
Abstract
Introduction
P
Peripheral facial palsy may be caused by trauma, accidental injuries, viral infections, inflammations, metabolic diseases, and tumors. The incidence of this condition is 20–30 cases in 100,000 individuals. It may lead to complications in verbal communication through facial expressions, which are very important in social relationships. 4 –9
Injuries involving peripheral nerves are classified, according to Seddon (1943), functionally and anatomically into neuropraxia, axonotmesis, and neurotmesis. 10 In 1951, Sunderland described five types of nerve lesions: the first type corresponds to neurapraxia and the second to axonotmesis. The third, fourth, and fifth types involve injury, respectively, to endoneurial tubes, perineurium, and epineurium. 11
Depending on the type of injury, the peripheral nerves may present regenerative capacity by themselves or through the use of surgical techniques, such as in the case of neurotic injuries, in which the nerve suffers total sectioning of the axon and its surroundings. 12,13 For neurotimic and small extension injuries, end-to-end epineural neurorrhaphy, where the stumps may be approximated and sutured without exaggerated tension, is considered the gold standard. 14,15
However, neurorrhaphy techniques that use sutures require knowledge of microsurgical techniques and the functional damage that can result from excessive manipulation of tissues. 16,17 Fibrin sealant is currently used in the recovery of peripheral nerves with the aim of minimizing the disadvantages of epineural suture techniques. 18
The new heterologous fibrin sealant derived from snake venom is a biological and biodegradable product containing no human blood, preventing the spread of infectious diseases. It also has good adhesive capacity and is used as an adjunct to conventional suture procedures. 19 The clot formed by the fibrin sealant is a physiological component found in the repair of tissues, differing from that of other types of sealants that present high fibrin formation and toxicity. The fibrin sealant can be a useful tool in the clinical environment as it presents high versatility and reduced cost in comparison with commercial adhesives. 20
Low-level laser therapy (LLLT) is another modality used in the process of regeneration and functional recovery of peripheral nerves. It was first used in the 1980s and has been the subject of numerous recent studies because it demonstrates an immediate protective effect, reducing the formation of edema and scar tissue in the region of the injury and increasing axonal metabolism. 21,22 In addition, it has analgesic and anti-inflammatory properties and increases mitotic activity, leading to a faster nerve regeneration process. 23,24
The photobiostimulatory effect of LLLT refers to a tissue uptake by photoreceptors, thus facilitating mitochondrial respiration, adenosine triphosphate production, additional calcium transport in the cytoplasm, and initiation of signaling pathways mediated by reactive oxygen species, the cyclic adenosine monophosphate and nitric oxide. 25 These effects lead to activation of several transcription factors related to cell migration, proliferation, survival, tissue repair, and nerve regeneration. 26
Functional evaluation of the repair of nerve injuries usually complements morphological evaluations. In rats, one method is the evaluation of movements of the whiskers through its position and movement. The movement without tremors and the anterior positioning of the whiskers generally serve as reference for the analysis of postinjury recovery. 27,28
Because of the way in which it is currently produced, the new heterologous fibrin sealant has not been subjected to functional testing on facial nerve lesions. Taking into account the incidence of nerve injuries and their functional and social effects, the present study aimed to evaluate the efficacy of LLLT on qualitative, quantitative, and functional aspects of the facial nerve regeneration process.
Materials and Methods
Experimental design
The experimental procedures were approved by the Animal Ethics Committee of the School of Dentistry of Bauru of the University of São Paulo (São Paulo, Brazil).
Forty-two 60-day-old male Wistar rats (Rattus norvegicus) with an average weight of 250 grams were used. All animals were kept in appropriate boxes and received water and food ad libitum with no movement restrictions, maintaining a 12-h light–12-h dark regime (temperature of ∼22°C).
The animals were randomly divided into a control group (CG) and four experimental groups: 1. CG consisted of 10 animals in which the buccal branch of the facial nerve was collected at 95 and 130 days, the euthanasia times of the experimental groups. 2. Suture experimental group (SEG) and fibrin experimental group (FEG) consisted of 16 animals in which the buccal branch of the facial nerve was sectioned on both sides of the face; end-to-end epineural suture was performed on the right side, and fibrin sealant was used on the left side for coaptation of the stumps. The animals were euthanized 5 weeks (95 days old) and 10 weeks after the surgery (130 days old). 3. Laser suture experimental group (LSEG) and laser fibrin experimental group (LFEG) consisted of 16 animals that underwent the same surgical procedures as SEG and FEG in combination with the application of LLLT. The animals were euthanized 5 weeks (95 days old) and 10 weeks after the surgery (130 days old).
Experimental surgery
For the surgical procedure, at the of age of 60 days, all of the animals in the experimental groups (SEG, FEG, LSEG, and LFEG) were weighed and submitted to general anesthesia by intramuscular injection of the anesthetic agent Zoletil 50 (Virbac, Brazil) in the following proportion: 1:1 (125:125 mg) tiletamine hydrochloride and zolazepam hydrochloride (0.15 mL/kg/IM). After adoption of antisepsis techniques for the procedure, trichotomy was performed on all of the animals and they were placed in the lateral decubitus position.
A facial incision was performed with a No. 15 scalpel blade (approximately from the tragus of the ear to the corner of the mouth) with subsequent dissection by layers up to the exposure of the buccal branch of the facial nerve (Fig. 1A). The nerve was sectioned with fine straight tip Íris surgical scissors (Quinelato; Rio Claro, Brazil) without removal of fragments (Fig. 1B).
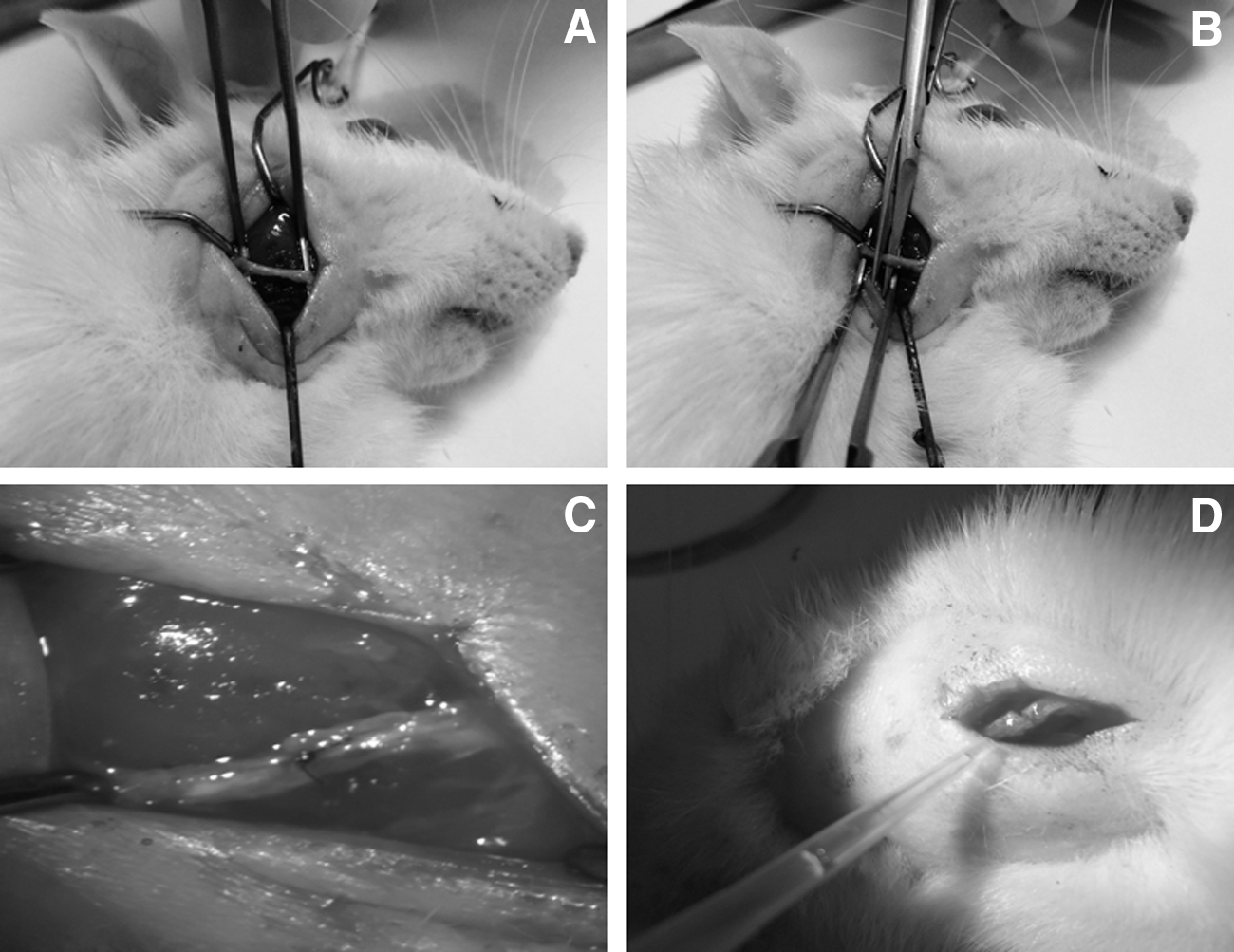
Experimental surgery:
In the SEG group, an end-to-end epineural suture was performed on the right side of the face with 10/0 monofilament nylon sutures (Ethicon; Johnson & Johnson, Brazil; Fig. 1C). In the FEG group, following the same procedure, the stumps were approximated and coaptated with the fibrin sealant (Fig. 1D). Completing the surgical procedure, the skin was sutured with 4-0 silk thread (Ethicon; Johnson & Johnson).
Fibrin sealant
A new heterologous fibrin sealant derived from snake venom was kindly supplied by the Center for the Study of Venoms and Venomous Animals of São Paulo State University; its constituents and instructions for use are stated in its patents (registration numbers BR1020140114327 and BR1020140114360) and it was prepared as suggested by Barros et al. 19 The components of the sealant were stored in three Eppendorf tubes and kept at −80°C. At the time of use, the components were thawed, then reconstituted, mixed, and applied according to the following protocol: the first bottle contained fibrinogen obtained from buffalo blood (5 μL), the second contained calcium chloride (2 μL), and the third contained a thrombin-like fraction (1 μL), totaling 8 μL. 19,20,29 –31
Photobiomodulation therapy
In the LSEG and LFEG groups, the animals were subjected to photobiomodulation (PBM) therapy with a continuous pulse from a gallium–aluminum–arsenide laser (GaAlAs; Laserpulse IBRAMED, São Paulo, Brazil). The protocol was applied using a laser pen on the skin surface, with the following parameters
32,33
: • Wavelength: 830 nm • Optical output power: 30 mW • Power density: 0.2586 W/cm2
• Energy density: 6.2 J/cm2
• Beam area: 0.116 cm2
• Exposure time: 24 sec per point • Three different points along the surgical site • Total energy per point: 0.72 J • Total energy per session: 2.16 J • Cumulative dose: 34.56 J
The laser source had previously been tested to verify the dose. The laser therapy applications were performed 1 day after surgery and three times a week in the postoperative period for a total of 5 weeks. 34 –38 For the application, the animals were carefully restrained by placing the operator's hand firmly over the back and rib cage. The laser pen was placed over the incision area, in three points: cranial, middle, and caudal, in relation to the cranial delimitation plane (Fig. 2).

Positioning of the laser pen over the surgical area. Application at the caudal point of the incision, with cranial and midpoint markings (black circle).
Functional analysis
During the postsurgical period, the animals were submitted to observation of facial movement, spontaneously and under stimulation. Each rat was individually assessed twice, at the 5th and 10th weeks, in a cardboard box with a black inner surface to provide more clarity in the observation of whisker movement. The observer clapped his palms together three or four times to generate better whisker movement. This observation was made by the same examiner and all of the animals were photographed and filmed for more efficient data collection. The observer classified the whisker movement according to the scale below, as described by Faria et al. 27 (Table 1).
Euthanasia and histological processing
At 5 and 10 weeks after the surgical procedure, 5 animals from the CG and 16 animals from the experimental groups were euthanized by anesthetic overdose. The previously operated site was reopened to capture images of the nerve stumps using a digital microscope (Dino Lite Plus, Taiwan) and to collect the undamaged buccal branch of the facial nerve in the CG and the distal stump from the buccal branch of the facial nerve in animals from the experimental groups (SEG, FEG, LSEG, and LFEG).
The samples were fixed in Karnovsky's solution for 24 h and then immersed for 2 h in 1% osmium tetroxide (Sigma-Aldrich, USA). Then, the sections were subjected to routine procedures for inclusion in histological resin (Leica Historesin, Germany). After inclusion, ultrathin transverse sections (5 μm) of the fascicles were obtained and stained with 1% toluidine blue. The images were captured using an Olympus microscope (Japan) and photographs were taken with a coupled digital camera (Olympus DP 71, Japan).
Quantitative analysis of regenerated axons
Quantitative evaluation of regenerated axons in the distal stump of the buccal branch of the facial nerve was performed in the experimental groups with three images obtained with 400x magnification, involving analysis of the total number of myelinated axons in a 9000 μm2 nerve area and the partial density of myelinated axons [partial number of axons/partial area (9000 μm2)], according to Bento et al. 39
Statistical analysis
The data obtained from whisker movement were compared using Fisher's exact test. 28 Quantitative analysis was carried out using Image Pro-Plus 6.0 software (Media Cybernetics, Bethesda, MD). The total number and density of regenerated axons were analyzed using the unpaired t-test (significance level α < 0.05) once normality was demonstrated (Shapiro–Wilks test), and comparisons were between groups that had the same repair technique with or without LLLT (SEG × LSEG; FEG × LFEG) during the same period. The software program used for statistical analysis was GraphPad (La Jolla, CA).
Results
Functional analysis
The CG was used as a measure of normality in relation to the movement and position of the whiskers (score 5), according to the parameters established in Table 1 (Fig. 3A, B).
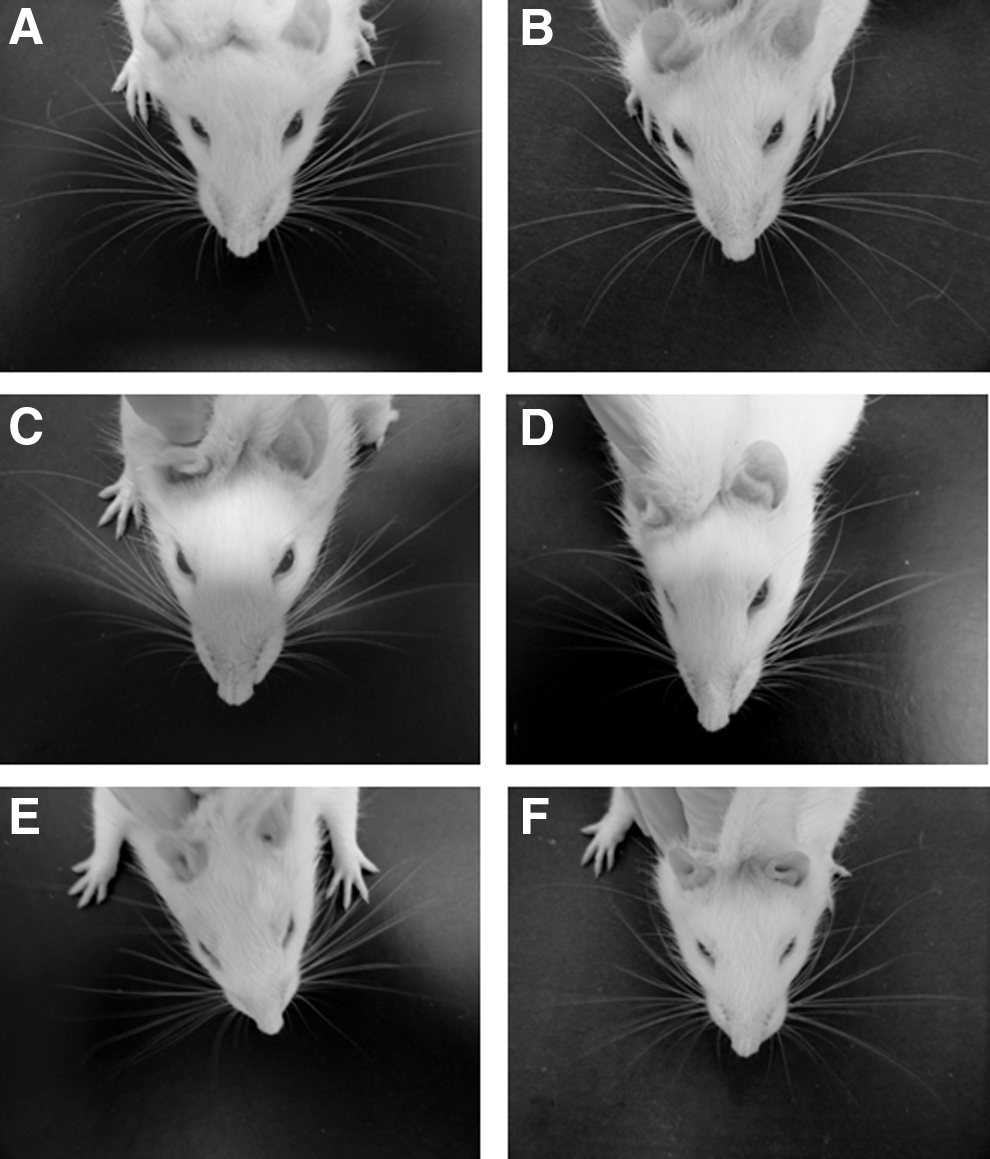
At 5 weeks, the SEG and FEG presented median scores of 3.1 and 3.3, respectively, representing movement with major tremor and posterior position (Fig. 3C). The LSEG and LFEG, which were submitted to LLLT, presented median scores of 4.0 and 4.2, respectively, corresponding to normal movement and posterior position (Fig. 3D).
At 10 weeks, the SEG and FEG presented median scores of 4.1 and 4.3, respectively, representing normal movement and posterior position (Fig. 3E). The LSEG and LFEG presented median scores of 4.8 and 4.9, respectively, with normal movement and anterior position, similar to the CG (Fig. 3F).
Figure 4 shows the scores for assessment of whisker movement and position in all animals of all groups in the assessed periods (mean and standard deviation).
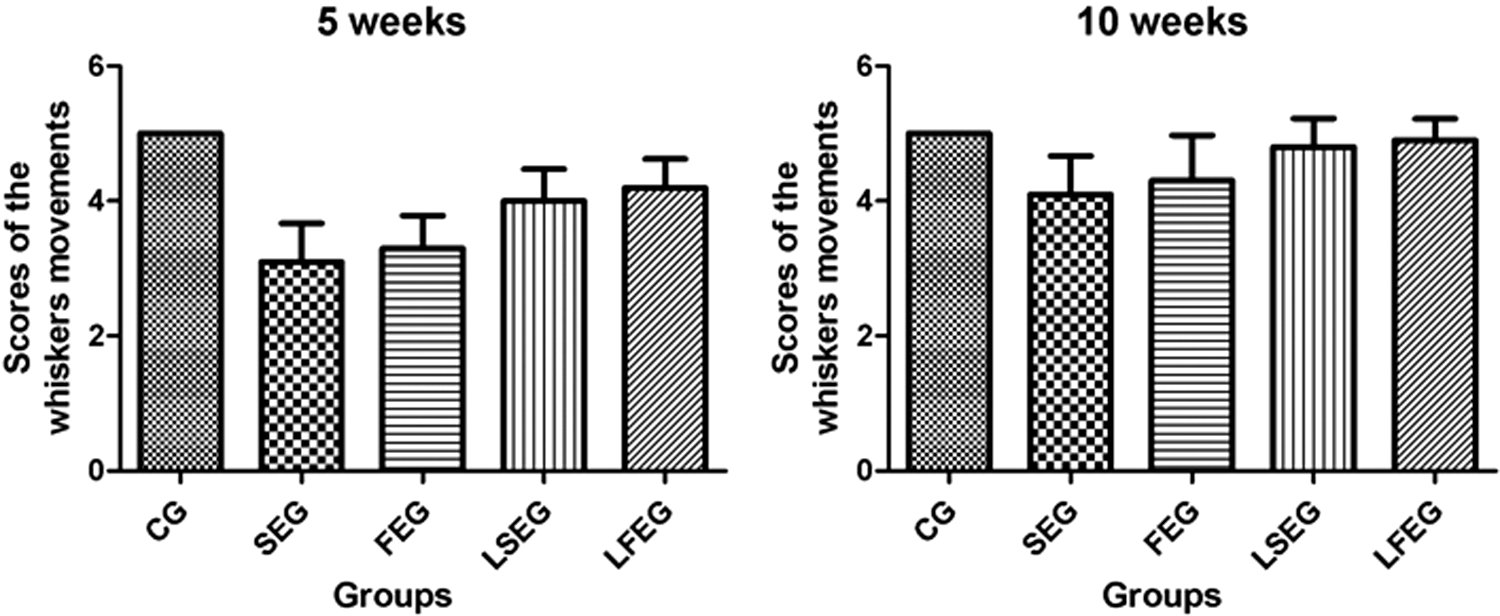
Results of the functional analysis (whisker movement and position).
Morphological assessment (digital microscopy)
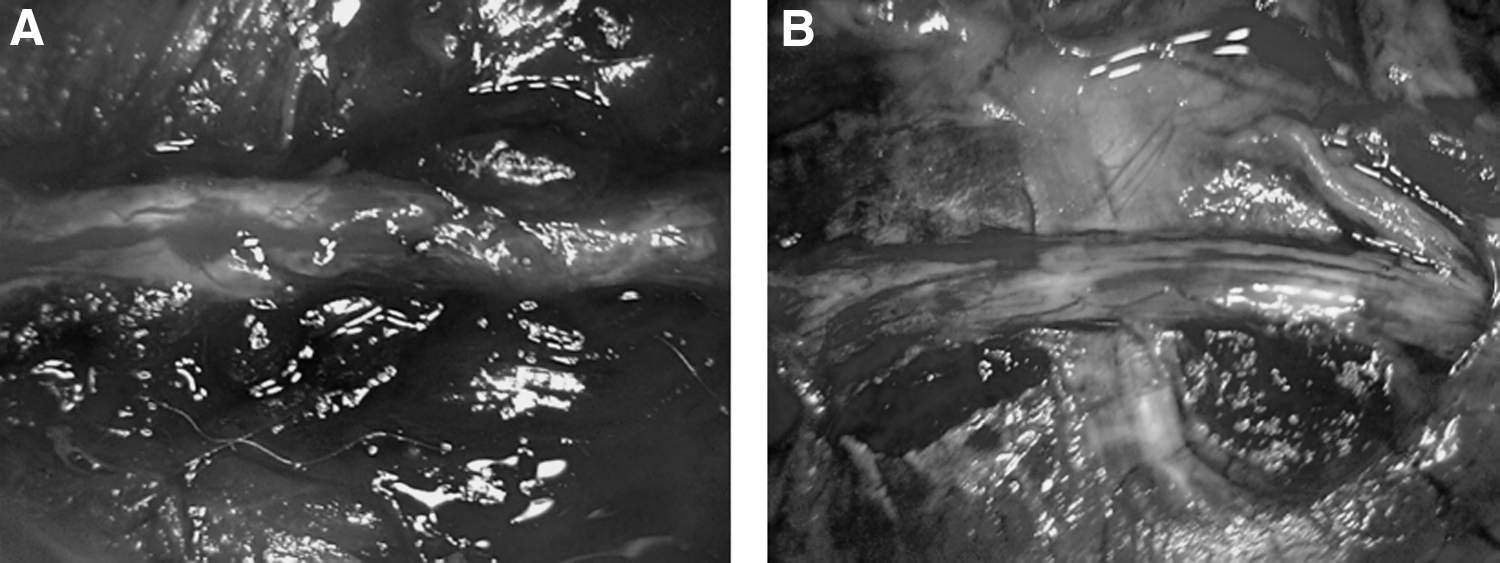
In both analyzed periods, all of the animals presented nerve stumps fixed by suture or fibrin sealant (Fig. 5).
Morphological assessment (optical microscopy)
Five weeks after surgery, all animals in the CG presented myelinated fibers regularly arranged inside the nerve with regular morphology. The experimental groups presented myelinated fibers irregularly arranged with heterogeneous diameters distributed inside the nerve, adjacent connective tissue, and the presence of new blood vessels (Fig. 6).
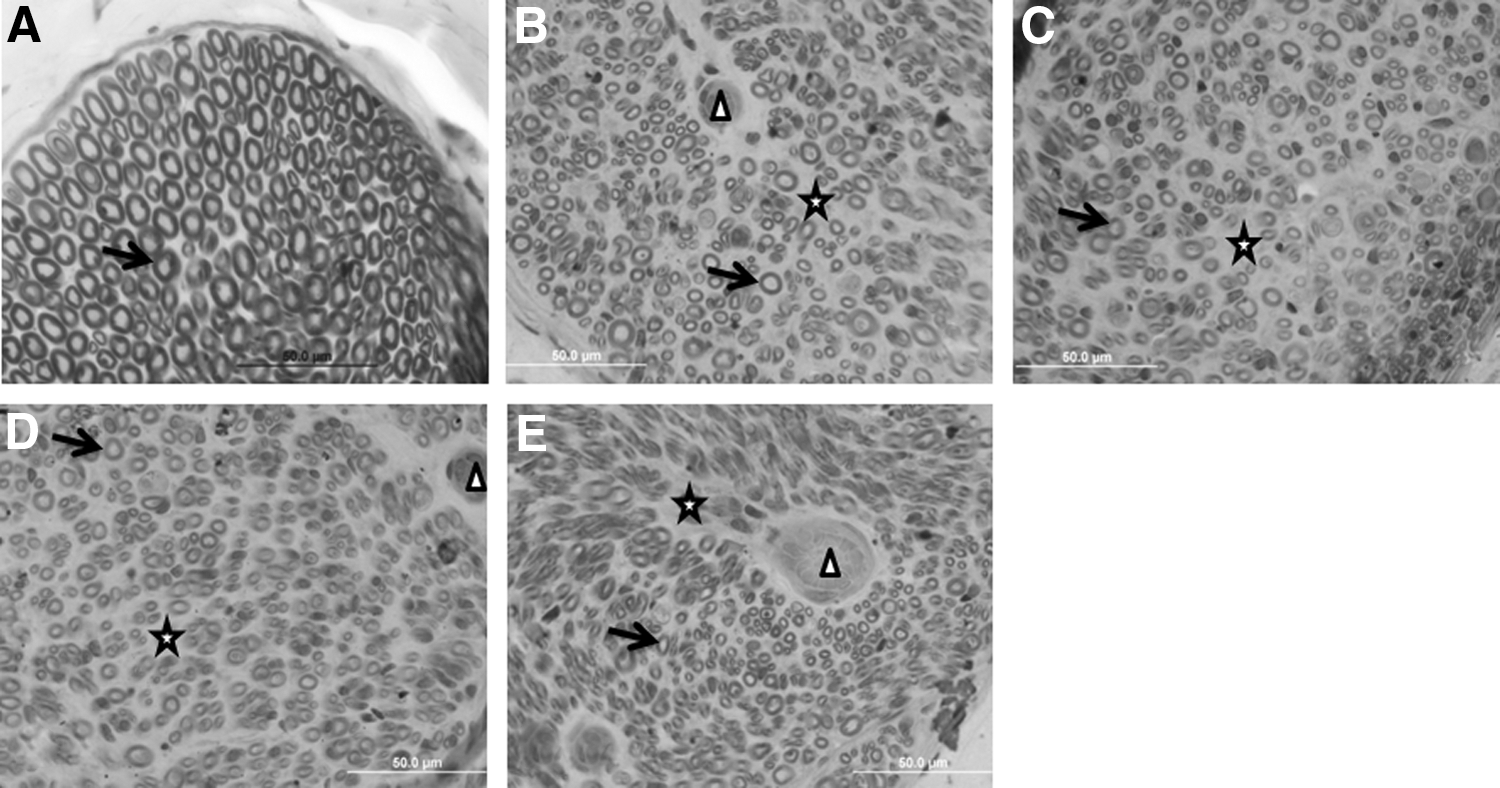
Animals 5 weeks postsurgery. Microscopic appearance of the buccal branch of the facial nerve in the groups:
Ten weeks after surgery, the CG presented myelinated fibers with regular appearance, similar to at 5 weeks postoperative. In the experimental groups, the myelinated fibers presented irregular arrangement and morphology distributed inside the nerve, adjacent connective tissue, and the presence of new blood vessels (Fig. 7).
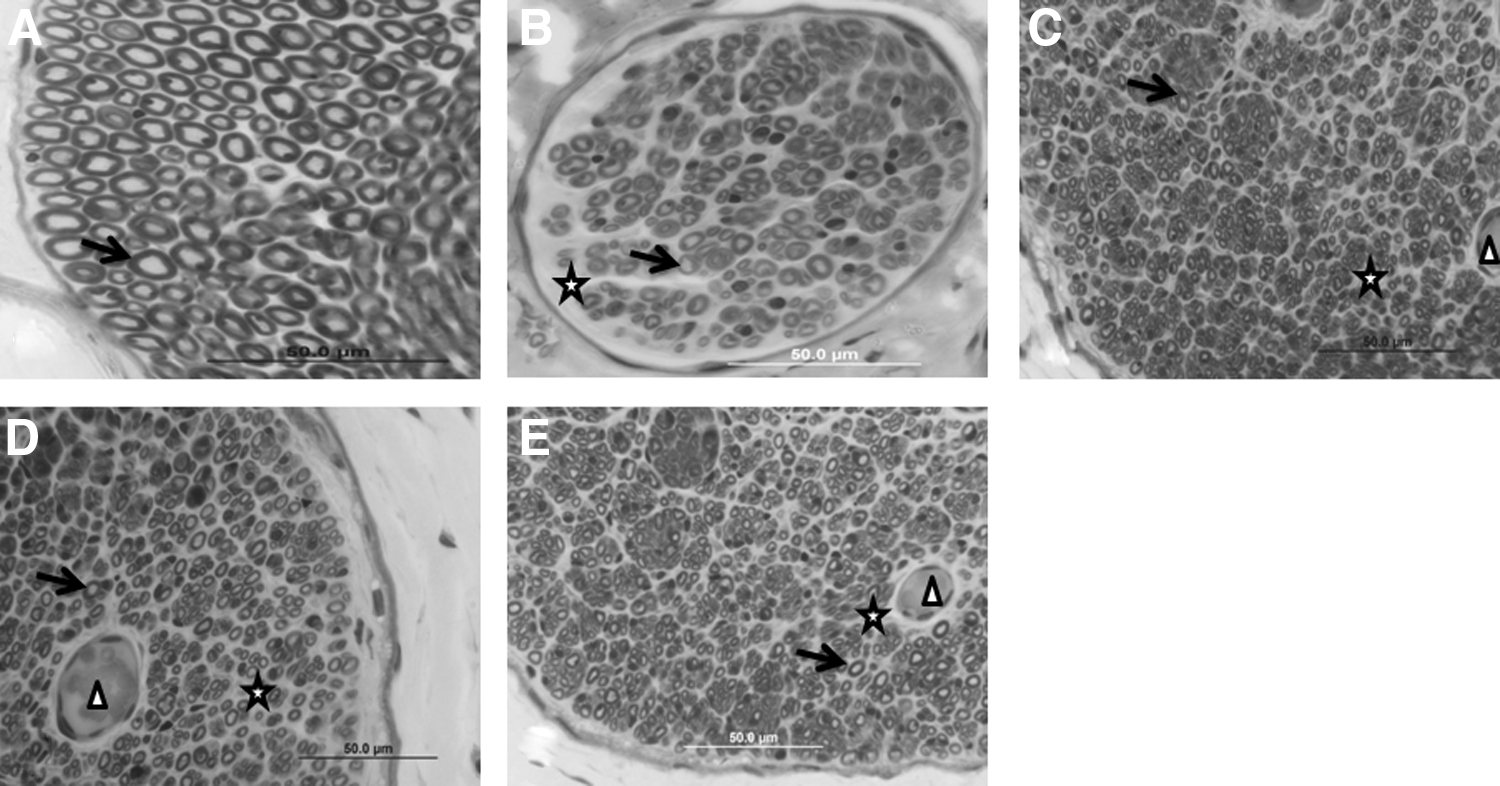
Animals at 10 weeks postsurgery. Microscopic appearance of the buccal branch of the facial nerve in the groups:
Quantitative assessment
With regard to the number and density of regenerated axons, there was a statistically significant difference (significance level α < 0.05) between the groups (SEG × LSEG; FEG × LFEG; p < 0.0001) at both 5 weeks (Table 2) and 10 weeks (Table 3).
Different lowercase letters (a, b) indicate significant differences among the groups by mean ± SD, unpaired t-test, and significance level α < 0.05, p < 0.0001.
FEG, fibrin experimental group; LFEG, laser fibrin experimental group; LSEG, laser suture experimental group; SD, standard deviation; SEG, suture experimental group.
Different lowercase letters (a, b) indicate significant differences among the groups by mean ± SD, unpaired t-test, and significance level α < 0.05, p < 0.0001.
Discussion
The present study aimed to evaluate the efficacy of LLLT on qualitative, quantitative, and functional aspects of the facial nerve regeneration process. It was concluded that LLLT enhanced axonal regeneration and accelerated the functional recovery of whiskers and that both repair techniques (suture and a new heterologous fibrin sealant) promoted the growth of axons.
End-to-end epineural suture is described as an effective technique for axonal regeneration in cases of neurotimic injuries that do not present tissue loss. 14,15 In the present study, the buccal branch of the facial nerve was sectioned and the stumps were approximated without exaggerated tension. End-to-end suture was then performed, leading to satisfactory results that are in accordance with previous research, in which the end-to-end epineural suture technique is considered the gold standard in cases of full injuries of the nerve with small lengths and no tissue loss. 14 –16
However, according to some studies, the repair of injuries involving peripheral nerves by means of sutures includes stump manipulation, leading to disruption of the axons and consequent formation of fibrosis. 40 In the search for an alternative technique or a technique that may be associated with suturing, fibrin sealants have been shown to be effective and their application is easier 32,37,41 –44 ; in addition, the surgery time for nerve repair is shorter. 32,37 During surgical procedures, fibrin sealant has presented good adherence and manipulation properties, as observed in other nerve injury recovery work. 19,29,37,42,43,45,46
In general, in all experimental groups, morphological observation presented a prevalence of myelinated fibers with irregular arrangement and diameters, showing that the nerve was in the process of regeneration. Consistent with these data, other research through histological analyses has shown no differences between the techniques. 16,47 At 10 weeks postoperative, the nerve fascicles presented a better arrangement in relation to the myelinated fibers when compared with 5 weeks, showing a progressive trend in the experimental groups.
Regarding the use of LLLT in the process of repairing nerve injuries, studies using similar protocols have shown that laser light causes the expression of neurotrophic factors, leading to increased regenerative rates and contributing to reduced inflammation and edema. 24,38 However, the parameters of irradiation, dosage, intensity, exposure time, and laser application methods vary widely among the different clinical reports on nerve regeneration. 47
The application protocol used in this study was based on previous work carried out, which showed the beneficial effects of LLLT in the regenerative process in nerve repair as in bone repair with the use of gallium-aluminum-arsenide that (when used under appropriate conditions) has good penetration capacity in tissues, improving and speeding the recovery process of the injuries. 32,33 Although the results of this study demonstrate the effectiveness of the laser, more research is needed for the standardization of protocols applied. 22,23,33,37,48,49
In facial nerve regeneration experiments, rats present anatomy that allows easy access to the nerve and ease of sectioning and repair, with subsequent functional analysis of whisker movement due to the dynamics of the animal justifying their choice for this experiment. These data are in agreement with the literature, demonstrating that it is possible to assess and quantify facial expressions from clinical observation using scoring scales. 27,28
For analysis of whisker movement, we chose 5 weeks and 10 weeks after surgery for the analysis of functional progress according to maximum regeneration of the axons. 50 The best results were found in the LSEG and LFEG at 10 weeks, with anterior position of the whiskers, similar to the CG, which is probably a consequence of the beneficial effects of laser therapy, the only difference in variable between the groups. The quantitative analysis, with higher averages and significant difference in the groups with LLLT, agreed with the functional assessment.
Electrophysiological tests may assist the functional assessment, which can be considered a limitation for this study. Further studies using other methodologies are recommended such as the new PBM therapy. In general, the buccal branch of the facial nerve reacts satisfactorily to both of the assessed techniques, and the LLLT promotes faster functional recovery of whisker movement, showing it to be a potential auxiliary alternative in the nerve regeneration process.
Conclusions
LLLT enhanced axonal regeneration and accelerated the functional recovery of whisker movement, and both repair techniques (suture and a new heterologous fibrin sealant) promoted the growth of axons.
Footnotes
Author Disclosure Statement
No competing financial interests exist.