
Abstract
Introduction
A
Low-level laser therapy (LLLT) is also a safe and effective means of achieving significant reductions in body circumference. Following positive clinical study results, 8,9 two LLLT devices have received clearance by the U.S. Food and Drug Administration for use as noninvasive, dermatological esthetic treatment as an adjunct for individuals intending to undergo liposuction procedures for reduction of circumference of hips, waist, and thighs. A third device has been cleared for use as a noninvasive, dermatological esthetic treatment as an adjunct for individuals intending to undergo liposuction procedures for the reduction of circumference of the upper arms. 10
In addition to improved physical appearance and self-esteem, decreasing body circumference may have far-reaching health consequences. It is now recognized that adipose tissue is an endocrine organ that serves physiologically important functions. 11,12 In normal individuals, adipose tissue is the source of leptins, which regulate energy balance by acting centrally 13 to decrease food intake, 14 increase energy expenditure by decreasing appetite, 15 and controlling peripheral insulin sensitivity, free fatty acid oxidation, and lipolysis 16 ; however, when the mass of fat cells increases, adipocyte dysfunction leads to the release of various proinflammatory adipokines implicated in the development of insulin resistance, metabolic syndrome, and vascular disease. 17
Previous studies demonstrated the effectiveness of LLLT for reducing body circumference in the hips, thighs, and abdomen of nonobese individuals with a body–mass index (BMI) <30 kg/m2. 8,9,18 The purpose of this randomized, double-blind placebo-controlled study was to assess the effectiveness of an LLLT device as a noninvasive esthetic treatment for reducing body circumference in the hips, thighs, and abdomen of obese individuals with BMI between 30 and 40 kg/m2.
Methods
Study subjects
Obese, but otherwise healthy, male and female subjects, 18–65 years of age, seeking treatment to reduce their hip, waist, and upper abdomen circumference were enrolled. Subjects were required to have a BMI between 30 and 40 kg/m2, inclusive. Each subject met American Society of Liposuction Surgery/American Academy of Cosmetic Surgery criteria for the use of liposuction techniques for removing localized deposits of adipose tissues. 19
Subjects expressed their willingness to abstain from other weight loss or body contouring treatments, such as dietary or herbal supplements and appetite suppressants; weight loss programs or diet plans, such as Weight Watchers®, SlimFast,® or Atkin's® Diet; surgical procedures for body sculpting or weight loss, such as liposuction, abdominoplasty, stomach stapling, or lap bands; and alternative therapies, such as acupuncture, body wraps, hypnotherapy, or mesotherapy. Subjects agreed to maintain their regular diet and exercise routine for the duration of the study.
Reasons for exclusion from study participation included cardiovascular disease or prior cardiac surgery; prior surgical intervention for body sculpting or weight loss; medical, physical, or other contraindications for body sculpting or weight loss; use of medications known to cause weight changes; medical conditions known to affect weight or cause bloating or swelling; irritable bowel syndrome; infection, wound, or other external trauma to the planned treatment areas; photosensitivity disorder; cancer; pregnancy or planned pregnancy before study completion; serious mental health disorder, developmental disability, or cognitive impairment; or participation in a clinical study during the previous 30 days.
Study device
The laser is a preprogrammed, variable frequency device consisting of 10 independent 17 mW, 532 nm green laser diodes positioned 120 degrees from one another and tilted at a 30 degree angle (Erchonia® Emerald Laser; Erchonia Corporation, McKinney, TX). Internal mechanics collect light emitted from each laser diode and direct it through a proprietary lens, which redirects the beam with a line refractor. The refracted light of each diode is bent into a random spiral pattern that is independent of the other diodes. The sham LLLT device has the same physical appearance as the actual device and emits similar appearing visible green light when activated. The energy characteristics of the LLLT device are summarized in Table 1.
Procedures
To ensure consistency, hip, waist, and upper abdomen circumference measurements were made by the same study personnel. Hip circumference measurements were made such that both hip bones were encircled. For the waist (mid-abdomen) circumference, the distance from the hip bone to the point where the circumference of the waist was measured (at the subject's natural waist formation) was recorded after the first measurement for consistent postprocedure measurements. Similarly, the distance from the natural waist to the point of the upper abdomen was recorded after the first measurement to allow for measurement consistency.
Before treatment, the investigator recorded the presence and location of any existing skin markers on the hips, waist, and upper abdomen of each subject, such as hernias, scars, asymmetries, cellulite, stretch marks, or discoloration; stria and dimpling; underlying abdominal musculofascial system; presence or absence of flaccidity and diastasis recti; and quality and elasticity of the skin.
Each subject received 12 LLLT treatment sessions over the 4-week treatment phase (three procedures weekly). During each procedure, subjects laid face upward on the procedure table. The center diodes of the LLLT or sham device were positioned 4 inches (∼15 cm) above the abdomen, centered along the body midline, focused on the navel, and the device was activated for 15 min. The subject then laid face downward on the procedure table. The center diode of the device was positioned 4 inches above the back, centered along the body midline, focused on an area corresponding with the navel, and activated for 15 min. Safety glasses were worn by both the investigator and the subject during all LLLT procedures (KenTek C22-KMT-6101; KenTek Corporation, Pittsfield, NH).
Follow-up visits
Following 2 weeks of treatment (six LLLT sessions) and 4 weeks of treatment (12 LLLT sessions), BMI and hip, waist, and upper abdomen circumference were measured, a skin assessment was performed, and reported adverse events were recorded. In addition, digital images of the treated areas were obtained at 4 weeks, subject satisfaction was recorded, and perceived group allocation was recorded for subjects and the investigator. Two weeks after the final LLLT session, subjects were seen again for final BMI, hip, waist, and upper abdomen circumference measurements.
Efficacy end-points
Primary efficacy outcome measure was a statistically significant difference in the proportion of subjects who demonstrated a ≥3.0 inch (7.62 cm) reduction of their combined baseline hip, waist, and upper abdomen circumference after the 4-week treatment phase of the study. The 7.62 cm criterion was previously accepted as a clinically meaningful change by the U.S. Food and Drug Administration in clinical studies supporting the 510(k) clearance of the LLLT device for similar indications. 8,18
Overall study success criteria were defined as a ≥40% difference between procedure groups by comparing the proportion of individual successes in each group. The secondary efficacy outcome measures of BMI and individual hip, waist, and upper abdomen circumference measures were analyzed using Student's t-test and ANOVA. Additional outcome measures included self-reported subject satisfaction with treatment outcomes; deviations in subject's daily diet and exercise compliance; concomitant medication and therapy; and their relationship to study outcomes, changes in skin assessments, and reported adverse events.
At week 4, subjects were asked to indicate how satisfied they were with the appearance of their hips, waist, and upper abdomen using a five-point Likert scale in response to the question: How satisfied or dissatisfied are you with any change you may have noticed in the appearance of your hips, waist, and upper abdomen area after having received treatment with the obesity laser?
Subjects and investigators were each asked for their perceived group allocation and to record whether they believed each subject received actual or sham LLLT. Subjects were also asked to record any changes in diet or exercise routines, concomitant medications or therapies, and possible adverse events in daily diaries.
Safety end-points
At each evaluation, all potential adverse events reported by a subject or observed by an investigator were recorded. Patients were examined for any evidence of skin irritation, discoloring, rash, indentations, and infection.
Statistical analysis
It was anticipated that about 55% of subjects in the test group and about 15% of subjects in the control group would meet the individual success criteria. Based on the planned application of a one-tailed test with an alpha value of 0.05 and power of 0.8, a sample size of 22 subjects in each group was needed 20 ; however, as it was also anticipated that about one-twelfth of all subjects may withdraw from the study before completion for various reasons, 24 subjects were enrolled in each of the two treatment groups. Subjects were allocated to their treatment group using variable block randomization.
Ethics
The protocol used in this study adhered to the Good Clinical Practice guidelines of the International Conference on Harmonization.
21
The protocol and all related documents were approved by a commercial institutional review board (Western Institutional Review Board®, Puyallup, WA). Each subject provided informed consent before participating in any study-related activities.
Results
Fifty-three subjects with a mean age of 47.04 years were randomized to the active procedure group (n = 28) and the placebo group (n = 25) and all completed the study. Other baseline characteristics are summarized in Table 2. A series of t-tests for independent samples revealed no significant intergroup difference in any baseline measurements.
BMI, body–mass index; LLLT, low-level laser therapy; SD, standard deviation.
Efficacy measures
Among subjects treated with the LLLT device, 71.43% attained a ≥7.62 cm decrease in combined circumference measurements versus 12% of subjects who received the sham procedure (p < 0.00005). The overall mean (standard deviation) decrease in combined circumference measurement for subjects treated with the LLLT device was 10.52 (7.59) cm (p < 0.0001 vs. baseline) compared with 1.80 (32.0) cm for subjects who received the sham treatment (p < 0.05 vs. baseline). The mean combined circumference measurements at each study point are summarized in Table 3 and shown graphically in Fig. 1. The mean combined circumference measurements among subjects meeting the individual subject success criterion of ≥7.62 cm are shown in Table 3. The change in combined circumference measurements is shown in Fig. 2. For subjects treated with LLLT, the combined circumference measure further increased to 11.79 cm at the 2-week postprocedure evaluation. Representative pre- and post-treatment images are shown in Figs. 3 and 4.
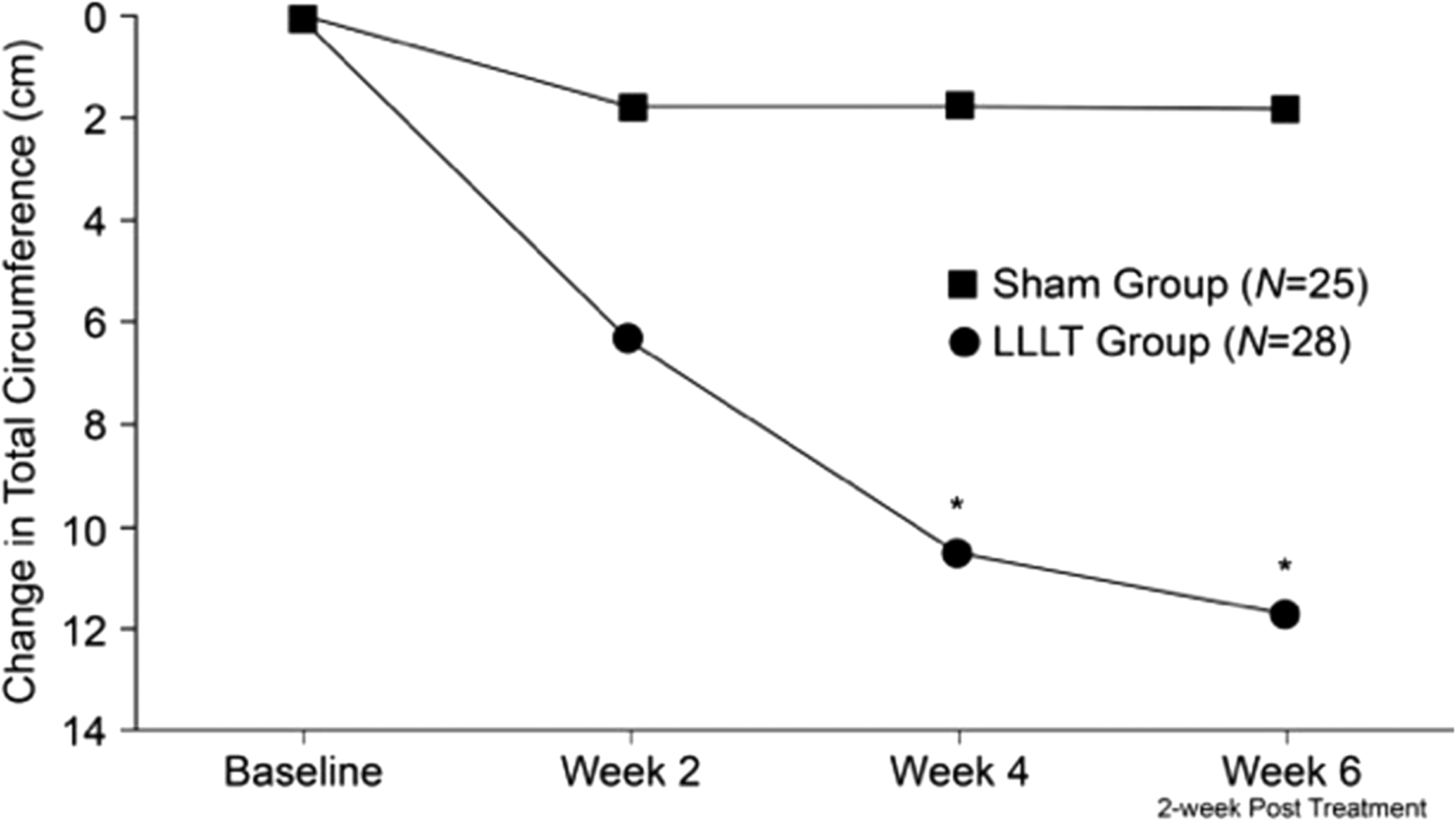
Mean change in total hip, waist, and abdomen circumference. *p < 0.0001.
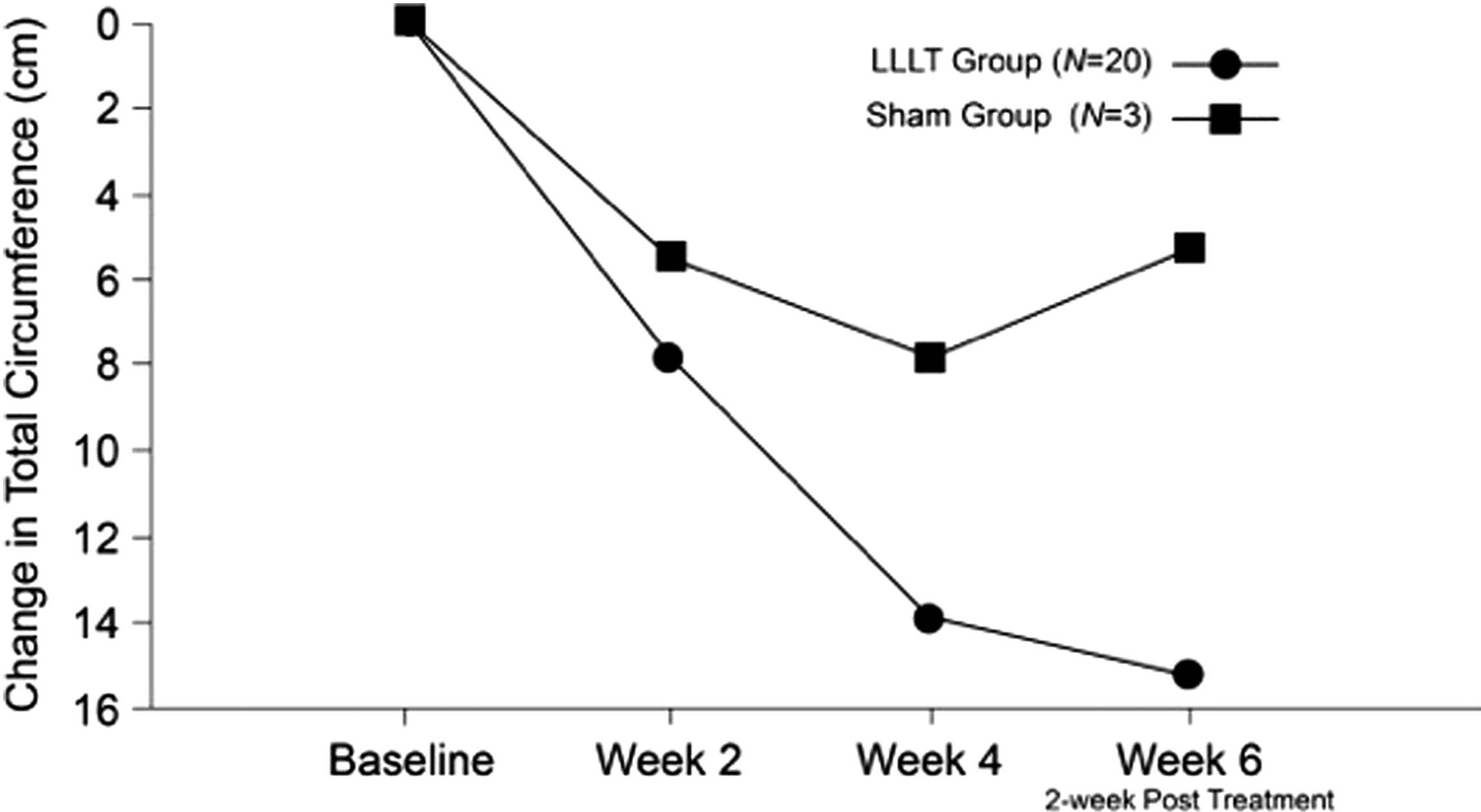
Total mean change combined circumference measurements among subjects meeting the individual subject success criterion of ≥7.62 cm.
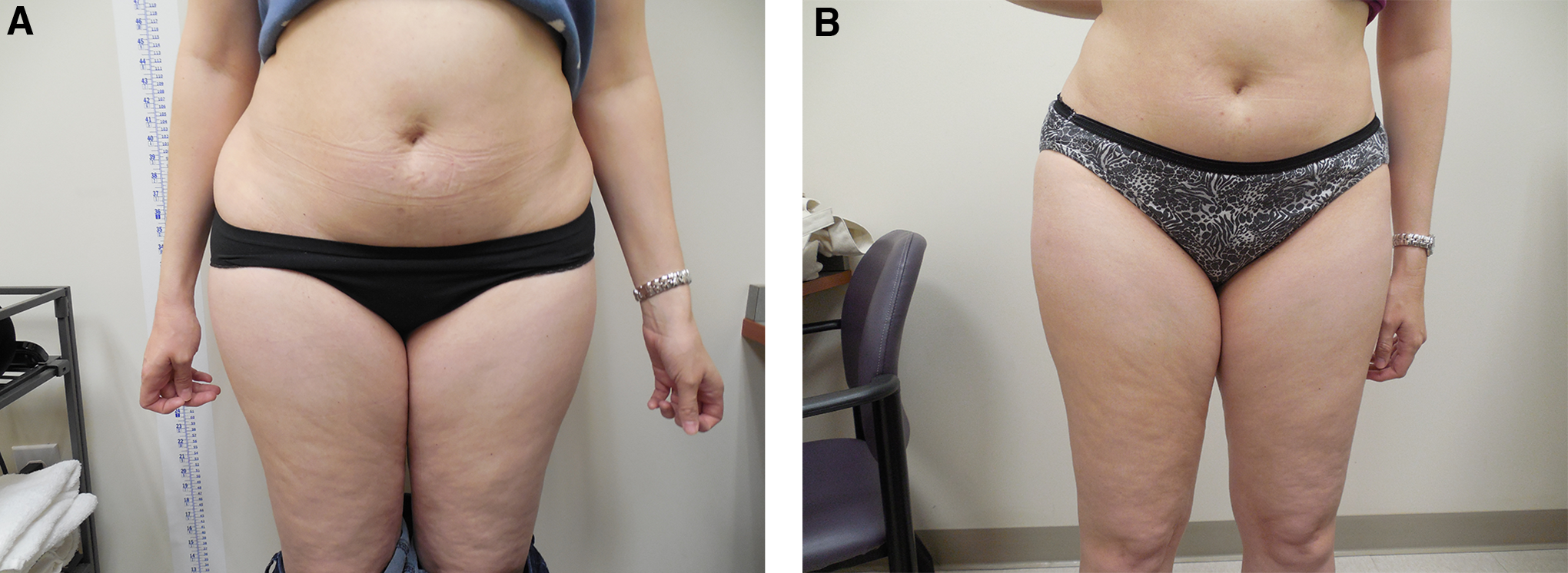
Frontal images of a subject
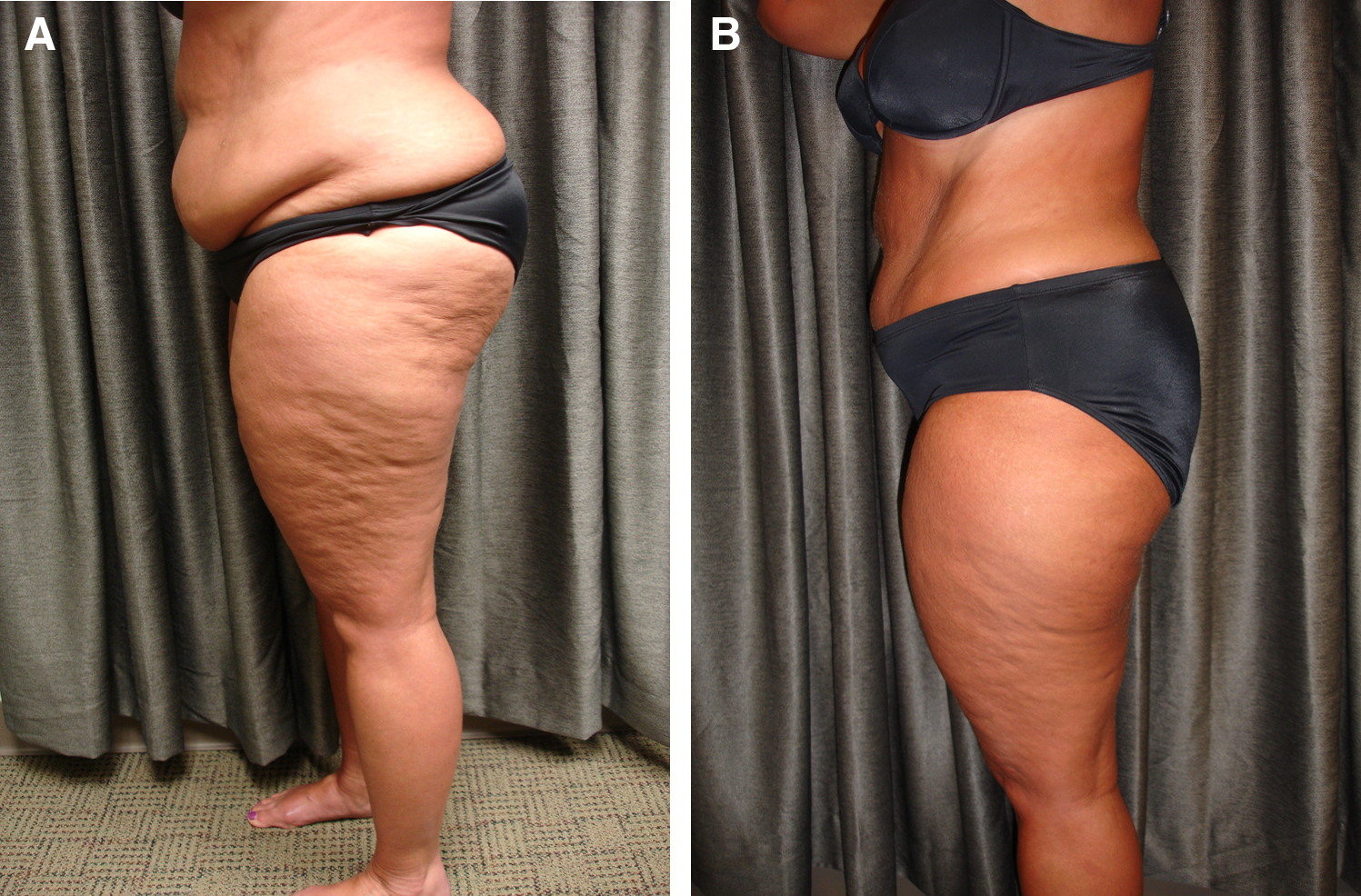
Lateral images of a subject
p < 0.0001 versus baseline.
p < 0.05 versus baseline.
There were too few sham-treated subjects for meaningful standard deviations.
p < 0.01 versus baseline.
Among the subjects meeting the individual subject success criterion of a combined decrease in inches of ≥7.62 cm, the mean combined circumference measurements decreased by 7.82 and 13.92 cm at weeks 2 and 4, respectively, further decreasing by 15.21 cm at the 2-week post-treatment evaluation.
For subjects undergoing sham treatment, their overall circumference remained essentially unchanged. Twelve subjects (48.0%) experienced no change and 10 subjects (40.0%) experienced a <7.62 cm decrease. In contrast, five subjects (17.9%) treated with LLLT achieved a 7.62 to <10.16 cm decrease, eight (28.6%) achieved a 10.16 to <15.24 cm decrease, and seven (25.0%) achieved a >15.24 cm decrease in total body circumference. A series of one-way ANCOVAs for two independent samples demonstrated that the efficacy of the LLLT device is independent of baseline body weight or BMI.
Among subjects treated with LLLT, individual baseline circumference measurements progressively decreased at each subsequent evaluation point, reaching a maximum mean decrease of 4.72 cm for the hips, 3.15 cm for the waist, and 3.83 cm for the upper abdomen (Table 4). For sham-treated subjects, the magnitude of the changes in individual baseline circumference measurements was very small, reaching a maximum mean decrease of 1.19 cm for the hips, 0.56 cm for the waist, and 0.10 cm for the upper abdomen.
There was no significant difference in weight loss or BMI among either LLT- and sham-treated subjects (Table 4). At the end of the 4-week treatment phase, 79% of subjects in the LLLT groups were very satisfied or somewhat satisfied with the results they achieved versus 16% of sham-treated subjects. Treatment group allocation was correct for 22 of 28 LLLT-treated subjects, (79%), and 19 of 25 sham-treated subjects, (76%). The treating investigators correctly determined subject group allocation for 25 of 28 LLLT-treated subjects (89%) and 20 of 25 sham-treated subjects (80%). Overall, LLLT-treated subjects were very satisfied (n = 17, 61%), somewhat satisfied (n = 5, 18%), neither satisfied nor dissatisfied (n = 5, 18%), not very satisfied (n = 1, 3%), or not at all satisfied (n = 0) with their treatment results. In contrast, sham-treated subjects were very satisfied (n = 0), somewhat satisfied (n = 4, 16%), neither satisfied nor dissatisfied (n = 11, 44%), not very satisfied (n = 5, 20%), or not at all satisfied (n = 5, 20%) with their results.
Safety measures
No subject reported any deviation from baseline diet, exercise, or concomitant medication use. Following completion of the 2-week treatment phase and the 2-week postprocedure phase, no changes in baseline skin markers were noted. There were no reports of adverse effects at any time during the study.
Discussion
LLLT, also known as nonthermal laser therapy, exerts its effects by the process of photobiomodulation. Various therapeutic benefits can be achieved by exposing tissues to specific wavelengths of light. 22 Photobiomodulation occurs when special molecules known as chromophores absorb a photon of light, raising an electron to an excited state. This molecule is most commonly the iron- and copper-containing enzyme cytochrome C oxidase located in the mitochondrial respiratory chain. 22 –24 Stimulation of cytochrome C oxidase results in increased mitochondrial activity, resulting in increased ATP, NADH, and RNA and cellular respiration; increased nitric oxide synthase activity and nitric oxide production; and increased reactive oxygen species, which play an important role in cell signaling, cell cycle progression, enzyme activation, and synthesis of proteins and nucleic acids. 22 –24
With respect to adipocytes, activation of cytochrome C oxidase triggers a number of cellular events, including increased ATP synthesis with subsequent upregulation of cAMP and cytoplasmic lipase activation. The activated lipase breaks down intracellular triglycerides into fatty acids and glycerol. 25,26 The activation of cytochrome C oxidase also results in transient formation of pores in the cell membrane of adipocytes, which allow the newly formed fatty acids and glycerol to pass through the membrane into the extracellular space. 27 The result is the complete collapse, but not death, of adipocytes exposed to the LLLT. 28
After leaving the cell, released lipids are transported to lymph nodes where lysosomal acid lipase hydrolyzes the released triglycerides to generate nonesterified free fatty acids. 28,29 Released lipids may also be transported to the liver through the lymph network where they undergo normal fatty acid oxidation. It should be noted that the release of lipids following LLLT does not elevate plasma lipids. Plasma triglycerides and cholesterol have actually been shown to decrease following the use of LLLT. 30,31 Since LLLT does not cause the death of adipocytes, the endocrine functions of adipose tissue are preserved. 32
In the current study, treating subjects with a BMI between 30 and 40 kg/m2 with 12 sessions of LLLT over a 4-week period resulted in a significant and clinically meaningful decrease in combined waist, hip, and thigh circumference. The mean decrease for all patients was 10.52 cm following the 4-week treatment period, but decreased further to 11.79 cm at the 2-week postprocedure evaluation. While the mean total circumference measurement decrease of 1.80 cm among sham-treated subjects was statistically significant, it was not clinically meaningful.
In addition to improving appearance and increasing self-esteem, a reduction in waist circumference is likely to contribute toward improved health. According to the World Health Organization, there is a convincing association between an increased waist-to-hip ratio and risk factors for cardiovascular disease, type 2 diabetes, hypertension, and several types of cancer. 33 Specifically, a waist-to-hip ratio ≥0.90 cm for men and ≥0.85 cm for women is associated with an increased risk for metabolic disease. At the end of the present study, there were a substantially greater number of subjects with a decreased waist-to-hip ratio among the LLLT-treated subjects (n = 13; 46%) versus the sham-treated subjects (n = 7; 28%).
Under healthy conditions, adipocytes in white fat store lipids and regulate metabolic homeostasis (reviewed by Balistreri et al. 34 ). M2-type macrophages release anti-inflammatory cytokines and arginase, which inhibits nitric oxide synthesis. In obese conditions, M1-type macrophages in white fat release nitric oxide synthase and proinflammatory cytokines. Thus, reducing stored body fat will decrease mediators of inflammation and other adipokines associated with obesity-related disease. 34
It is interesting to note that liposuction alone does not improve these metabolic derangements. In one study, there was a drop in leptin levels immediately following liposuction, which correlated with the amount of aspirated fat; however, the change was no longer significant after 6 weeks. 35 In another study, the effects of liposuction plus dieting on leptin levels were no different than dieting alone. 36 A large meta-analysis concluded that there is no evidence that subcutaneous fat removal reduces early cardiovascular or metabolic disease, its markers, or its risk factors. 37 In contrast, bariatric surgery can lead to beneficial changes in peripheral blood levels of some adipokines and hormones controlling energy turnover and appetite. 38,39 Among patients with type 2 diabetes, bariatric surgery resolved or improved in most patients. 40 It can be hypothesized that the effects of LLLT on metabolism of obese individuals are likely to be similar to bariatric procedures.
The beneficial effects of LLLT on adipose tissue occur through the process of photobiomodulation. This begins when a suitable chromophore becomes stimulated by absorbing a photon of laser light. In adipose cells, the chromophore is the copper-containing mitochondrial cytochrome C oxidase. 22 Activation of cytochrome C oxidase triggers a number of cellular events, including an increase in adenosine triphosphate synthesis with subsequent upregulation of cAMP and activation of cytoplasmic lipase, which breaks down intracellular triglycerides into fatty acids and glycerol. 26 In addition, cytochrome C oxidase activation results in the transient formation of pores in the cell membrane of adipocytes. 41 This allows the newly formed fatty acids and glycerol to pass through the membrane into the extracellular space. 27 Following 4 min of laser exposure, 80% of intracellular fat was released from adipose cells increasing to almost 100% after 6 min of exposure, 28 resulting in the complete collapse, but not death, of treated adipocytes.
Upon entering the extracellular space, lipids released following LLLT are transported to lymph nodes where lysosomal acid lipase hydrolyzes the released triglycerides to generate nonesterified free fatty acids. 28 Alternatively, released lipids may be transported through the lymphatic system to the liver where they undergo normal fatty acid oxidation. Although the metabolic fate is not known with certainty, it is known that the release of intracellular lipids does not contribute to elevated plasma lipids. In fact, the use of LLLT clinically has been associated with decreased plasma triglycerides and cholesterol. 31 Importantly, LLLT does not result in tissue necrosis. Consequently, the endocrine functions of adipose tissue 32 are preserved while avoiding the inflammatory response associated with the use HIFU 42 and cryolipolysis. 43
As a cosmetic procedure, LLLT was first used to decrease tissue trauma and inflammation and promote wound healing after lipoplasty-assisted liposuction. 41 Since that time, LLLT has become an effective stand-alone method for body contouring. In an initial study, subjects with a mean BMI of 25.74 kg/m2 (n = 35) were treated with a multiple-head, low-level diode laser consisting of five independent diode laser heads emitting 635 nm (red) laser light with an output of 17 mW. 18 Similar to the present study, each subject received three weekly treatment sessions for 2 weeks with each treatment 2 days apart. At the end of the treatment period, the mean decrease in waist circumference was 8.94 cm. In a subsequent retrospective study, subjects undergoing the same treatment protocol with the same LLLT device (n = 689) achieved a decrease in waist circumference of 2.90 cm. 8 These results have been confirmed by independent investigators who showed that subjects treated with the LLLT device (n = 86) achieved mean abdominal circumference reduction of 2.84 cm. 44 Comparable circumferential reductions have been observed in subjects undergoing treatment of the hips, thighs, 8,18,44 and upper arms. 10
In addition to tumescent liposuction, numerous technologies are currently available for noninvasive body sculpting/contouring, including HIFU, 45 cryolipolysis, 6 and radiofrequency; 46 however, the mean BMI of subjects in these studies was <30 kg/m2. Subjects undergoing treatment with HIFU commonly experience mild or moderate procedural pain and ecchymosis. 45 Although cryotherapy appears to be better tolerated, most subjects in one study reported minimal to tolerable procedural discomfort. 47 To date, there have been no reports of adverse events in any subject undergoing treatment with LLLT for body sculpting. 8 –10,18,44 It is also important to note that the endocrine functions of adipose tissue are preserved since LLLT does not cause adipose necrosis. 32 The mean decrease in waist circumference achieved by subjects across LLLT studies compares very favorably with other noninvasive treatment modalities, especially when considering its outstanding safety profile.
Based on these results, this LLLT device (Erchonia® SHL Laser; Erchonia Corporation) was approved by the U.S. Food and Drug Administration on October 21, 2014, for use as a noninvasive dermatological esthetic treatment for reduction of circumference of hips, waist, and upper abdomen when applied to individuals with a BMI between 30 and 40 kg/m2.
Conclusions
Subjects with BMI between 30 and 40 kg/m2 were treated with LLLT or sham treatment twice weekly for 3 weeks. Among subjects treated with the LLLT device, 71.43% attained a ≥3.0 inch decrease in combined circumference measurements versus 12% of sham-treated subjects. The overall mean decrease in combined circumference measurement for subjects treated with the LLLT device was 10.52 cm versus 1.80 cm for sham-treated subjects. There were no adverse events. Decreasing the amount of fat stored in adipocytes may have substantial health benefits in obese individuals.
Footnotes
Acknowledgments
This study was sponsored by Erchonia Corporation, McKinney, TX. The authors acknowledge the careful review by Stephanie Shanks, the editorial assistance of Dr. Carl S. Hornfeldt, Apothekon, Inc., and the statistical support of Elvira Walls, Regulatory Insight, Inc.
Author Disclosure Statement
No competing financial interests exist.