
Abstract
Introduction
O
TMD is frequent; however, its symptoms are complex and pain is the main sign, 2 –4 usually on the pre-auricular region, which may spread to the temporal, frontal, and occipital regions. 1,5
Older patients rarely report sounds in the temporomandibular joint; 6 on the other hand, young patients report pain mainly on palpation of the masticatory muscles; women are more affected by TMD in a ratio of two to one. 7 –11
Emotional stress is important in the early stages of TMD development, involving the masticatory muscles and their fascias, the psychophysiological TMD development theory. 12
In 80% of patients, the main cause of the painful symptoms of TMD are spasms of the masticatory muscles, which can be caused by distension, contraction, or fatigue of those muscles, mainly caused by parafunctional habits and affected by emotional stress. 13
TMD is progressive, creating a cycle where the muscle spasm leads to a functional limitation that leads to pain, and this, in turn, produces more spasm and more pain, the so called “pain-spasm-pain syndrome.” 14
There are several treatments for pain associated with TMD like drugs [physiotherapeutic and drug protocol (PDP)], heat, cryotherapy, local anesthesia, occlusal appliances, physiotherapy, transcutaneous electrical neural stimulation, and low-level laser (LLL), which can reduce inflammation, relax masticatory muscles, and reduce pain. 15
Red and infrared LLL wavelengths have been clinically used to reduce different kinds of pain, including pain associated with TMD.
The protocol suggested in this clinical trial has been used at Cruzeiro do Sul University and at Caruaru Federal University with good results.
Objective
The objective of this study was evaluating the effectiveness of Gallium-Aluminum Arsenide (GaAlAs) laser diode, 780 nm, (LLL), in the treatment of pain associated with TMD, compared to PDP and placebo.
Materials and Methods
The clinical trial was initiated after approval of the Research Ethics Committee in Human Beings, EC protocol number/UCS-167/2011, held in the Stomatology department of Center for Dental Specialties (CEO), at Caruaru Federal University (ASCES), and conducted by Professor Uoston Holder Silva.
Diagnosis was made using the method of muscle tenderness palpation 16 and the questionnaire of Fonseca, 17 which ranks (0–15) no TMD, (20–40) mild TMD, (45–65) moderate TMD, and (70–100) severe DCM.
LLL therapy
LLL device—Twin Flex Evolution, MM optics®, São Carlos, Brazil, sent to be calibrated by the manufacturer before use.
LLL description—780 nm GaAlAs infrared laser diode, power 70 mW, irradiance 1.75 W/cm2, and laser spot 0.04 cm2
LLL application protocol—35 J/cm2 was applied in contact with each of the five following points: (intraoral) pterygoid medial, (extraoral) intra-headset, pre-headset, gonion, and anterior superior insertion of masseter (Fig. 1), for 20 sec every other day, except weekends, for four weeks, total dose applied to each point 420 J/cm2, patient cumulative dose 2100 J/cm2, total energy delivered per patient during treatment 84 J (Table 1).

LLL application points to reduce pain associated to TMD,
Dose energy density or fluence (J/cm2), time exposure (seconds), energy (J), gallium-aluminum arsenide (GaAlAs) infrared wavelength 780 nm, irradiance or power density 1.75 W/cm2.
PDP therapy
Hot packs, thrice a day (morning, afternoon, and evening) for 15 min each, at intervals of 5 min; mouth exercise of opening and closing twice a day, associated to MIOFLEX-A (myorelaxing drug) thrice a day; and MOVATEC 7.5 mg (anti-inflammatory drug) once a day.
Placebo therapy
Application of 480 nm halogen light of the Optilight® curing device at the same points and with the same frequency of the LLL application, simulating LLL irradiation.
Exclusion criteria and ethical considerations were excluded from this study, all patients diagnosed as mild TMD, whose TMD was associated with systemic diseases, arthrogenic TMD, traumas, disc displacements, and cancer.
Sample—60 females, 20–50 years old, with moderate and severe TMD, controlled in relation to the triggering agents (stress, parafunctional habits) (Table 2) were randomly divided into three groups: group 1—LLL, group 2—PDP, and group 3—placebo.
All patients were females, from class C and D, nonsmoking, ages varying between 20 and 50 years, presented severe and moderate TMD, and had parafunctional habits removed before treatment started.
TMD, temporomandibular disorders.
Statistical analysis
The statistical program used to analyze the results was the Statistical Package for Social Sciences, SPSS 17.
Data were analyzed using the chi-square test and Fisher's exact test (p < 0.05).
Results
Evaluation results of pain before treatment, the majority in each group had moderate pain, with percentages ranging from 70% (PDP group) to 85% (LLL group), and the rest of the patients in each group had severe pain, without statistical differences (p > 0.05) (Fig. 2).
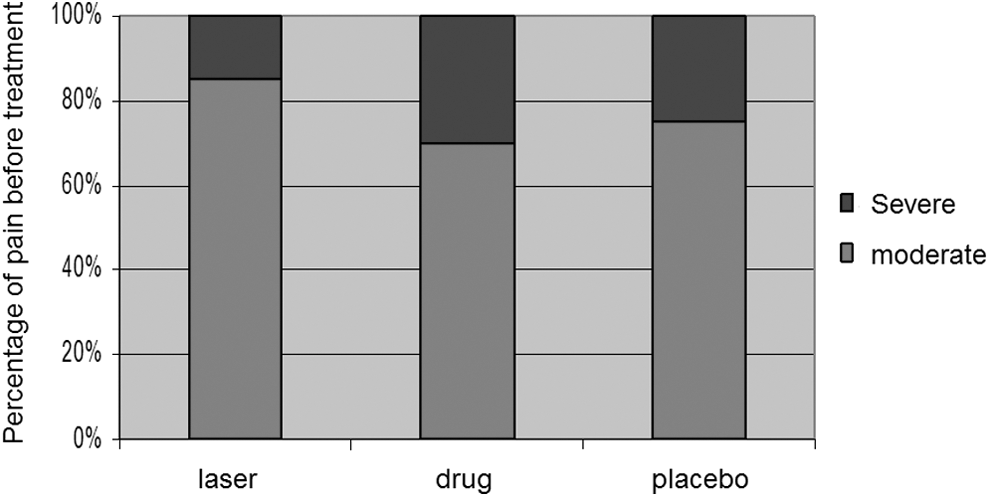
Evaluation of pain before treatment; the majority in each group had moderate pain, with percentages ranging from 70% (PDP group) to 85% (LLL group) and the rest of the patients in each group had severe pain. PDP, physiotherapeutic and drug protocol.
Data of LLL and placebo groups were collected and analyzed on Mondays, Wednesdays, and Fridays, but for the PDP group, data were collected and analyzed just on Fridays.
First week: On Monday, all patients from each of the LLL and placebo groups had pain.
On Wednesday, 85% of the samples of LLL and placebo had pain. On Friday, 60% of LLL, 70% of placebo, and all PDP patients related pain (Fig. 3).
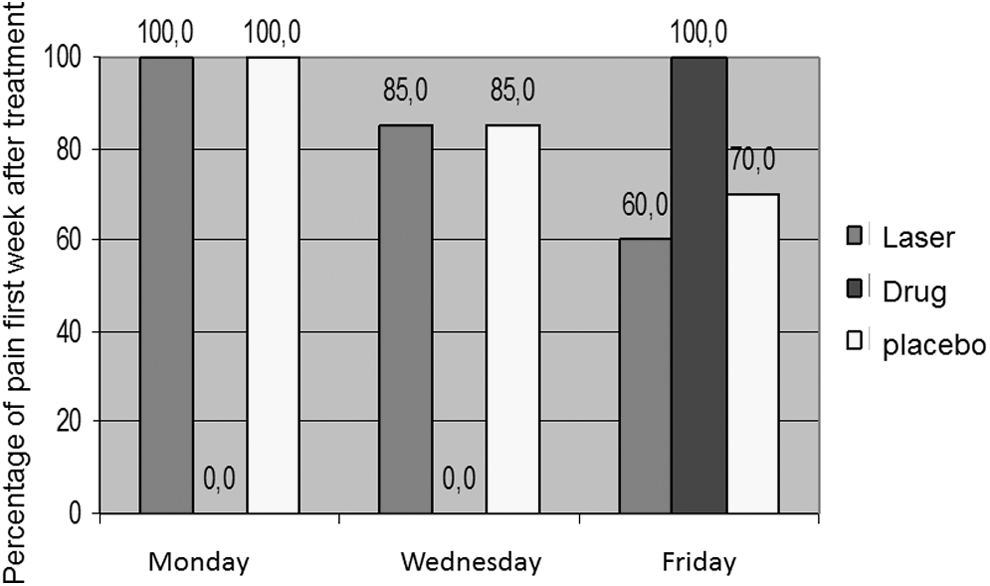
Evaluation of pain first week after treatment initiation, 60% of LLL, 70% of placebo, and all PDP patients related pain.
Second week: On Monday, the percentage of patients with pain was much higher in the placebo group than in the LLL group, 75% placebo and 40% LLL; on Wednesday, 65% of placebo and 20% of LLL related pain; and on Friday, 100% of placebo, 55% of LLL, and 15% of PDP had pain (Fig. 4).
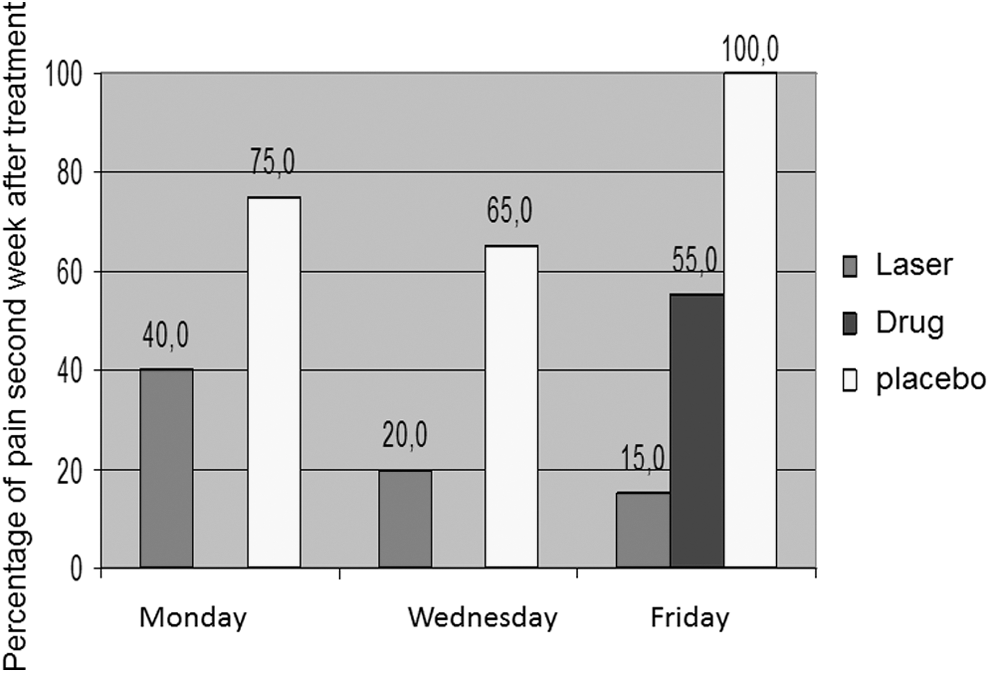
Evaluation of pain second week after treatment initiation, 100% of placebo, 55% of LLL, and 15% of PDP had pain.
Third week: On Monday, the placebo group reported more pain than the LLL group, 75% placebo and 15% LLL; on Wednesday, 50% of placebo and 15% of LLL had pain; and on Friday, the placebo group reported 85% of pain, the PDP group 15%, and the LLL group 10% (Fig. 5).
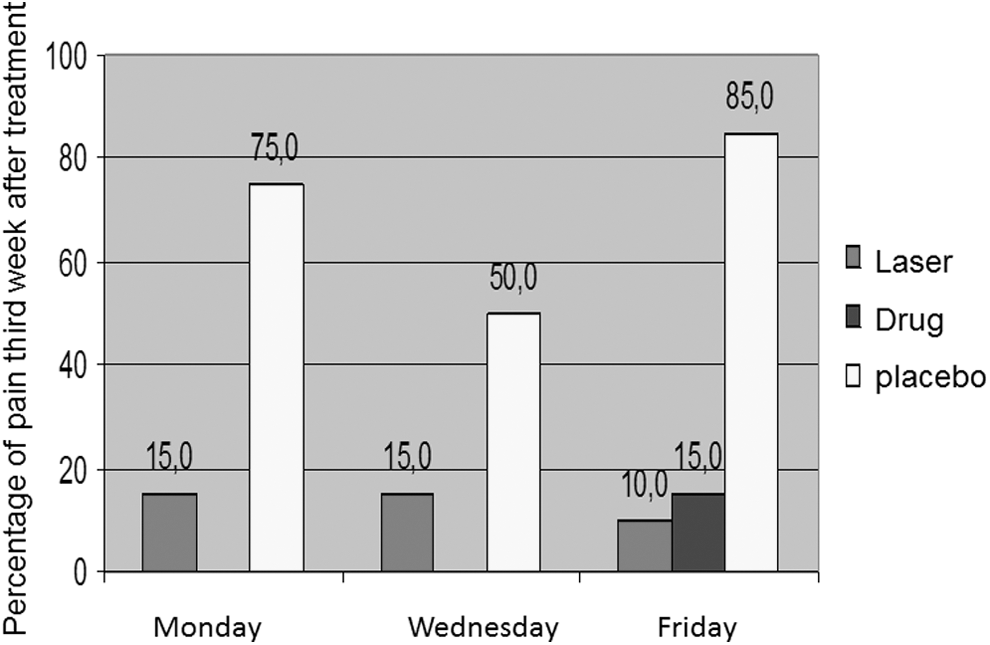
Evaluation of pain third week after treatment initiation, placebo group reported 85% of pain, the PDP group 15%, and the LLL group 10%.
Fourth week: On Monday, the percentage of pain was much higher in the placebo group (70%) than in the LLL group (5.0%); on Wednesday, all patients in the placebo group had pain, while the LLL group had no pain. On Friday, while all patients in the placebo group had pain, no patient of LLL and PDP presented pain.
No patients in the actual study reported any side effects.
The results were statistically significant (p < 0.05%). After the fourth week, all patients in the placebo group received conventional therapy to control pain. All patients were seen for 60 days and showed no recurrence during this period (Fig. 6).
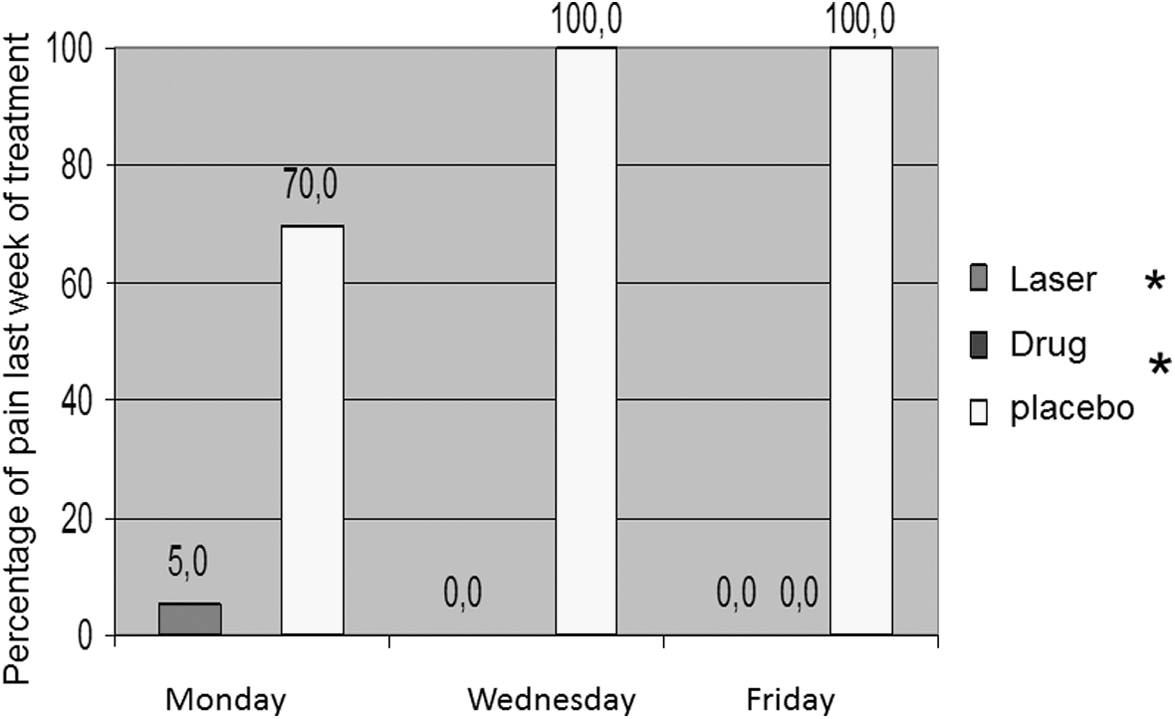
Evaluation of pain fourth week after treatment initiation, all patients in the placebo group had pain, no patient of LLL and PDP presented pain (*statistically significant, p < 0.05).
Discussion
Our results state that LLL can control pain associated with TMD.
Comparing LLL and PDP treatments is important because, despite the fact that there are other treatment options, 18 –21 PDP is widely used to control this kind of pain.
LLL has been used to control acute and chronic pain associated or not with drugs; it promotes analgesia, 22 but the analgesic power of opioids or mimetic opioids is higher than that produced by LLL, its biological principle is related to lessen the releasing of algogenic factors (serotonin and bradykinin) at tissue injury sites. 23
Chow et al., 24 states that the specific inhibition of nerve fibers Aδ and C by LLL is of particular relevance to the explanation of the analgesic effects; experiments also point to a reduction in the responses of the nociceptors stimulated by a wide variety of noxious stimuli, including pro-inflammatory.
Pain reduction mechanism of LLL reduces inflammation 25 and also promotes muscle relaxation, 26 like PDP that uses anti-inflammatories associated with muscle-relaxing drugs and physiotherapy to control pain.
In our experiment, patients evaluated before treatment-related severe and moderate pain.
Analyzing our results, pain began to decrease at the end of the first week for patients who received LLL and more gradually at the end of the second week in the PDP group.
During treatment, the placebo group-related pain variation, which can be attributed to anxiety and depression control, 27 –30 but at the end of the treatment, the placebo group had pain in 100% of cases and LLL and PDP groups presented no pain.
In the economic point of view, the laser patients had to visit the clinic (3 × 4) = 12 times, while the PDP patients only had to come 4 times. This reveals a weakness in the LLL treatment compared to PDP, which was more convenient and cost effective, when chair time, travel, and staff expenses are included. Using a home care laser device could even these differences in cost-effectiveness.
In our opinion, just like Bjordal et al., 31 the use of LLL fulfills therapeutic requirements.
Conclusions
Based on obtained data, we concluded that, compared to PDP, LLL treatment is effective to control pain associated with TMD.
Footnotes
Acknowledgments
We would like to thank our friend Professor Uoston Holder Silva, from Federal University of Rio Grande do Norte (UFRN), who died last November, for conducting this clinical trial.
Author Disclosure Statement
No competing financial interests were reported.