
Abstract
Introduction
T
In recent years, multiple studies on the medicinal use of low-level light therapy (LLLT) have been carried out. The LLLT effects are used in dentistry, otolaryngology, purulent surgeries, and other medical fields. 15 –24 It has been proved that low-intensity LLLT not exceeding 100 mW/cm2 improves rheology, hemostatic properties of blood, and its circulation in lesion; it reduces inflammatory reactions and exudation, and activates the reparative processes in the tissue; it is bactericidal. 15 –24 However, this method of treatment has not been widespread in liver and gallbladder laparoscopy.
The purpose of this study was to evaluate the benefits of using LLLT to reduce the intraoperative adverse effects of LCE during the early postoperative period.
Materials and Methods
Patients
Two hundred sixty-three patients diagnosed with chronic calculous cholecystitis were the participants of a randomized, controlled, single-center, prospective, open-label clinical trial to be operated at Voronezh Clinical Hospital of Russian Railways JSC in 2013–2015. The criteria for inclusion were chronic calculous cholecystitis without clinical, laboratory, or instrumental signs of exacerbation, reference total bilirubin ranges, and clinically significant levels of ALT and AST in blood, which did not exceed the upper limit of the reference value more than 1.5 times. The exclusion criteria were acute cholecystitis; clinical, laboratory, and instrumental signs of liver failure and/or jaundice; and/or severe comorbidities (diabetes, cardiovascular, renal failure). The trial protocol was approved by the local ethics committee. Patients were randomized into test and control groups with the sealed code envelope method. All patients were informed about the approved treatment protocol and provided a written consent to participate in the trial. All patients received typical LCE performed without draining the bile duct.
Irradiation procedure
The patients in the test group of 131 individuals were exposed to single-time irradiation of the Svetozar-PRO device (Table 1; Fig. 1) for 2 min (approximately equal time on the gallbladder bed and porta hepatis) with the average irradiation power density 15–30 mW/cm2, specific dose—0.9–1.8 J/cm2, and distance to the object in the abdomen: ∼1–2 cm. The patients were exposed to irradiation of hepatic parenchyma during the surgery right after completion of the main phase of gallbladder removal (Fig. 2).
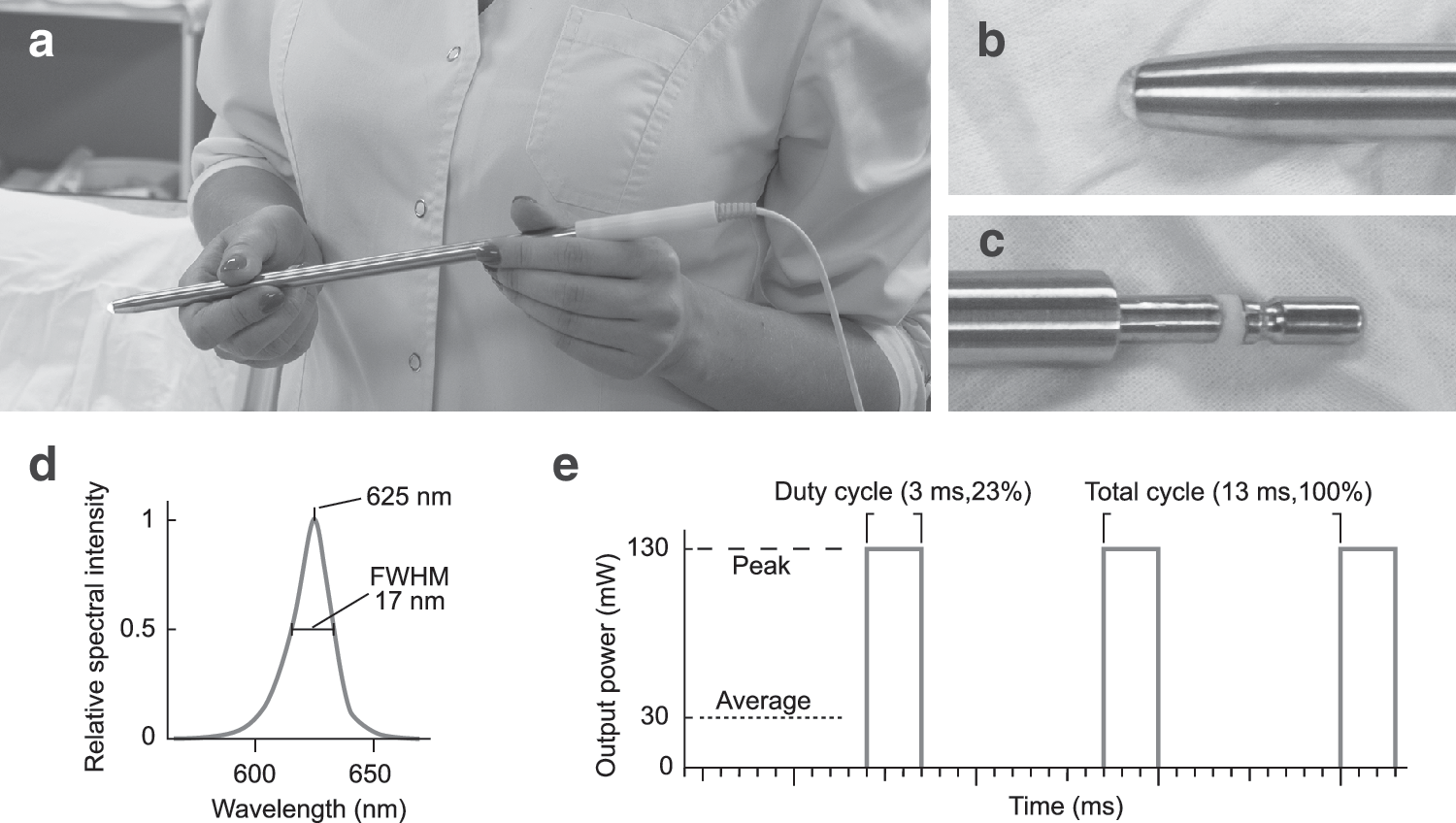
The emitter of the device Svetozar-PRO.
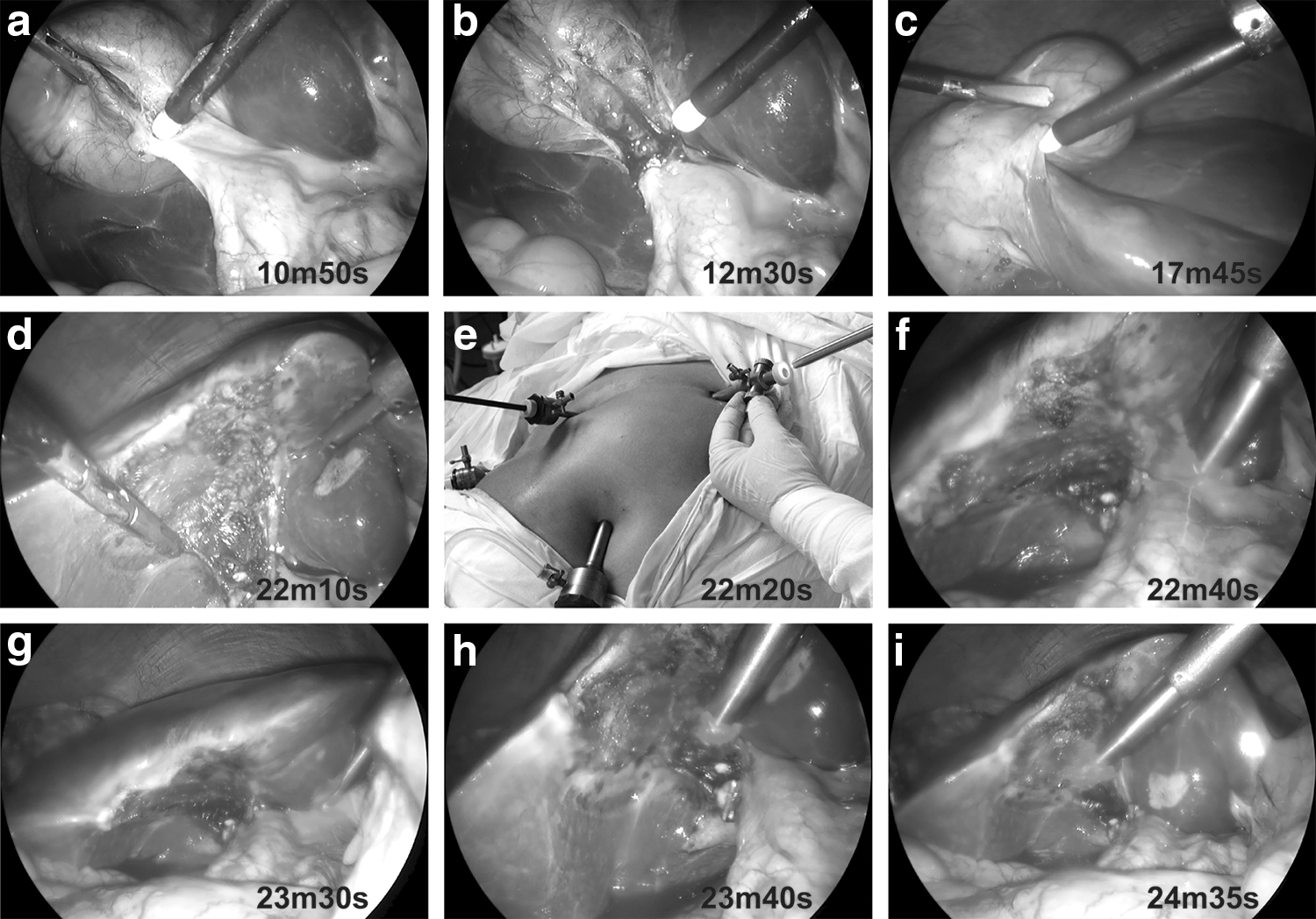
Typical cholecystectomy, followed by low-level light therapy on the porta hepatic and gallbladder bed. On each frame is shown the time from the start of surgery.
FWHM, full width at half maximum; PWM, pulse width modulated.
The control group of 132 patients was not exposed to irradiation. All other procedures during the surgery in both groups were exactly the same. Since surgery was performed under general anesthesia, the placebo effect was eliminated.
Blood tests
Subject to the provisions of the Russian Federation Government Specification,
25
the following blood parameters must be controlled in cholecystectomy: − for peripheral blood: red blood cell (RBC) level, hemoglobin (HGB), white blood cells (WBCs), and integral erythrocyte sedimentation rate (ESR) index; and − biochemical tests: total bilirubin, AST, ALT, and amylase levels.
Identical indicators were selected to evaluate the effect of LLLT on the intraoperative level of LCE undesirable effects on the liver in the early postoperative period. Blood test samples were taken for analyses the same day before surgery and on the third day after the surgery.
Statistical analyses
The statistical analyses were performed at test significance p < 0.05, where p is the probable coincidence of the two statistics. Due to limitations in total bilirubin, AST, and ALT values before the surgery, the initial index distribution is truncated. Under these conditions, chi-square criterion fitting has not revealed any known distribution related to all of the examined blood parameters. In this regard, the nonparametric statistical analysis was performed.
Results
Demographic and clinical characteristics
The demographic and clinical characteristics of groups of patients did not reveal any statistically significant differences before the surgery (Table 2).
Average values, standard deviations, and match probability p according to Student's t-test.
Changes in blood tests
After the surgery, the statistically significant changes were recorded for the patients in both groups (Table 3): median ESR values (an increase from 13 to 16 in the test group, p < 10−3, and from 14 to 25 in the control group, p < 10−3), ALT values (an increase from 23 to 54 in the test group, p < 10−3, and from 22 to 62 in the control group, p < 10−3), and AST (an increase from 23 to 37 in the test group, p < 10−3, and from 22 to 44 in the control group, p < 10−3). After the surgery, ALT values exceeding the upper standard limit were observed in 48% of patients in the control group and in 33% of patients of the test group. Distributions in quartiles for ALT, AST, and ESR are shown in Fig. 3. The RBC, HGB, WBCs, amylase, and total bilirubin levels did not have any significant changes compared with the baseline during the immediate postsurgery period in both groups or did not reveal any statistically significant differences between the groups.
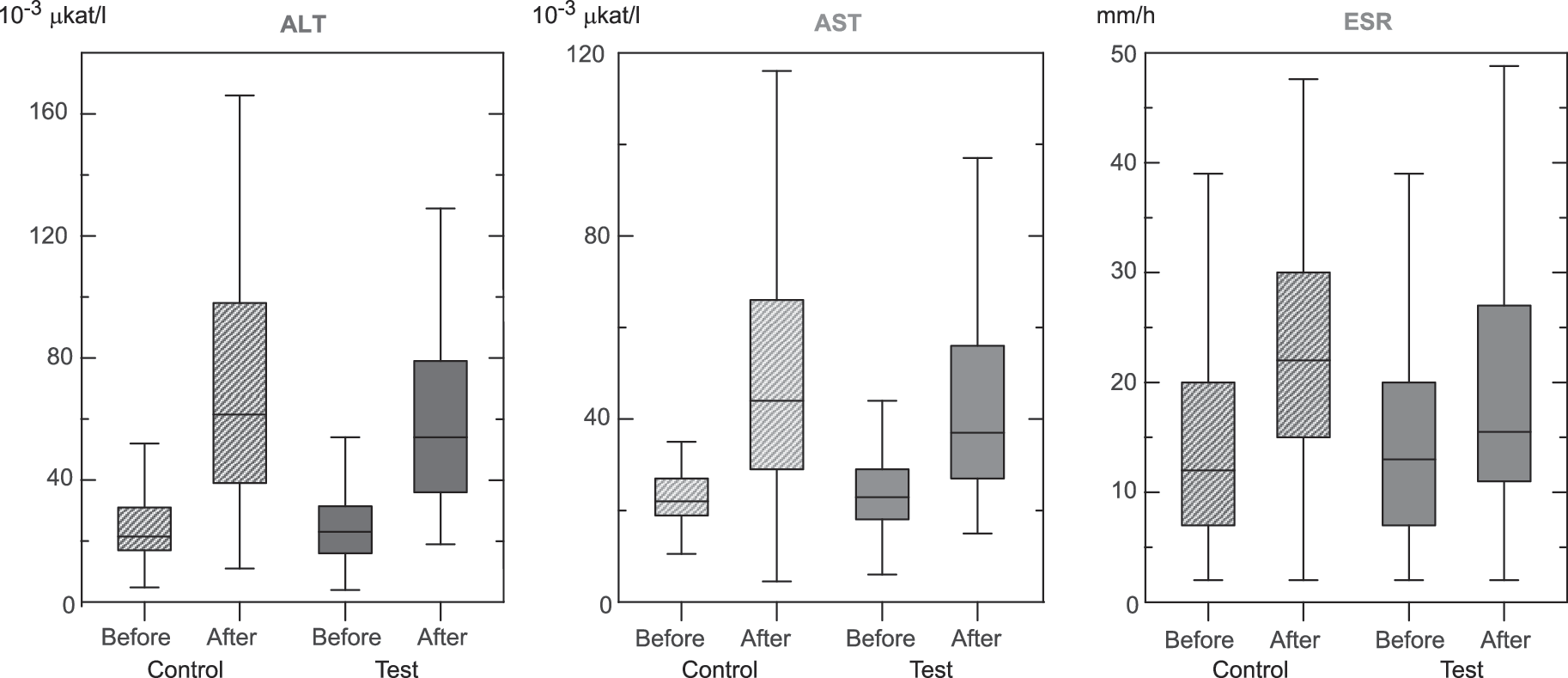
Blood data distribution: ALT, AST, and ESR for the control group (bar background) and test (solid background) group before and after surgery; whiskers—minimum and maximum; rectangles represent the lower quartile, median, and upper quartile. ALT, alanine aminotransferase; AST, aspartate aminotransferase; ESR, erythrocyte sedimentation rate.
CIMs are 0.95. Match probabilities p obtained in Wilcoxon test before and after the surgery within the group, and Mann–Whitney U-test between groups.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; CIMs, confidence intervals of the medians; ESR, erythrocyte sedimentation rate; HGB, hemoglobin; RBCs, red blood cells; WBCs, white blood cells.
Note that AST and ALT are not independent parameters. Without an acute pathology, they change simultaneously, and the AST-to-ALT ratio (the De Ritis ratio) on average varies by no more than two times. 26 With this in mind, the probability of the simultaneous significantly random difference of both indices in the two groups constitutes p ≤ 3 · 10−3 after the surgery, which is two times less than the lower limit of the significance criterion given the multiple corrections according to Hochberg 27 (the Bonferroni adjustment).
Thus, the statistic gain of AST and ALT was significantly lower in the intraoperative LLLT group than in the unexposed group. The significant difference in ESR growth, without the multiple comparisons, but combined with the impressive median changes in the test group (19%) compared with the reference group (83%), suggests that the buildup of index data will allow for more correct significant difference with reference to the multiple comparisons too. The statistically significant postoperative difference of other parameters between the two groups has not been found.
Discussion
This study investigated the effect of the intraoperative local low-intensity pulse width modulated (PWM) light exposure of the liver parenchyma on the condition of liver during the immediate postsurgery period after removal of the gallbladder in patients with LCE over the uncomplicated gallstone disease.
The disturbances of liver function after LCE, manifested in the growth of AST and ALT serum levels, were first described by Halevy et al. 3 in 1994 and later by many other authors. 4 –8,28 Among another factors contributing to liver functional abnormalities after LCE, the following effects have been mentioned: electrothermal treatment of liver parenchyma upon diathermy dissection and tissue hemostasis with subsequent formation of a large wound surface and necrosis, 9 –11 carbopneumoperitoneum, 6,8,29,30 mechanical impact on liver (gallbladder traction), 28 anesthetic treatment, 31,32 clipping branches, and coagulation of the right hepatic artery branchlets near the gallbladder bed. 33,34 The adverse hepatic effects of the above factors, although normally transient, may have long-term aftereffects in the form of strictures of the bile ducts, local cirrhotic changes in the liver parenchyma, and cholestatic manifestations, especially in patients with existing preoperative functional and/or organic liver lesions. 28
The results of our research confirm the negative impact of LCE on certain liver function, even in intact somatic patients with cholelithiasis and normal preoperative indicators of liver enzymes, ALT and AST. Patients in both groups showed an increase in level of these enzymes on the third day after surgery, while for 106 of 263 patients (40%), this growth has reached pathological values (for 63 patients from the control group and for 43 patients in the test group). The necrobiotic processes in the liver parenchyma, although over a limited area, reflected in ESR increase as an integral marker of the systemic inflammatory response and associated immune response.
To reduce the adverse hepatic effects during LCE, various authors suggest using bipolar coagulation instead of unipolar coagulation, ultrasonic energy, 11,12 hypothermic methods of hemostasis, 13,14 and performing surgery at a low pressure of pneumoperitoneum, 4,13,14 etc. (Table 4). However, the proofs of effectiveness of these methods have not met the EBM requirements; moreover, their use affects the practices in the key stages of surgery.
For the article: Redkin et al. “Reduce Adverse Effects of Laparoscopic Cholecystectomy with Pulse Width Modulated LED Light (625 nm, 76 Hz, 23% Duty Cycle).”
LLLT, based on the principles of photobiomodulation, 15 –19 has been increasingly used for treating various pathological conditions associated with tissue damage recently. Several studies in vitro and in vivo showed that LLLT has a beneficial effect on the various functions of cells and thus can improve the clinical parameters. 19 –21 In these studies, it was found that photobiomodulation affects a variety of biological processes, including strengthening mitochondrial respiration and adenosine triphosphate (ATP) synthesis, stimulating cell proliferation and regeneration of muscle tissue after injury, and accelerating collagen synthesis and wound repair. 15 –24
Basford research 22 found that photoradiation efficiency is virtually independent of the source of energy: be it laser, LED, or otherwise.
For the intraoperative irradiation of liver, we used modified equipment Svetozar-PRO with a laparoscopic emitter with which the liver can be exposed to irradiation from a distance of 2–3 cm. The combination of radiation parameters (625 nm, 76 Hz, 23% duty cycle, and about 30 mW power) for the optimal LLLT using red light was found earlier on the results of using this method in the treatment of oral diseases. 19 Then, it was considered the hypothesis of stress stimulation associated with temporary blocking of ATP production by mitochondria. That hypothesis allows to significantly reduce the number of observations, but even in this case, it required observations for 800 patients. We believe that common mechanisms of photobiomodulation LLLT with the red light allow us to suggest that parameters of the luminous flux found in the treatment of oral diseases will be optimal in other cases, including cholecystectomy.
In the group of patients with intraoperative LLLT, the gain of hepatic ALT, AST, and ESR was significantly lower than in the unexposed group (Table 3), which, in our opinion, points at a favorable effect of LLLT on the functions of liver, which suffered from the aggressive surgical environment during LCE.
We plan to continue research to extend the period of observations. Besides, we examined patients with preoperative liver function equal to or no more than 1.5 greater than normal, while the most risk of complications is for patients with more severe disorders of such functions. For such group of patients, we also plan to conduct a special study.
Conclusions and Summary
The study of the influence of intraoperative low-intensity PWM light emission on the condition of liver during the immediate postsurgery period after LCE proves that the method is significantly effective in eliminating the unwanted consequences of liver damage as a result of aggressive impacts during LCE surgery.
Footnotes
Acknowledgments
The coauthors wish to thank the following persons for their valuable assistance in the research and preparation of this article: Prof. T.N. Popova, Prof. A.A. Kunin, Prof. B.A. Zon, I.P. Dorovskoy, G.B. Yuldasheva, and V.N. Novikov.
Author Disclosure Statement
This study received support from Voronezh Railways Clinical Hospital with an equipment loan from Rosprominform, LLC. A. N. Redkin, V. V. Vdovin, and N. A. Malkina serve as acting surgeons for Voronezh Railways Clinical Hospital and terms of this arrangement have been reviewed and approved by the management of hospital in accordance with its policy on objectivity in research. V.M. Vahtel and P.A. Lukyanovich are researchers from Voronezh State University conducting engineering and material studies.