effect.
The soft TT decreased at the end of 1 month compared with baseline in the control group, whereas this thickness increased in the test group from baseline measures. However, these differences did not reach a statistically significant level. There was an increasing tendency of TT in the LLLT group. LLLT may produce this result by increasing fibroblast activity, collagen synthesis, and the release of growth factors. 19,34,35 It is especially interesting that the TT at the first month was thicker than at baseline. Soft TT—gingival thickness—at the palatal donor site is important to obtain soft tissue grafts with sufficient lamina propria. The lamina propria might get thinner during palatal donor site healing, and in the future high-quality grafts with adequate lamina propria thickness cannot be obtained because of thinning of soft tissue at the palatal donor site. Thus, in our study, the PSTT was decreased in the control group at the end of 1 month. Therefore, preservation of the PSTT as a potential donor site for soft tissue grafts is important. The results of our study showed that the LLLT procedure preserved the PSTT at 4 weeks. This may be attributed to the direct effect of LLLT on connective tissue cells and the release of growth factors from gingival fibroblasts as mentioned in the literature. 19,34 However, additional studies are needed with long follow-up periods.
Conclusions
Within the limitations of this study, we can conclude that biostimulation using the LLLT could benefit wound healing at the FGG donor area by accelerating wound healing. This technique also enables to preserve palatal soft TT after surgery. LLLT also helps to reduce postoperative self-reported bleeding. However, more clinical controlled split-mouth studies with long follow-up periods are needed to investigate the effect of the LLLT technique.
Footnotes
Acknowledgments
Author Disclosure Statement
The authors report that there is no conflict of interest. The study was self-funded by the authors and their institutions.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.