
Abstract
Introduction
S
It is known that conventional root canal preparation and irrigation solutions cannot securely eliminate remaining bacteria effectively, as microorganisms are capable of colonizing the dentinal tubules up to 1000 μm, 1 whereas conventional irrigation solutions due to their surface tension penetrate only about 100 μm into dentin. 2
To aid the disinfecting procedures, different laser wavelengths have been introduced for endodontic purposes during the past years. Near-infrared laser light may reach relatively deep dentin layers, up to 1000 μm. This special group of lasers shows a very different effectiveness on bacterial kill in root canals. 3 –5 Despite the fact that the laser intensity exponentially decreases at deeper layers of the tissue, hydroxyapatite prisms and dentinal tubules may act as light conductors, so despite weakened laser light, the bactericidal effect is maintained. 6 –8
The Nd:YAG laser, due to its high penetration depth, was introduced to endodontology as early as in the 1990s, 9 –11 followed soon after by Diode and Erbium Lasers, which also proved to have bactericidal capacity in the root canal as well. 12 –14
Diode lasers are applied in a range of wavelengths between ∼600 and 980 nm. Especially the antibacterial ability of 810–980 nm has been extensively investigated. It was demonstrated that not only the wavelength is responsible for the efficacy but also the integration of the access cavity into the irradiation protocol markedly added to the improved results. 4 Recent studies have demonstrated that there is a good bactericidal effect of the wavelength 980 nm. 15,16 Different optic fiber designs are being investigated for the potential to increase the efficiency of the 980 nm diode laser irradiation. 16 The mentioned studies have all used the chopped mode. 4,15,16
It has to be stated that characteristics of pulsed lasers (CO2, Nd:YAG) are not suitable for diode lasers as they operate in a continuous or chopped mode only. There is a persisting incongruity in the nomenclature that the diode laser works in the “pulsed mode.” Accordingly, the “micropulsed mode” represents gated chopped mode or microchopped mode. A diode laser's microchopped mode is an intermittent sequence of pulse complexes, and the maximum output is always equal to the nominated output of the device. Although the wrong expressions are widely used, we stick to the correct terms in this article.
As diode lasers present a lower penetration depth into dentin compared to Nd:YAG lasers, a reduced risk of unwanted temperature increase in the periradicular tissues is expected. 17
Our null hypothesis is that the modified chopped mode (microchopped mode) in a Diode 980 nm laser will not induce any risk of thermal impact to the root surface.
The aim of this article was to investigate the temperature increase of the external root surface during simulation of laser-assisted endodontic treatment using a diode laser (980 nm) in a microchopped mode.
Materials and Methods
The study used 10 human, freshly extracted maxillary incisors, collected from a dental clinic in Vienna. The study was approved by the Ethics commission of the University of Vienna, Austria (EK Nr: 1386/2012).
Immediately after the extraction, the surfaces of the teeth were cleaned with ultrasonic bathing and 3% hydrogen peroxide and stored in sterile saline (0.9% NaCl solution) at a temperature of 5°C until used. Then, endodontic access cavities were prepared with an Endo Access Bur (Dentsply Maillefer), and an Endo Z bur (Dentsply Maillefer), using a high-speed handpiece. After the preparation of the coronal third with Gates Glidden burs (#1, #2, and #3) up to 2 mm beyond the cementoenamel junction, the working length was determined as 1 mm less than the actual length of the tooth. The root canals were prepared with ProTaper files (Dentsply Maillefer) up to size F4, according to the manufacturer's protocol.
The specimens were numbered from 1 to 10. Each tooth was treated according to all treatment schemes (irradiated with all four laser settings) in ascending powers. The output power was recorded by a measurement head (model 10AFS; Ophir Optronics).
During irradiation, the teeth were mounted in a holder. Irradiation was performed with a 980 nm InGaAs diode laser (GENTLEray 980 Classic Plus; KaVo) using a 200 μm fiber (Fig. 1).

Tooth mounted on a holder during laser treatment.
In all cases, the irradiation schemes applied consisted of six cycles: 5 sec of irradiation, followed by a pause of 20 sec. The fiber was inserted into the wet root canal at working length, and irradiation was started. The fiber was moved in a coronal direction, at a rate of approximately 3 mm/sec, utilizing a spiral movement to avoid hot spots. 12 Teeth 1 to 10 were handled according to the same sequence during the experiment. After the application of one treatment scheme, the teeth were irrigated with 5 mL sterile saline and embedded in 0.9% NaCl until the application of the next treatment scheme to allow rehydration and cooling down to room temperature (22°C). Also, following the completion of each treatment scheme for a given specimen, the tip of the optic fiber was cut off with the appropriate ceramic tweezers provided by the manufacturer, so a new tip would serve the next treatment.
The study involved four treatment schemes (Table 1).
In Group 1 (control), representing the actual standard of endodontic laser-assisted treatment, the root canal was irradiated in the chopped mode. We applied 2.5 W output power, 25 ms on/25 ms off, resulting in 1.25 W average power. Group 2 utilized a microchopped mode, using 1.6 W average power during the pulsetrains, which resulted in an overall average power of 0.8 W. Group 3 used 2.0 W average power during the pulsetrains (Ø 1.0 W), and Group 4 had 2.5 W (Ø 1.25 W) average power during the pulsetrains.
The microchopped mode utilized pulses of only 25 μs, grouped in “bursts” of 25 ms. The pulse power was 12 W. The average power was modified by varying the pulse breaks within the “pulsetrains” (Fig. 2).
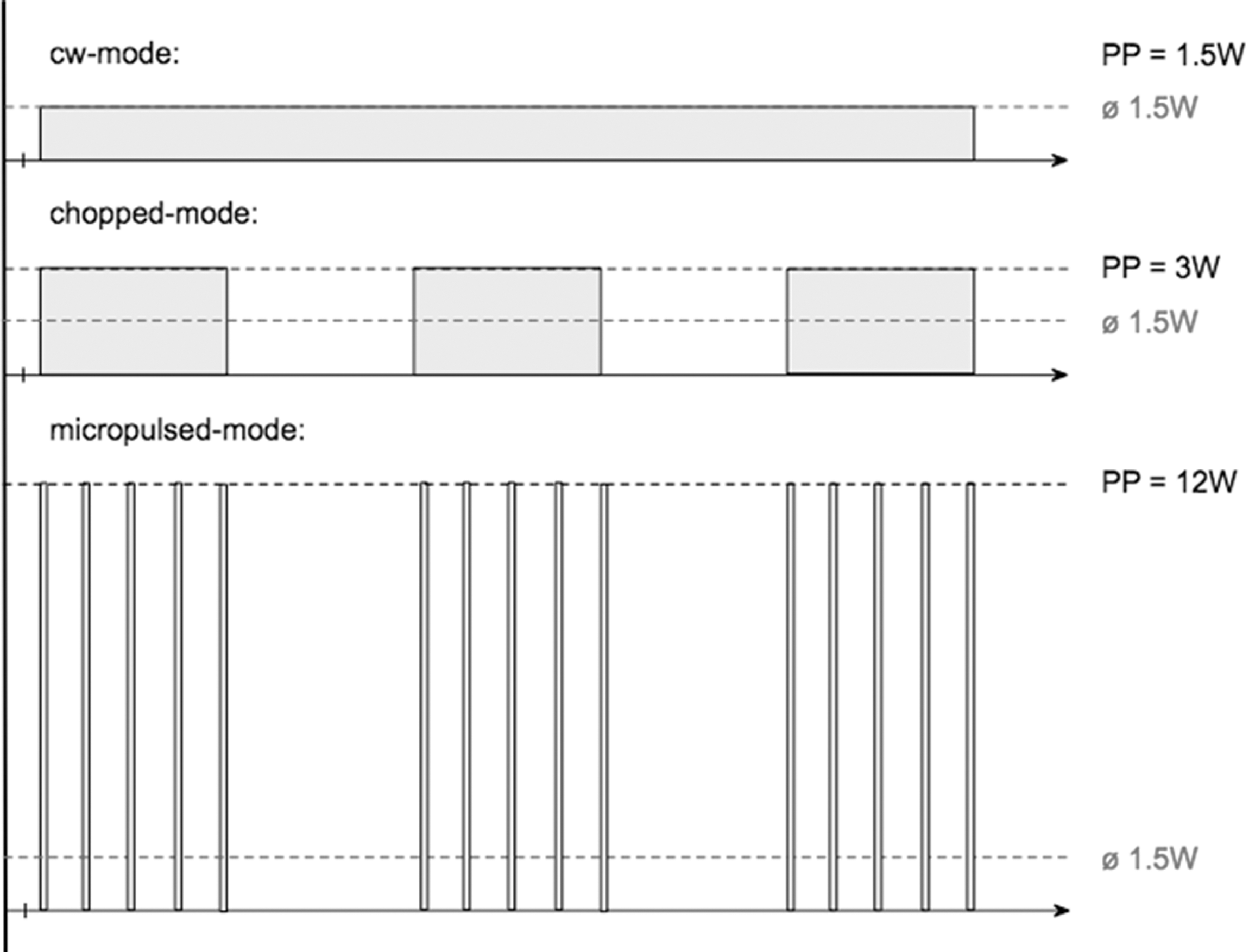
The effect of chopped and microchopped mode in diode lasers on the average power; an example.
A single experienced operator (blinded concerning the applied parameters) performed all procedures and the device was calibrated before each power setting was applied.
The temperature changes were documented with an infrared camera (EC 060; Trotec, Heinsberg, Germany) during all procedures. Measurements were always taken from the same three spots (apical, medial, cervical third) to enable a reproducible comparison of the four irradiation settings, despite different root morphologies and different thicknesses of the root canal walls. The temperature was measured at the approximal root surfaces with the least dentin thickness, and therefore, we expected the highest temperature increase there. 18 –20
Statistical tests
For the variable “temperature difference,” mean and standard deviation per Group (1–4) and reading point were calculated for the valid number of samples (n = 30).
Data were depicted using boxplots, bar charts, and time line curves. Measurements were taken at preassigned points in time (after 0, 5, 25, 30, 50, 55, 75, 80, 100, 105, 125, 130 sec). Single time line curves as well as mean curves were analyzed.
To determine temperature differences between groups we used a mixed model (ANOVA for repeated measurements). The depending variable was the difference between baseline (0 sec) and final value (130 sec). Independent variable was the factor “measuring spot.” Random factor was the “tooth.”
Statistical significance was defined at p < 0.05.
As the groups showed statistically significant differences, we applied pairwise post hoc t-test using the Bonferroni correction.
Results
Data analysis with ANOVA for repeated measurements has revealed a mean temperature increase of 1.06°C in Group 1, 1.57°C in Group 2, 1.74°C in Group 3, and 1.93°C in Group 4 (Table 2).
As temperature was measured in three spots n = 30.
Assuming a sphericity of the data, the groups showed a significant difference of p = 0.041. If the sphericity of the data was contaminated, although the applied Mauchly Test suggested a data congruency, we referred to the Greenhouse-Geisser correction, which also demonstrated a significance of p = 0.048. 21
Looking at the temperature development, grouped after the location, the study showed the lowest temperature increase in the cervical third (0.79°C ± 0.22°C), followed by the apical third (1.88°C ± 0.22°C), and the highest in the medial third (2.05°C ± 0.22°C). The post hoc t-test with the Bonferroni correction resulted in a significant difference between Group 1 and 4 (p = 0.007); the difference in temperature increase was 0.87°C. Between Groups 1 and 3 a significant difference in temperature increase was found to be 0.51°C (p = 0.035). Between Groups 1 and 2 we noted a marginally significant difference (p = 0.052).
No statistically significant differences were observed within the microchopped groups (Groups 2–4).
Despite the mean temperature increase and the standard deviations reported, intermediate temperature peaks were observed. The highest temperature increase was measured in tooth 1, treatment Group 2, at the middle third (+5.7°C).
The null hypothesis was verified.
Discussion
The use of laser technology in endodontic therapy has been widely investigated. Although the wavelengths of diode lasers (805–980 nm) are not perfectly fitting to the single tissue components (absorption from hydroxyapatite, water, dentin, and enamel), 22 they offer quite a suitable medium in its entirety, which is widely accepted in dental indications. 4,5,12,23 –25
It has been demonstrated that diode lasers provide satisfactory bactericidal effects and reach deep dentin layers (up to 500 microns) during treatment. 26 The usually applied standard settings using a diode laser are 2.5 W in the chopped mode. 20,27
The present in vitro study investigated if the manufacturer's suggested settings are safe, temperaturewise, for endodontic disinfection.
An infrared thermography system was chosen to monitor the temperature rise instead of a thermocouple method, because the monitoring of temperature changes is possible for rather a large surface area. The real-time thermal video image has the advantage of image analysis by the integrated software, allowing the identification of maximum temperatures at different points. 28
In literature, the safety threshold for temperature increase on the root surface is reported to be within the range of 7°C–10°C. 19,29 Otherwise, ankylosis may occur as a result of the thermal trauma to the surrounding periodontal tissues. 30 In this study, the maximum recorded temperature increase was 5.7°C, but the average temperature rise was below 2°C in all groups (Figs. 3 and 4); therefore, it may be assumed that the application of this microchopped mode is safe in laser-assisted endodontic therapy.
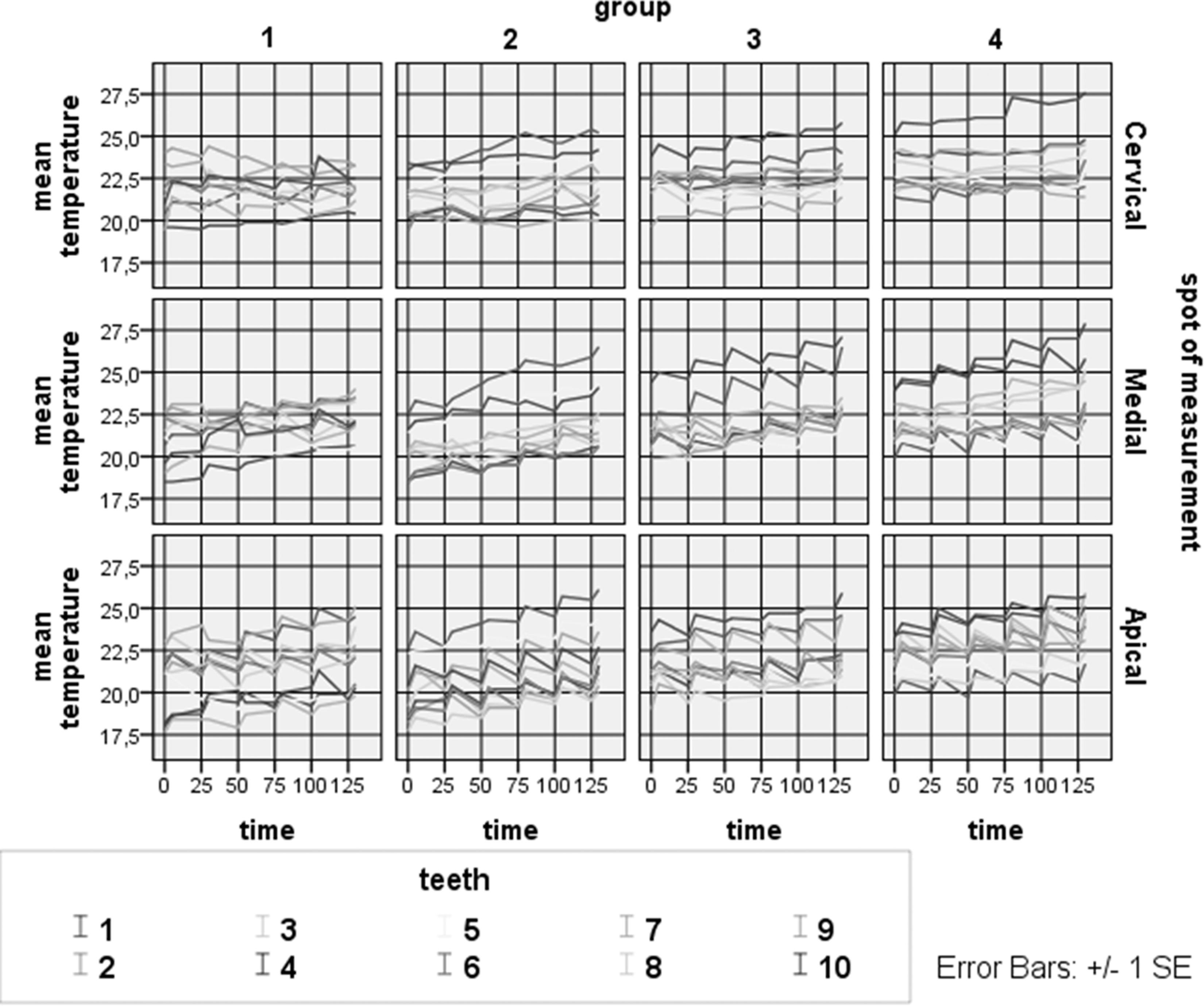
Individual temperature development in each tooth during the treatment applying the four different schemes.
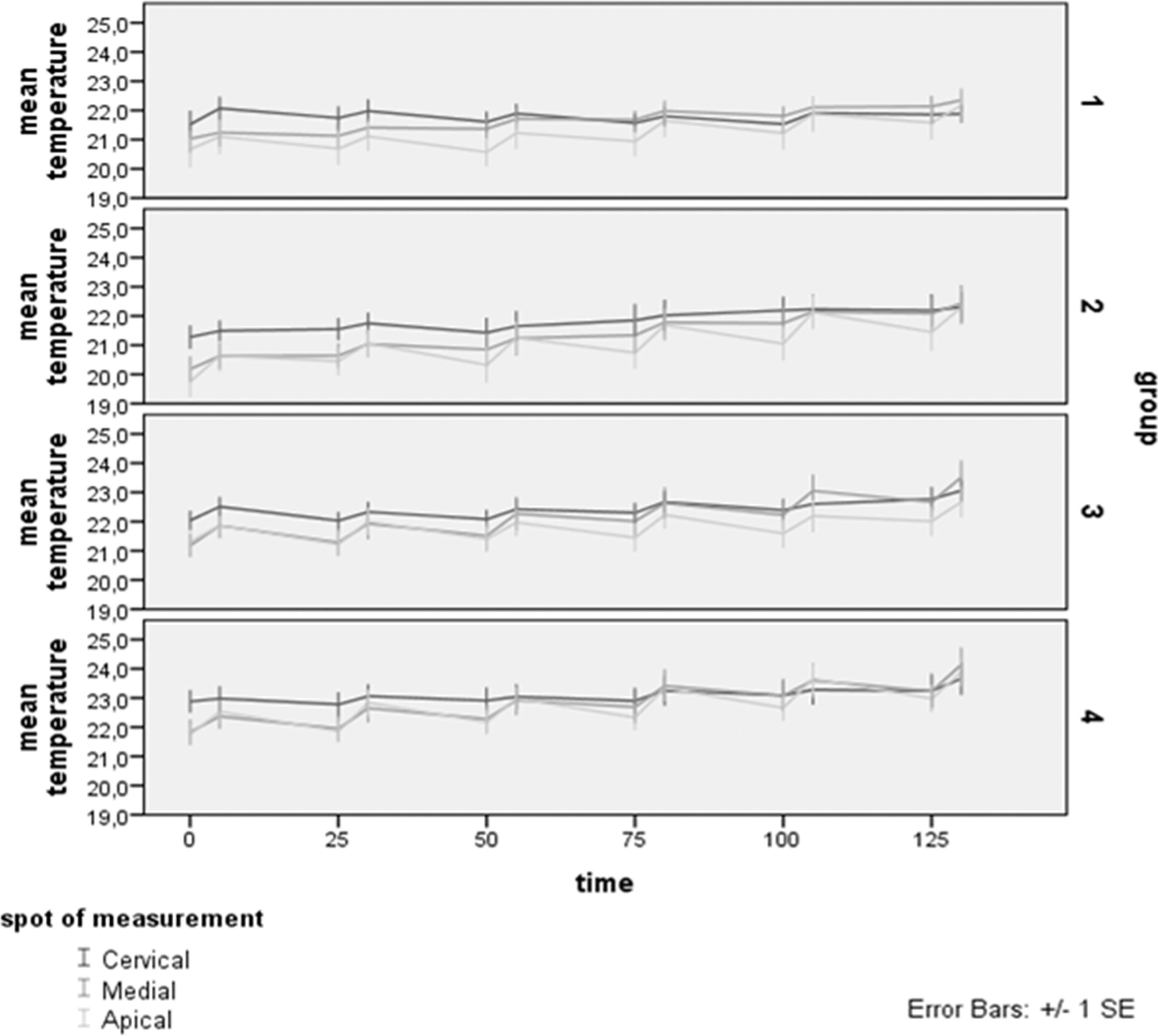
Mean temperature rise in the three thirtiles of the teeth.
Strakas et al. reported that the average temperature elevation for two different pulse durations on the root surfaces during laser-assisted endodontic treatment with a Nd:YAG laser was less than 9°C, but the actual maximum temperatures recorded in the study exceeded the safety threshold by far. 31
An extensive literature review revealed ∼35 articles concerning the temperature rise on the external surface of the root during laser-assisted Endodontics. Ten of them are on diode lasers. Interestingly enough, only one revealed the maximum recorded momentary temperature rise (11°C), with an average of 2.43°C (SD 0.774). 32 The aforementioned observation leads to the conclusion that not all proposed protocols in literature may be safe for clinical application as the rest of the articles refer on the mean and the standard deviation of the temperature rise. Thus, the message is alerting, as the mean temperature rise does not guarantee that the parameters used restrict the elevation within safety limits. As Heysselaer et al. rightfully reported, the use of diode laser in root canal treatments may be harmful for periodontal tissues if the irradiation conditions are not strictly respected. 33
Beer et al. demonstrated in an in vitro study that the cutting efficacy of a 980 nm diode laser was increased when the microchopped mode was applied. The microchopped mode—applied with the same average power as the chopped mode—results in a larger pause-to-pulse ratio, thus permitting sufficient thermal relaxation of the irradiated tissue. In addition, the collateral tissue damage was reduced when compared to the chopped mode. 23,34 In our case, the performance of wet canal irradiation and the sufficient resting time in between each cycle of laser application seem to be in favor of tissue thermal relaxation as supported by the reported results, temperaturewise.
During the experiment, specimens were kept in a holding device and were surrounded by air, thus the clinical conditions were not completely simulated. Periodontal tissues, as well as bone, possess much better thermal conductivity. Air ranges at 0.02 W/mK, bone at 0.16–0.34 W/mK, and blood at 0.62 W/mK. 35,36 This allows the presumption that the temperature rise in vivo will be even lower, because the tissues surrounding the tooth are much better able to dissipate heat. In addition, it can be expected that tissue temperatures around 40°C (corresponding to our measured temperature increase) will result in a certain vasodilatation with following enhancement of heat dissipation. 37,38
Under the conditions of the experimental setup, it was observed that the temperature rise was higher in the apical and medial thirds of the roots. This might be due to the fact that the dentin is thinner in these areas. According to the modified Beer–Lambert law and diffusion theory, the laser intensity exponentially decreases at deeper layers of the tissue. Thus, the resulting temperature at the root surface is directly depending on the dentin thickness. This was also the reason why the temperature was measured at the proximal root surface, as dentin walls are expected to be thinner. 18,39 Dentin thickness has shown to have a significant effect on intrapulpal temperature changes with a thinner dentin layer resulting in higher temperature elevations. 40 Caution must be taken in cases of roots with very thin approximal walls, for example, lower incisors.
The slight variations in temperature rise within the groups might be due to manual guidance of the fiber. An automatically driven movement of the laser fiber could exclude the bias of this shortcoming in the laser application.
It will be worth investigating the influence of diode laser irradiation in the microchopped mode on dentin composition and morphology, as suggested by Esteves-Oliveira et al. 41 It is very likely that the morphological changes correlate with the laser settings temperaturewise. 42,43 In addition, the bactericidal effect of these settings needs to be evaluated before adaptation in any clinical protocol. 26
Conclusions
Under the conditions used and within the limitations of the study, the microchopped diode laser irradiation is a safe possible treatment option in laser-assisted endodontic treatment, concerning the temperature elevation on the external root surface.
Compliance with Ethical Standards
Ethical approval: This article does not contain any studies with human participants or animals performed by any of the authors. The study was approved by the Ethics commission of the University of Vienna, Austria (EK Nr: 1386/2012), for the use of human extracted teeth.
Informed Consent
Informed consent was obtained from all individual participants whose teeth were included in the study.
Footnotes
Author Disclosure Statement
No competing financial interests exist.