
Abstract
Introduction
D
A study of ∼32,000 postmenopausal women in the United States reported a 12-fold greater incidence of hip fractures in women with TIDM compared with those without TIDM. 7 Intensive insulin therapy has led to reductions in microvascular complications along with increased lifespan in patients with TIDM. Therefore, the need exists to shift the focus from microvascular complications to OP in patients with TIDM. 8
Although tremendous advancements have occurred for systemic OP outcomes, management of fragility fractures in osteoporotic bone remains clinically challenging. Fracture nonunion is a consequence of low initial bone density and prolonged healing response. Local treatment strategies can be used to prevent fractures and accelerate healing by locally stimulation of anabolic pathways or inhibition of catabolic pathways. 9
Photobiomodulation is a term broadly applied to the therapeutic effects of lasers. Clinical applications of laser biostimulation are growing rapidly. 10 Several studies have highlighted the osteogenic effects of pulsed wave (PW) laser on osteoblasts both in vitro and in vivo. 11 –13 Other researchers observed that PW laser improved certain musculoskeletal disorders in both patients and animals. Chang et al. reported that lasers with specification of 10 Hz, 60 mW, 9.7 J/cm2, and 830 nm not only effectively alleviated pain and symptoms but also improved the functional ability of finger and hand strength for individuals with mild and moderate carpal tunnel syndrome. Patients reported with no adverse effects. 14 Studies from the corresponding author's laboratory showed beneficial effects of PW laser on osteochondral and bone defects. 15,16 We used the biomechanical three-point bending test in these studies. 15,16
Computed tomography (CT) and other recent improvements to imaging techniques have made it possible to evaluate the healing process by measuring the Hounsfield unit (HU) of bone tissue. 17,18
To the best of our knowledge, no study investigated the effects of photobiomodulation on biomechanical properties and the HU of the callus area after a partial tibial osteotomy in streptozotocin (STZ)-induced TIDM and ovariectomized- induced OP (OVX) rats. We intended to assess the effects of photobiomodulation on the HU and biomechanical properties in the callus area of a partial osteotomy in an experimental female rat model of TIDM and OP.
Materials and Methods
Animals and study design
In this study, we divided 30 adult female Wistar rats, 4 months of age (∼210 g), into the following groups: (1) ovariectomy (OVX) control with no TIDM and no PW laser, (2) OVX+PW laser and no TIDM, (3) OVX control+TIDM, (4) OVX+TIDM+PW laser, (5) OVX+TIDM+alendronate (3 mg/kg), and (6) OVX+TIDM+PW laser+alendronate. Rats received food and water ad libitum and were weighed on a weekly basis throughout the study. First, we induced TIDM in rats from groups 3–6. Next, all rats underwent total OVX (Fig. 1). A partial transversal standardized osteotomy was made with a drill in the right tibias of all rats. Next, we treated the tibias of rats from groups 2, 4, and 6 with an infrared PW laser (Fig. 2). At 30 days after surgery, the rats were sacrificed and their right tibias were submitted to CT scanning, in addition to a three-point bending test to evaluate HU and bone strength (Fig. 3), respectively. Table 1 shows the study design. The Medical Ethics Committee at Shahid Beheshti University of Medical Sciences, Tehran, Iran, approved the study protocol (no: 1393-1-91-13237).
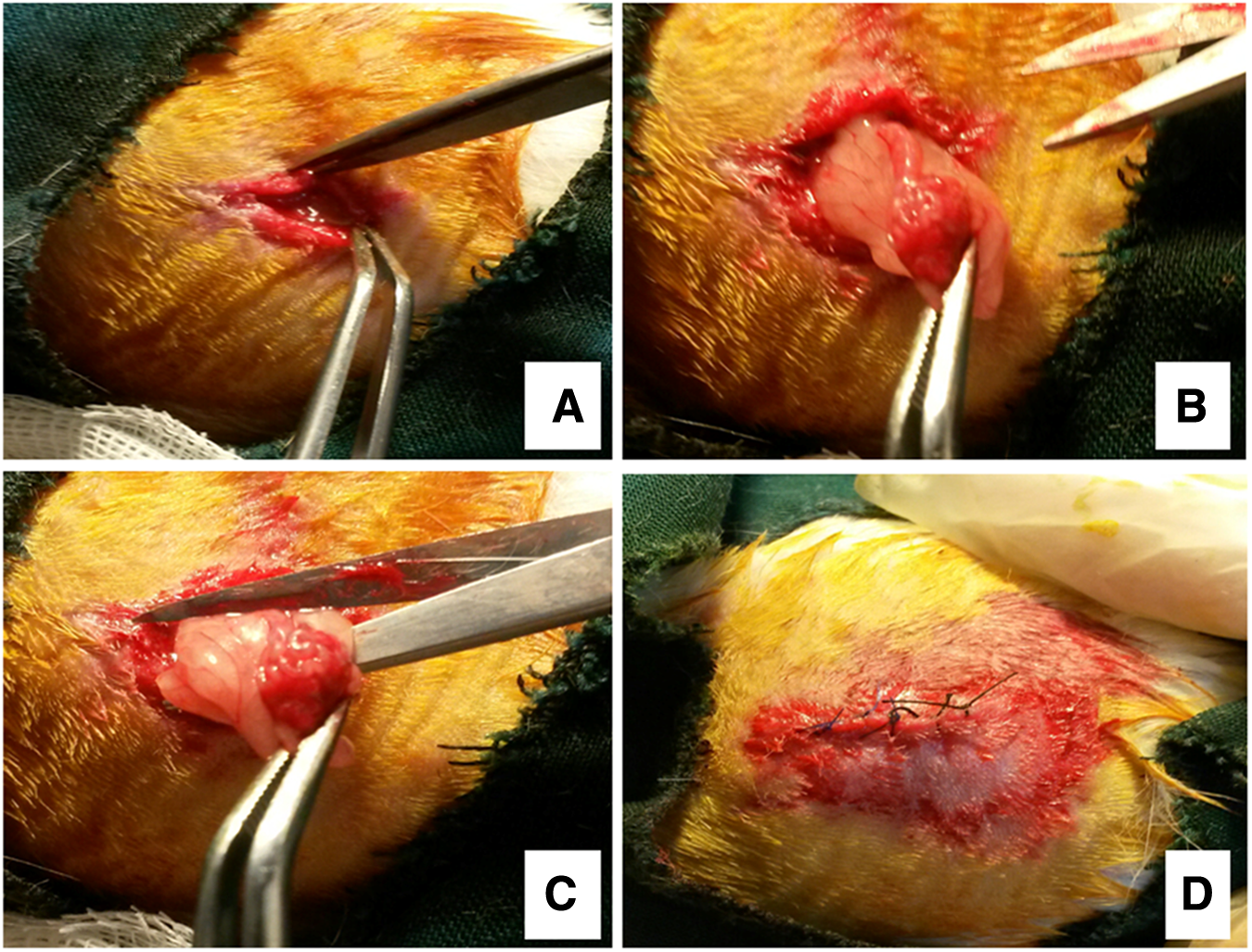
Ovariectomy steps. Images show the incision
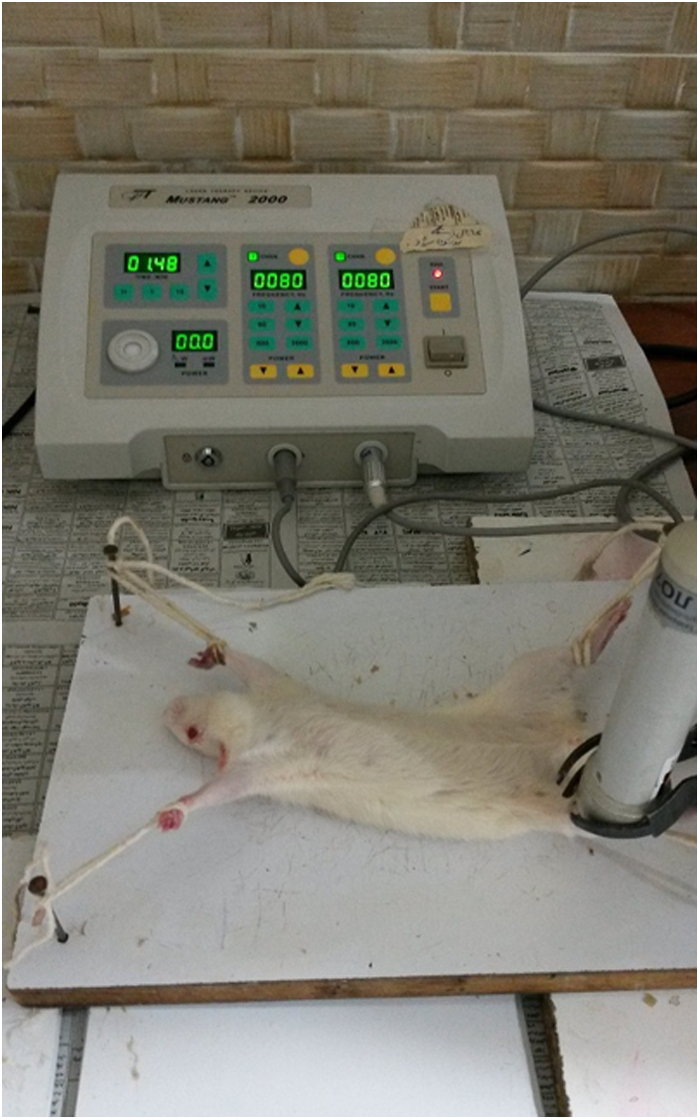
Laser irradiation technique.
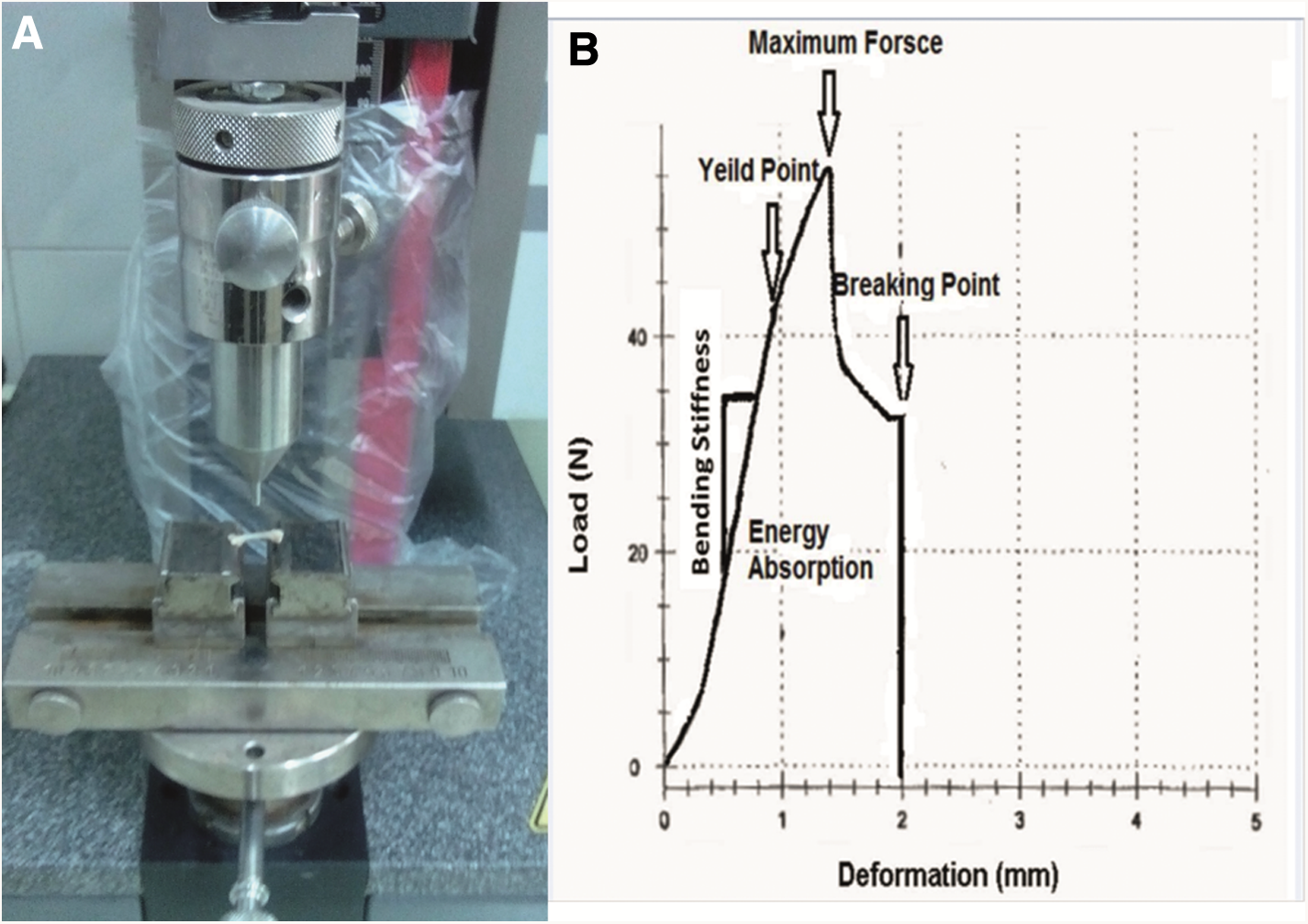
Three-point bending test instrument
CT, computed tomography; OVX, ovariectomy; PW, pulsed wave; TIDM, type I diabetes mellitus.
Induction of TIDM
Each rat from groups 3–6 received an intraperitoneal injection (40 mg/kg body weight) of STZ (Enzo Life Sciences, Inc., Farmingdale, NY) freshly dissolved in sterile distilled water. 19 TIDM was defined as a blood glucose concentration greater than 250 mg/dL in a tail vein blood sample (Gm 300; Bioneme, GmbH, Switzerland) 7 days after the STZ injection. 20 We monitored blood glucose levels and body weights weekly throughout the study. All diabetic rats were maintained for 30 days after administration of STZ. 16
Ovariectomy
All rats underwent total OVX. On day zero, or the surgery day, we anesthetized each rat with a dose of ketamine (50 mg/kg) and diazepam (5 mg/kg). We inflicted two paravertebral skin incisions and ligated the uterine tubes. After the ovaries were removed, we sutured the incisions (Fig. 1). Each rat received ceftriaxone (50 mg/kg, Jaber ben Hayan, Iran) injections, as antibiotic therapy, before the surgery and 24 and 48 h after surgery. 21 For relief of postoperative pain, the rats received 20 mg/kg ibuprofen (Emaddarmanpars Co., Tehran, Iran) before surgery, then, every 8–12 h for 5 days after surgery. 22 All animals were kept for 60 days after surgery in cages to develop OP. At the end of this period, the rats were submitted to CT scanning for confirmation of OP. Next, each rat underwent a partial osteotomy in the right tibia (Fig. 1).
Partial transversal standardized osteotomy
Under general anesthesia and sterile conditions, the skin of each rat's right leg was cut longitudinally just below the knee on the medial side. A circular partial transversal standardized osteotomy, deep to the central medullary canal, was created with a low-speed drill (terminal, 1.5 mm diameter; Delab; Dental Fabriktreffurt, Germany) and simultaneously irrigated with sterile water to avoid burning (Fig. 4). Next, the muscles were sutured with CG03; the skin was sutured with 04 nylon reversed cutting sutures. Rats received ceftriaxone as antibiotic therapy. 16
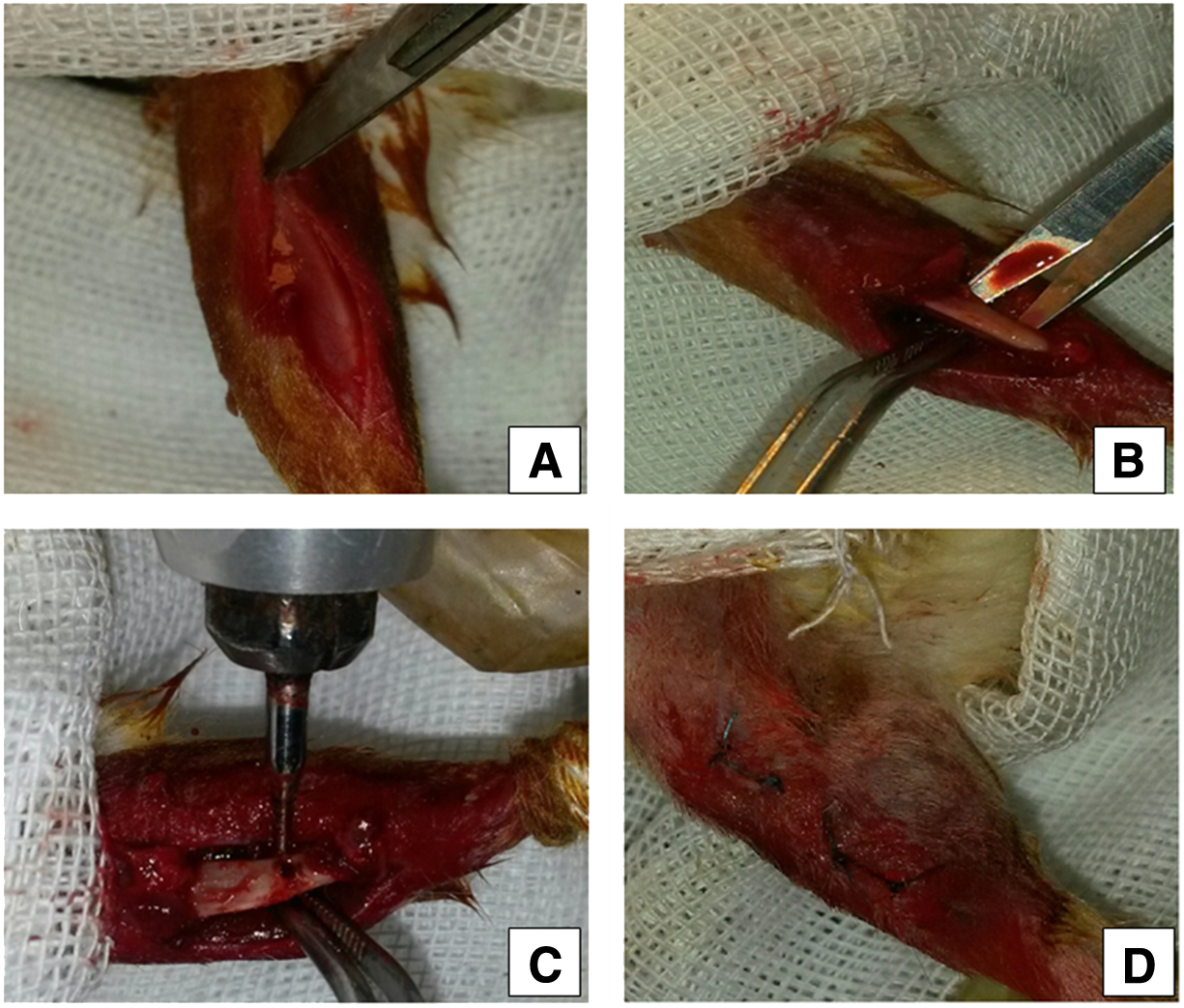
Steps in the partial transversal standardized osteotomy. Image shows the incision
PW laser and alendronate administration
We used an infrared PW laser (Mustang 2000; Technical Co., Moscow, Russia) with the specifications listed in Table 2. The PW laser protocol of the current study was applied successfully. 23 PW laser was performed on the right tibia three times per week for 30 days for a total of 14 sessions. Day 1 was considered the onset of PW laser treatment. Laser-treated rats' right tibias were completely irradiated by three laser shoots, while the laser pen was held perpendicular to the bone from a distance of <1 cm. The first laser shoot was performed on the bone defect, whereas the second was administered at a distance of 1 cm proximally from the center of the bone defect. The third laser was performed at a distance of 1 cm distally from the center of the bone defect (Fig. 2). 23 Rats from groups 5 and 6 received subcutaneous injections of 3 mg/kg alendronate (Alborz Darou Co, Iran) for 30 days. At 30 days after the beginning of the treatments, all rats were euthanized with an overdose of the anesthesia, and we removed their right tibias. We assessed the bone for HU, followed by a biomechanical examination.
ED, energy density.
CT scanning
First OP development of STZ+OVX rat tibias were evaluated qualitatively by CT scan using multi slides (kv = 100, ma = 50, sections = 2 mm, FOV = 240 mm; Toshiba, Aquilion 16, Japan) compared with healthy rats 2 months after OVX. Tibial bone density was determined while the rats were under general anesthesia. The callus densities of the bone defects were determined 30 days after partial osteotomy and immediately after the rats were euthanized (Fig. 4). A technician tested all tibias and calluses. Bone densities and callus densities were reported in HU. The technician was unaware of the study group assignments (Fig. 5). 18
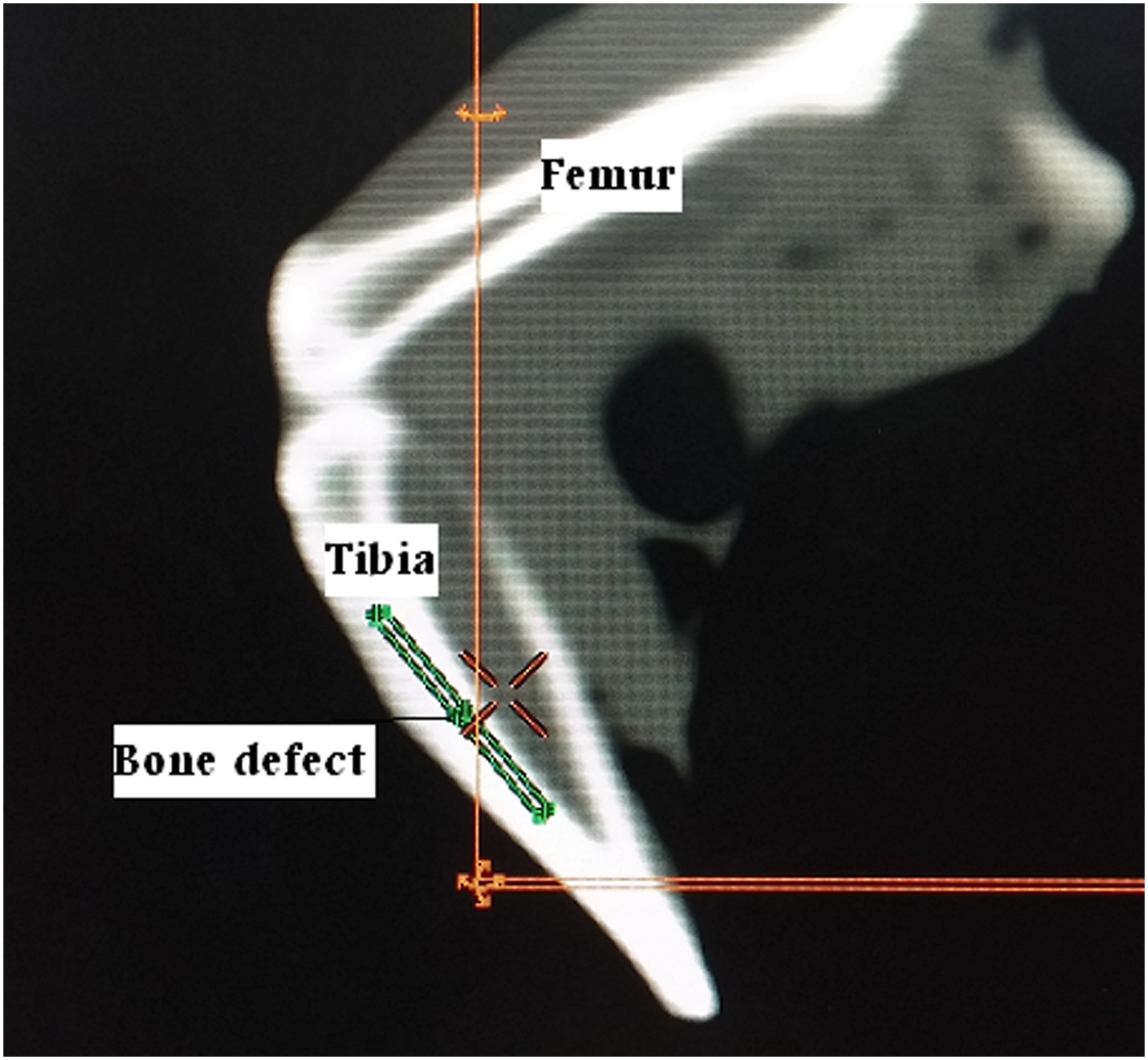
Computed tomography scan from the right hind limb of a rat. There were Tibia and femur.
Three-point bending test
We examined the biomechanical properties of five tibias in each group. The tibias were subjected to the three-point bending test by a material testing instrument (Zwick/Roell Group, Z 2.5 H 15WN, UIm, Germany) until fracture. Two loading points were used to support the tibia and a press head was subsequently activated to compress the midline of the bone shaft until a fracture occurred (Fig. 1A). The press head speed was 0.08 mm/sec for all tests. Data were recorded to the material testing instrument from the load-deformation curve (Fig. 1B), and we calculated the following biomechanical properties: bending stiffness (N/mm), maximum force (N), stress high load (N/mm2), and energy absorption (N mm) (Fig. 3). 24
Ne tissue
Statistical analysis
We used the paired Student's t-test to analyze the first and last blood glucose levels and first and last body weights. The tibia HUs from the STZ+OVX rats and healthy rats were compared by the independent sample Student's t-test. Data are expressed as mean ± standard deviation. Normal distribution of biomechanical properties and callus density data were evaluated by the one-sample Kolmogorov–Smirnov test. Analysis of variance (ANOVA) compared the changes between groups, while we used the least significant test (LSD) to identify the differences. A p-value of <0.05 was considered statistically significant.
Results
General observations
A total of 10 out of 20 rats from groups 3–6 developed clinical evidence of diabetes after the STZ injection. Of the remainder, eight failed to show clinical evidence of diabetes and two died. Consequently, they (10 nondiabetic rats) were replaced. Diabetic rats from groups 4–6 had significantly decreased body weight at the end of the study (Table 3).
Paired Student's t-test showed decreases in body weights of rats from groups 2 and 6.
p < 0.01, ** p < 0.001.
PWLLLT, pulsed wave low-level laser therapy.
HU analysis
The Student's t-test analysis showed that a significant decrease existed in tibial bone density in the STZ + OVX rats (678.6 ± 50.6 HU) compared with the healthy control group (743.8 ± 24.8 HU; p = 0.032).
ANOVA for callus density HU was p = 0.000. There was a significant increase in mean callus density in group 6 (OVX + TIDM + PW laser+alendronate) compared with groups 2 and 3 (LSD test, both p = 0.000). Our result showed a significant increase in the mean callus density in group 4 (OVX + TIDM + PW laser) compared with the control diabetic group (p = 0.000). The mean callus density of group 2 (OVX + PW laser, no TIDM) significantly decreased compared with the healthy control group (p = 0.007). Figure 6 shows the results.
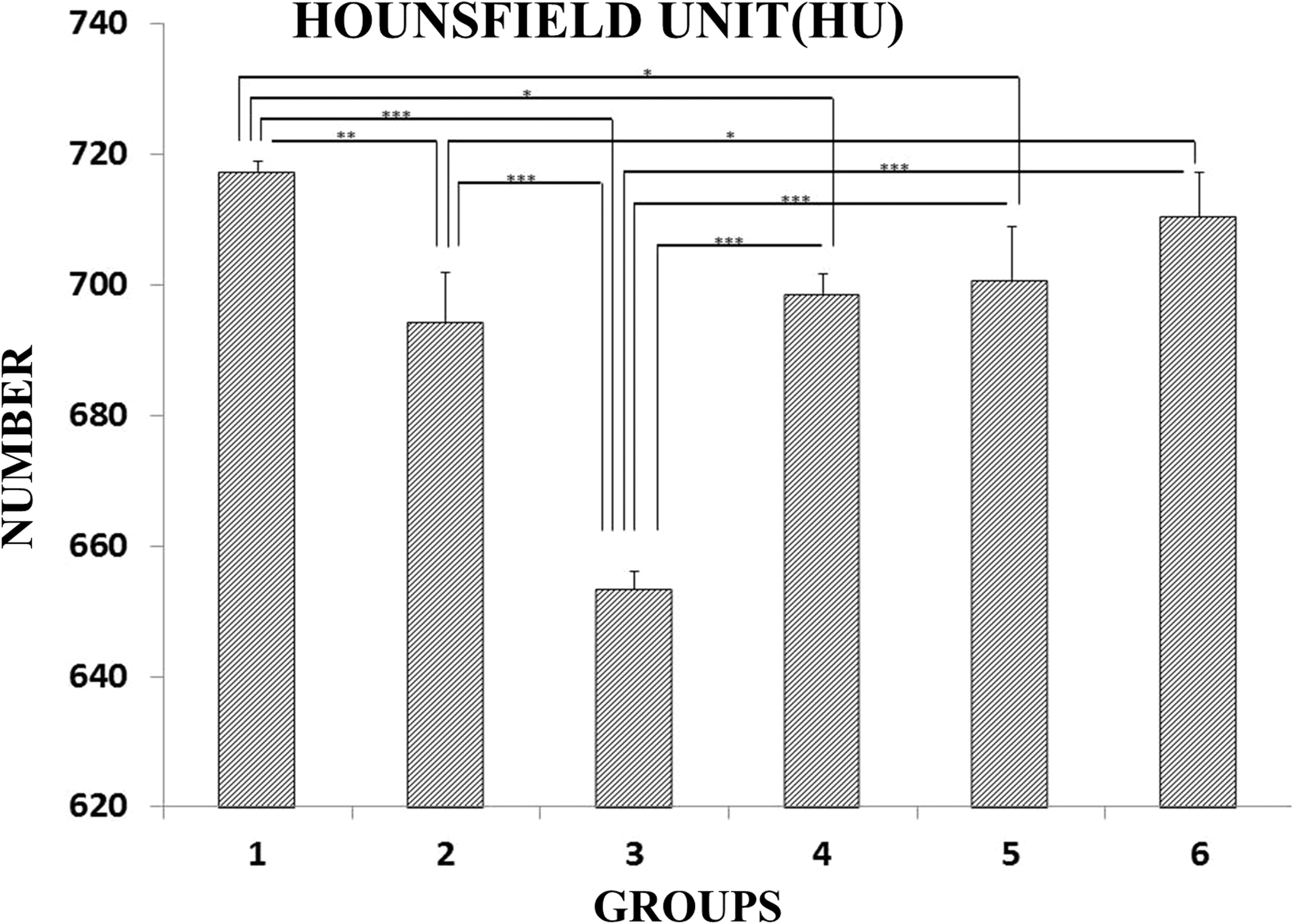
Mean ± standard deviation of HU in the study groups according to ANOVA. Group 1: OVX control, no TIDM, and no PW laser; group 2: OVX + PW laser and no TIDM; group 3: OVX control + TIDM; group 4: OVX + TIDM + PW laser; group 5: OVX + TIDM + alendronate; and group 6: OVX + TIDM + PW laser + alendronate. *p < 0.05; **p < 0.01; ***p < 0.001. ANOVA, analysis of variance; HU, Hounsfield unit; OVX, ovariectomy; PW, pulsed wave; TIDM, type I diabetes mellitus.
Three-point bending analysis
Figures 7 –10 show that the combined application of PW Laser and alendronate significantly increased important biomechanical properties for repair of the partial osteotomy of the tibia in STZ + OVX rats compared with the healthy and diabetic control groups.
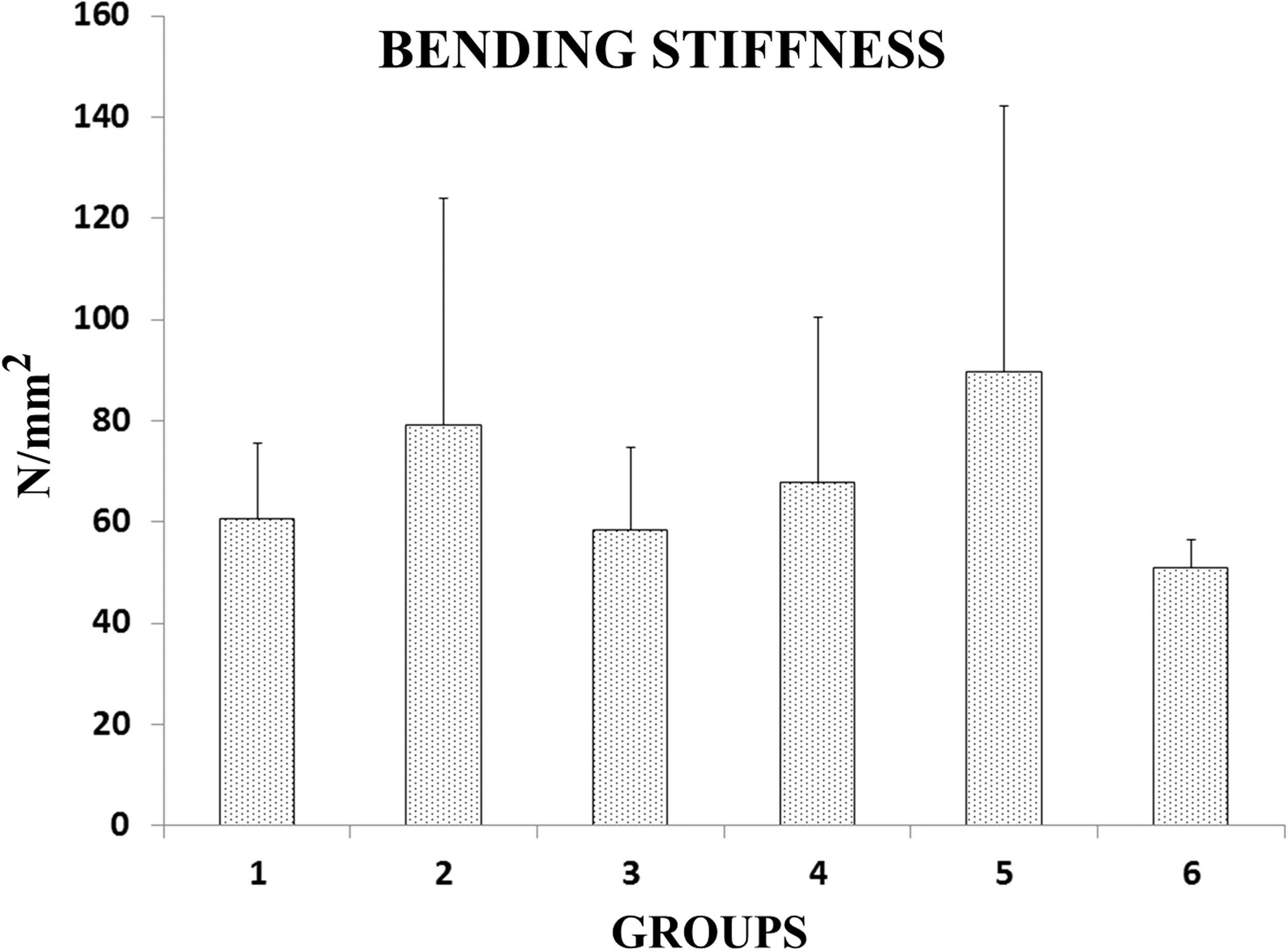
Mean ± SD of bending stiffness in the groups compared by ANOVA.
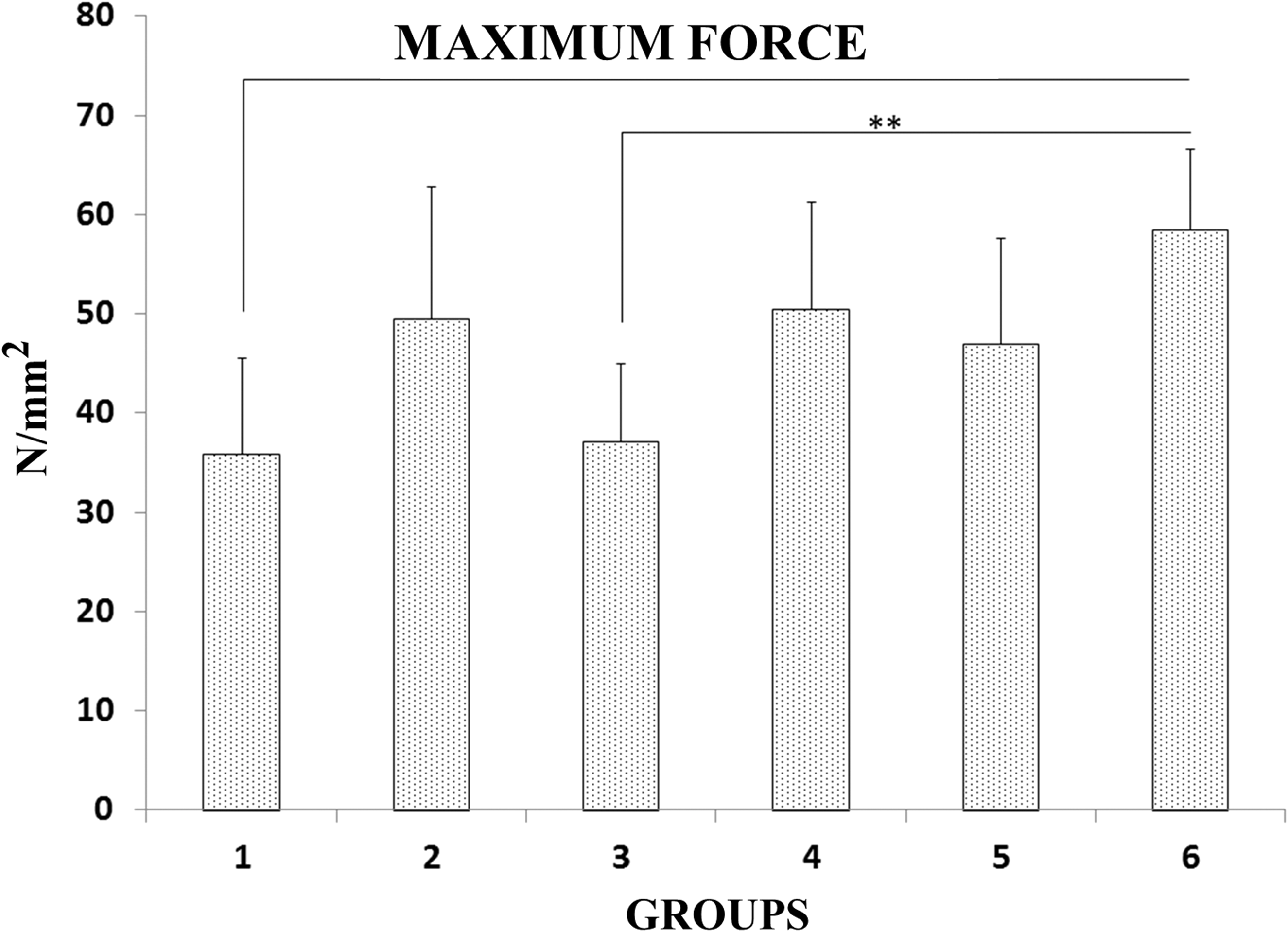
Mean ± SD of maximum force in the groups compared by the LSD test. **p < 0.01.
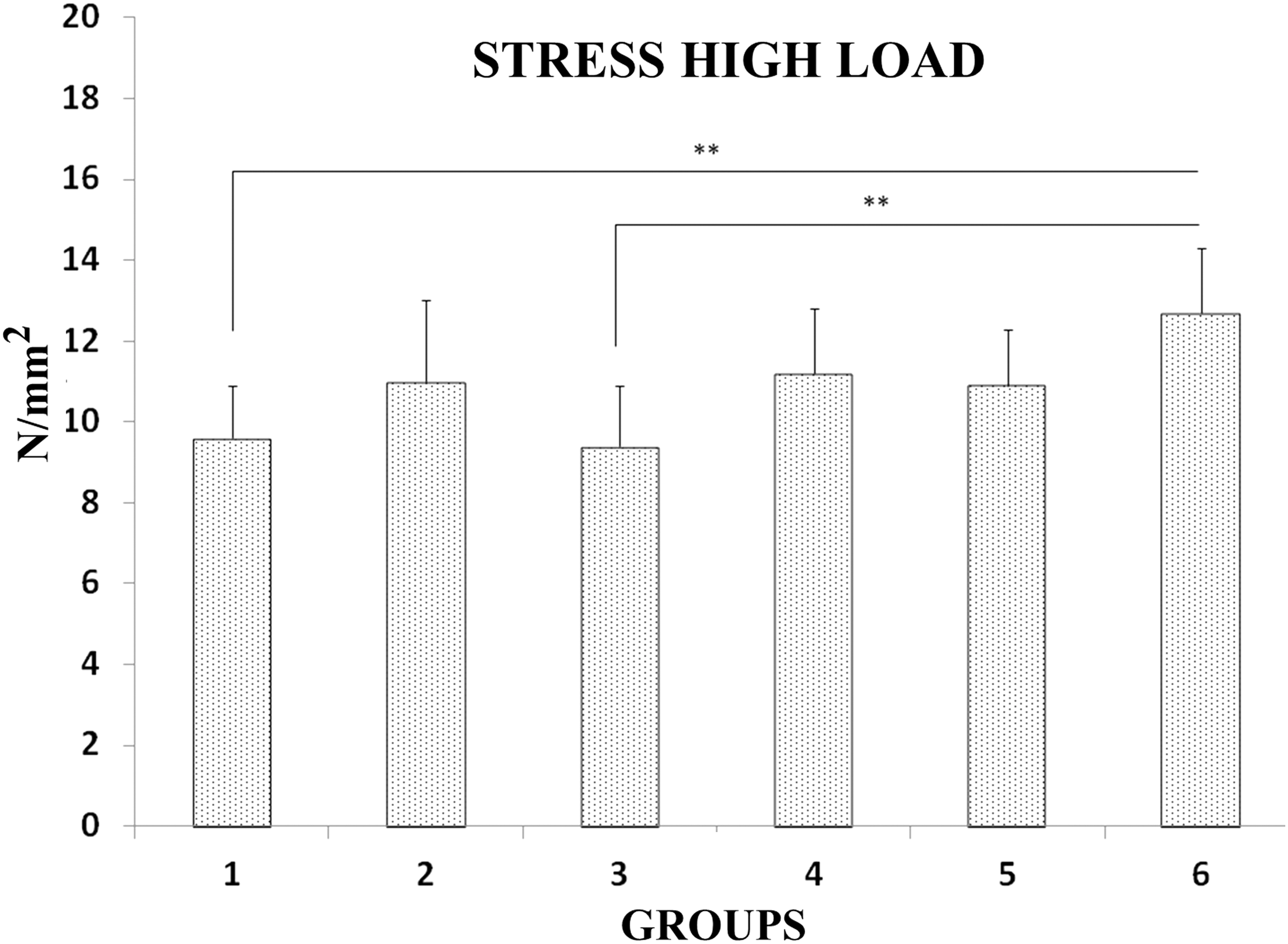
Mean ± SD of high stress load in the groups compared by the LSD test. **p < 0.01. LSD, least significant test.
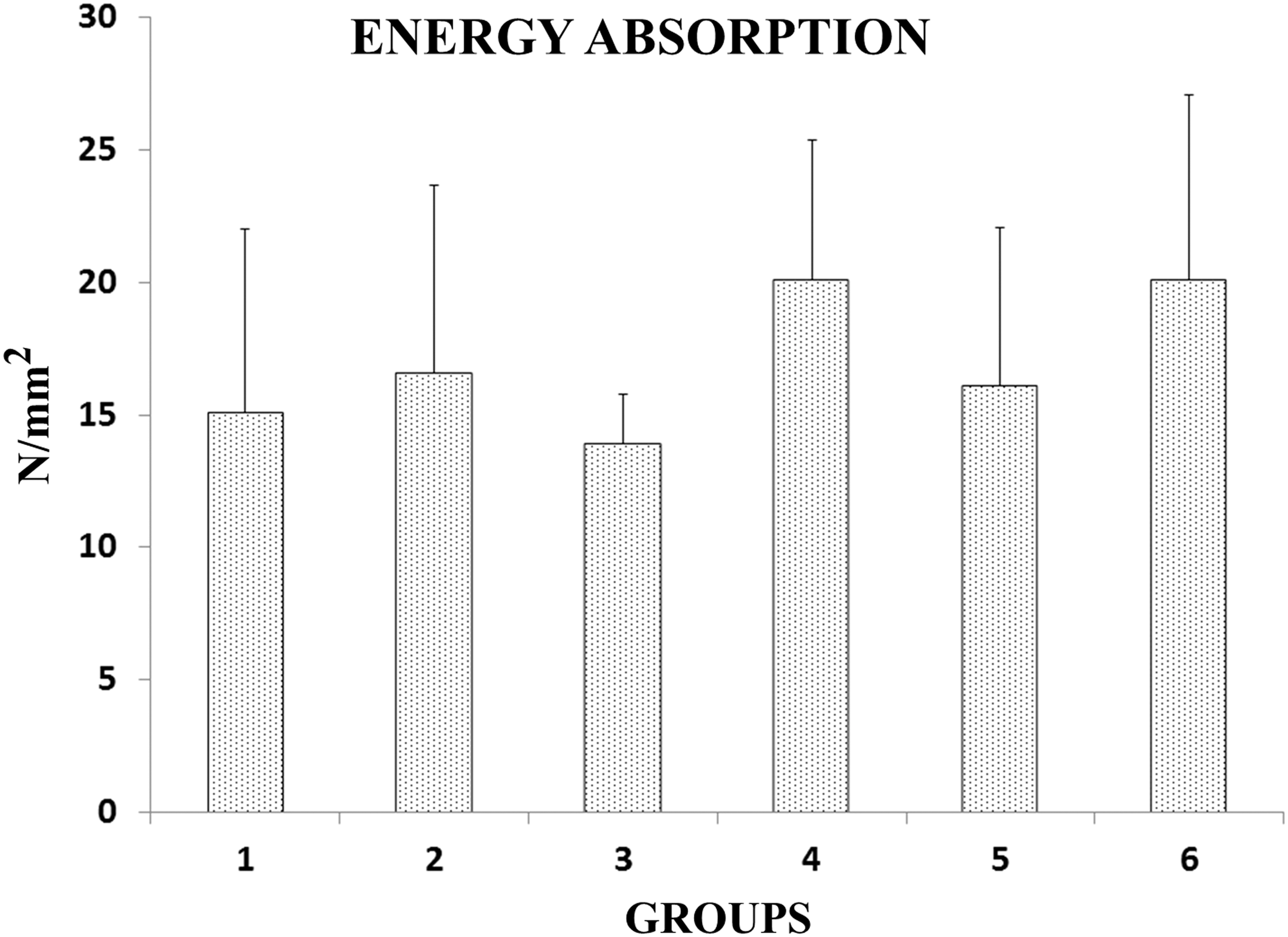
Mean ± SD of energy absorption in the groups compared by ANOVA.
Bending stiffness (N/mm)
The ANOVA for bending stiffness showed no significant differences among the studied groups (Fig. 7).
Maximum force (N)
The ANOVA for the maximum force variable produced p = 0.016. We observed a significant increase in maximum force in group 5 (PW laser + alendronate) compared with the healthy control group (p = 0.002, LSD test) and the diabetic control group (p = 0.003, LSD test; Fig. 8).
Stress high load (N/mm2)
ANOVA for the high stress load variable produced p = 0.035. We observed a significant increase in the high stress load in group 5 (PW laser + alendronate) compared with the healthy control group (p = 0.005) and the diabetic control group (p = 0.003, LSD test; Fig. 9).
Energy absorption (N/mm)
The ANOVA for energy absorption showed no significant differences among the studied groups (Fig. 10).
Discussion
When a long sample of bone is incrementally loaded, its load—deformation curve initially exhibits a linear relationship between the load and the deformation (the elastic region). However, at a particular stress (yield point) the further increase in load leads to a nonlinear deformation response, where small additional loads produce a large strain increase as a result of accumulation of damage (micro-cracks) in the material and a resultant decrease in stiffness (Fig. 2B). Bone is said to start to deform “plastically” at that point. An additional increase in load will eventually result in breakage of the sample; the stress, at which this happens, is named the stress high load (ultimate stress), which represents the strength of the bone.
Bending tests are not only the most common methods used to test whole bones but also are used particularly to define the mechanical behavior of bones from small rodents such as mice and rats that belong to different strains or treated by various drugs, which may affect the skeleton. 25 Whole-bone bending tests are mostly three- or four-point bending experiments. In the three-point bending test, the long bone (two extremities) is placed onto two supports (Fig. 2). A single-pronged loading device is applied at a point precisely in the middle between the two supports (Fig. 2A). In this manner, maximal force occurs at the point of the load application and the bone will eventually fracture at this location. 26
In the current study, we measured bone density in terms of HU. The HU of the bone defects in group 6 (OVX + TIDM + PW laser + alendronate) were significantly higher than the healthy control and diabetic control groups. At the same time, HU of the bone defect in laser-treated OVX rats showed a significant increase compared with control diabetic rats. Rats have been utilized as a standard rodent model in biomechanical skeletal studies. 27 We used the three-point biomechanical bending test to measure bone strength. The results showed significantly higher stress high load for group 6 compared with the healthy and diabetic control groups.
Bone strength could be indirectly estimated by imaging techniques such as bone mineral density (BMD) using Dual-Energy X-ray absorptiometry and CT scanning. Studies have shown that these techniques account for 60–70% of the variation in bone strength; however, these techniques do not capture many imperative factors. 28,29 Thus, an assessment of the intrinsic mechanical quality of bone tissue should provide a better understanding from the aspect of tissue quality in determining bone strength. 30 –34 The ultimate reason for bone fracture following minimal trauma is a reduction in mechanical strength. 32 Although bone densitometry is frequently used to assess bone fragility, direct biomechanical testing of the bone undoubtedly provides more information about mechanical integrity. 33 In the current study, we have measured the biomechanical properties of bone defects.
Growing evidence corroborates the fact that DM influences skeletal metabolism. Decreased BMD and increased fracture risk have consistently been observed in patients with TIDM. 34 Therefore, it is important to investigate treatments that have osteogenic potential, the capability to stimulate bone formation, and prevent bone loss. 35 The osteogenic effects of PW laser on osteoblastic cell proliferation in vitro and in vivo and osteochondral defect and bone repair in healthy and TIDM animals have been reported. 11 –16 Similarly, the positive effects of a continuous wave (CW) laser (Ga–Al–As, 808 nm, 100 mW, 33 sec, 120 J/cm2, 3.3 J per point) on histological parameters, biomechanical properties, and BMD of intact long bones (instead of the partial bone defect in the current study) in an STZ animal model of TIDM have been reported. Patrocinio-Silva et al. 36 initiated CW laser 15 days after the induction of TIDM instead of 30 days in the current study. They performed CW laser for 18 sessions over a period of 42 days compared with 30 days in the current work. They suggested that additional experimental and clinical studies should be developed in an attempt to provide more information about the mechanisms of action of lasers in diabetic bones. 36 In the current study, the PW laser with an 890-nm wavelength, 80 Hz pulse frequency, 1300 sec duration, and 1.5 J/cm2 energy density failed to cause any beneficial effects in the biomechanical 21 properties to repair the partial osteotomy in STZ+OVX rats. The findings of this study supported other studies that evaluated the effects of lasers on experimental osteoporotic animals. 21,35,37
Fridoni et al. used the three-point bending test to evaluate the effects of PW laser on tibial shaft bone strength in two experimental OP rat models. 21 The researchers conducted laser (890 nm, 80 Hz, 0.972 J/cm2) irradiation of the entire tibia three times per week for 8 weeks. Both groups of rats received alendronate. Laser irradiation at those parameters failed to cause remarkable biomechanical effects in the osteoporotic cortical bones. Laser combined with alendronate induced a greater effect on bone strength in the OVX-induced OP rat model. 21 Muniz Renno et al. 35 investigated the effects of infrared laser on exercised osteoporotic rats. The exercise program and CW laser (GaAlAs laser, 830 nm, 120 J/cm2) were performed every 48 h during an 8-week period. Exercised rats had higher bone toughness and physical property parameters compared with the other groups. However, laser treatment did not reinforce the positive effects from exercise on the osteoporotic femurs. 35 The impact of CW laser (GaAlAs, 830 nm, CW, 30 mW/cm2, 250 J/cm2) and electrical stimulation (SCE, 1.5 MHz, 1:4 duty cycles, 30 mW, 20 min) on bone loss in spinal cord-injured rats was studied by Medalha et al. 37 Electrotherapy had significantly higher values for the inner diameter, as well as the external and internal areas of tibia diaphysis compared with the spinal cord-injured rats. Laser treatment showed a trend toward the same result compared with normal rats. They observed no increase in mechanical or densitometry parameters. 37
Despite tremendous progress in the OP field, therapeutic outcomes and management of fractures in osteoporotic bone remain clinically challenging as reported in a review by Torstrick and Guldberg. Skeletal fragility cannot only be attributed to failure to create a skeleton of optimal mass and strength during growth and excessive bone resorption, which lead to decreased bone mass and microarchitectural deterioration of the skeleton. Instead, it can be the result of an inadequate formation response to increased resorption during bone remodeling. 38 Decreased bone density and a delayed healing process can lead to fracture nonunion. 9 Torstrick and Guldberg suggest local treatment strategies such as external mechanical stimulation via low intensity pulsed ultrasound (LIPUS) to provide for the local treatment of osteoporotic fracture, either alone or combined with other therapies. However, the effect of LIPUS on intact osteoporotic bone is inconclusive. 9
The biostimulatory effects by laser insufficiently decreased the negative effects from the experimental OP. 21,35,37 The combined effects of alendronate and laser in STZ + OVX rats preserved ontogenesis. PW laser + alendronate significantly increased the stress high load of the partial osteotomy that was repaired in STZ + OVX rats compared with the control groups. The results of this study confirmed data from a previous study. 37 Diniz et al. reported a positive effect by CW laser (Ga Al As laser, 830 nm, and 4 J/cm2) combined with bisphosphonate on osteoporotic trabecular bone structure. They suggested that CW laser combined with bisphosphonate administration was the best method to reverse OVX-induced OP in the vertebral column. 39 The cumulative effects of alendronate and LIPUS on metaphysical bone repair after osteotomy in the proximal tibia of aged rats were investigated by Aonuma et al. 40 They concluded that alendronate + LIPUS caused an extra increase in BMD at the affected metaphysis. 40 Hypotheses that attempt to explain the lack of biostimulatory effect of photobiomodulation on osteoporotic rats have been suggested. First, this could be attributed to the profound, systemic effects of TIDM, and OP on bones. The STZ + OVX models used in the current study were so strong that the osteoporotic bone tissue could not respond properly to biostimulation by laser or alendronate alone. Second, the photobiomodulation parameter energy density was chosen based on a work that reported that the 890 nm laser at 1.5 J/cm2 increased bone strength in healthy rats. 23 Third, this could be attributed to the fact that the laser relies to a large extent on the local effects of lights on the tissues, 41 whereas TIDM and OP are systemic diseases. The fourth reason has been supported by other studies that reported that laser associated with bone scaffold improved biomechanical properties of tibial bone callus in osteoporotic rats. 42,43
In the current study, the STZ + OVX animal model had a negative effect on repair of the partial tibial osteotomy. The combined treatment of laser and alendronate significantly enhanced partial osteotomy bone repair compared with the control groups. Since the laser has estrogenic effects, different parameters should be investigated to verify if an appropriate photobiomodulation protocol alone or in combination with a proper antiosteoporotic agent and/or bone scaffold would be able to reverse the detrimental effects of OVX-induced OP in diabetic rats.
Footnotes
Acknowledgments
We extend our sincere thanks to the late Mrs. Jamileh Rezaei. This article is financially supported by the Research Department of Shahid Beheshti University of Medical Sciences, Tehran, Iran (Grant No. 1393-1-91-13237).
Author Disclosure Statement
No competing financial interests exist.