
Abstract
Introduction
T
To reduce treatment time, it is necessary to speed the rate of orthodontic tooth movement, by interfering with the alveolar bone remodeling process occurring in response to the application of orthodontic forces. 2,4,5
Corticotomy and injections of prostaglandins, osteocalcin, relaxin 1, and 25(OH) 2 D3 (the active form of vitamin D3) within the alveolar socket were found to accelerate orthodontic tooth movement. 6 However, corticotomy is an invasive procedure requiring highly skilled oral surgeons, while local injections of such substances are associated with local pain and discomfort. 4
Low-level laser therapy (LLLT) is a noninvasive technique with a wide range of applications in medicine and modern dentistry. 7 It uses low-powered laser light at wavelengths from 632 to 1064 nm, the red to near-infrared range, to provoke a biological reaction. LLLT accelerates cellular turnover 8 by increasing the vascular activity 9 and availability of adenosine triphosphate (ATP). 10
In the orthodontic field, the assumption is that such increased cellular metabolic activity may speed the rate of bone remodeling. 11,12 Prospective studies 4,13 –16 have investigated the effect of LLLT on the rate of orthodontic tooth movement; however, divergent results were found due to differences in the applied methodology, that is, type of laser, dosage, treatment time, and orthodontic biomechanics.
To date, no randomized clinical trials evaluated the efficacy of LLLT on the orthodontic treatment time. This pilot study aimed to assess if LLLT can reduce the time to align teeth in a sample of patients that underwent a nonextraction orthodontic treatment with a fixed appliance.
Materials and Methods
This randomized, with parallel groups (1:1), single operator, interventional pilot study was approved by the ethics committee of the Faculty of Medicine at the Milano-Bicocca University and was performed in observance of the Declaration of Helsinki. Subjects were selected and treated between January 2014 and March 2016 and all patients signed an appropriate informed consent.
Human subjects
Ninety-seven patients were selected from a larger pool of aspirants to orthodontic treatment at the Department of Surgery and Translational Medicine, Section of Orthodontics, Milano-Bicocca University. Patients were enrolled based on the following criteria: (1) age between 13 and 30 years, (2) completely erupted mandibular teeth, (3) Angle class I malocclusion, (4) lower 6–6 mild crowding measured on dental cast, (5) no spaces or diastema in the lower arch, (6) no ectopic teeth, (7) no treatment plan, including extractions or the use of intraoral or extraoral auxiliary devices, and (8) no previous orthodontic treatment. Thirty-six subjects (mean age 16.9) including 22 females (mean age 17.4) and 14 males (mean age 16.2) were finally enrolled.
Subjects were randomly allocated to receive orthodontic treatment with fixed appliance plus administration of LLLT (test group) or with fixed appliance only (control group). For randomization purposes, SPSS Statistics software (IBM Corporation, Armonk, NY) was used to generate an allocation sequence. Each subject was assigned a study number that was concealed until the date of bonding the fixed appliance.
Intervention
All participants were treated with 0.022-inch slot Empower self-ligating appliances (American Orthodontics, Sheboygan, WI) and Low Profile tubes (American Orthodontics) with MBT prescription. Both groups received the same archwire sequence, that is, a 0.014-inch thermal NiTi archwire (Thermal-Ti Lite, Form I; American Orthodontics) followed by 0.016 × 0.022-in and 0.017 × 0.025-in thermal NiTi archwires (Thermal-Ti Lite, Form I; American Orthodontics). The archwire sequence progressed only if full bracket engagement was easily feasible, that is, without forcing the rectangular wires throughout the bracket system. Control visits were scheduled at intervals of 4 weeks to check clinical progress and adjust the appliance, if necessary.
During the same appointment, LLLT was administered to the tested group using a Diode laser emitting infrared radiation at 980 nm (Wiser; Doctor Smile–Lambda Spa, Brendola, VI). The plane wave optical fiber (AB 2799; Doctor Smile–Lambda Spa) dispensed a beam spot size of 1 cm2 and irradiation was administered by positioning the optical fiber tip along the mandibular dental arch (1.5 cm as minimum on defocalization, as prescribed by the producer). Specifically, four dental segments (right first premolar-canine, right lateral-central incisors, left central-lateral incisors, left canine-first premolar) were consecutively irradiated for 8 sec and two dental segments (right first molar-second premolar, left second premolar-first molar) for 9 sec, for a total of 50 sec (Fig. 1). The procedure was repeated 3 times at intervals of 2 min. All irradiations were done with an output power of 1 W at a continuous wave. The total energy density for the entire mandibular dental arch, corresponding to an exposure time of 150 sec, was 150 J/cm2, (1 J/cm2 per second) including 27 J/cm2 for each of the two first molar-second premolar segments and 24 J/cm2 for each of the remaining four dental segments.

LLLT procedure used in this study. Irradiation was administered by positioning the optical fiber tip along the mandibular dental arch, at 1.5 cm as minimum on defocalization. LLLT, low-level laser therapy.
All patients signed the informed consensus form to receive LLLT. Brackets bonding, clinical controls (including the adjustment of the appliance and archwire), and LLLT administration were performed by the same expert operator (G.C.).
Assessment of dental alignment treatment time
The Little's irregularity index 17 was used to quantify the initial amount of crowding in the lower arch from 6 to 6 (11 contact points). The same operator (G.C.) performed the measurements on initial dental casts by means of a digital caliper (Absolute Digimatic IP67; Mitutoyo Europe GMBH) and all values were reported on a spreadsheet. To evaluate the reliability of the analyses, 15 randomly selected dental casts were remeasured by the same operator 4 weeks later. A paired sample t-test was applied to the first and second measurements and no differences were found.
To assess the alignment treatment time in both groups, the date of brackets bonding (T1) and the date when complete resolution of crowding was established (T2) were recorded. Alignment treatment time was defined in days as T2 − T1 and reported on the spreadsheet along with the total number of monthly scheduled control visits. The resolution of dental crowding (T2) was assessed by the same expert operator (G.C.) basing on visual inspection of correction of the 11 mandibular interproximal contacts.
Statistics
Descriptive statistics was carried out to analyze demographic and clinical characteristics of the sample of this study. For the comparisons between the two groups, Student's t-test and chi-square test were used, respectively, for numerical (age, crowding) and categorical (gender) characteristics.
Normal distribution of data of treatment time duration (days and number of appointments) was preliminarily checked using the Shapiro–Wilk test (
The Log-rank (Mantel-Cox) Test for survival analysis was used to assess treatment duration (days) in both test and control groups. Survival analysis is used when the outcomes are prospectively evaluated as the time elapsing (time-to-event data) before an event is experienced (i.e., the resolution of dental crowding in this study). Mann–Whitney U tests was performed to compare the total number of appointments from T1 to T2 between the two groups.
Results
The CONSORT flowchart is reported in Fig. 2. From 97 subjects assessed for eligibility, 36 were enrolled in this study. All showed good compliance during the treatment, hence no discontinued interventions were detected. No differences were found between the two groups for age, sex, and amount of crowding (Table 1).
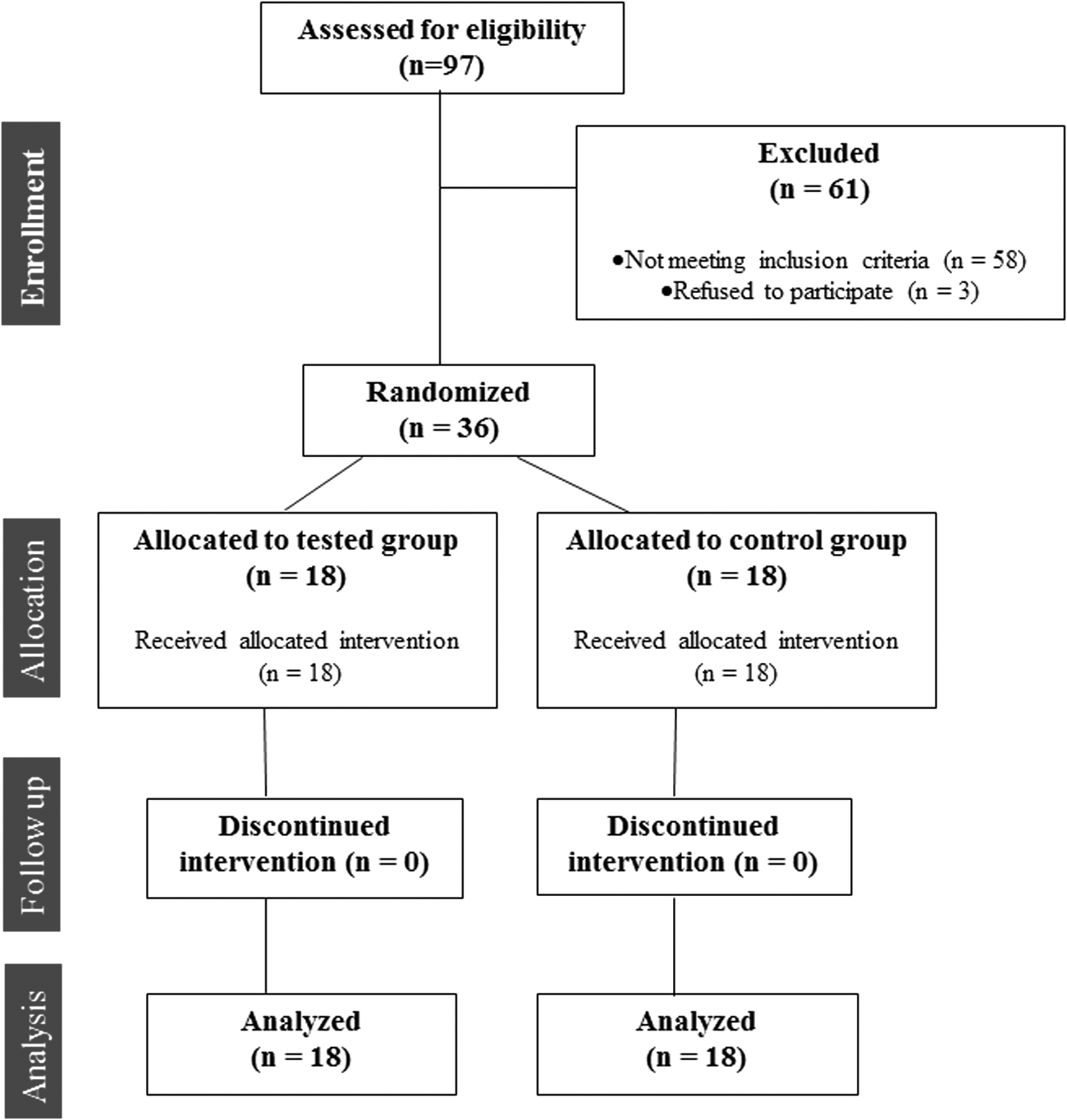
CONSORT flowchart diagram of the clinical trial.
Control = orthodontic treatment with fixed appliance. Test = orthodontic treatment with fixed appliance and low-level laser therapy.
Significance for comparison of group means calculated by paired t-test or chi-square test.
NS, not significant.
The log-rank (Mantel-Cox) Test for survival analysis showed that the average time for dental alignment was significantly shorter (p < 0.001) in the tested group (211.8 days) compared to the control (284.1 days) (Table 2). Consequently, test group needed significantly (p < 0.001) less monthly scheduled control visits compared to the control group (7 vs. 9.5 visits, as median values), as reported by Mann–Whitney U test (Table 3). Figure 3 shows the Kaplan–Meier survival curves for the two treatment groups. The separation between the two curves indicates that the treatment time differs in a statistically significant manner between test and control groups.
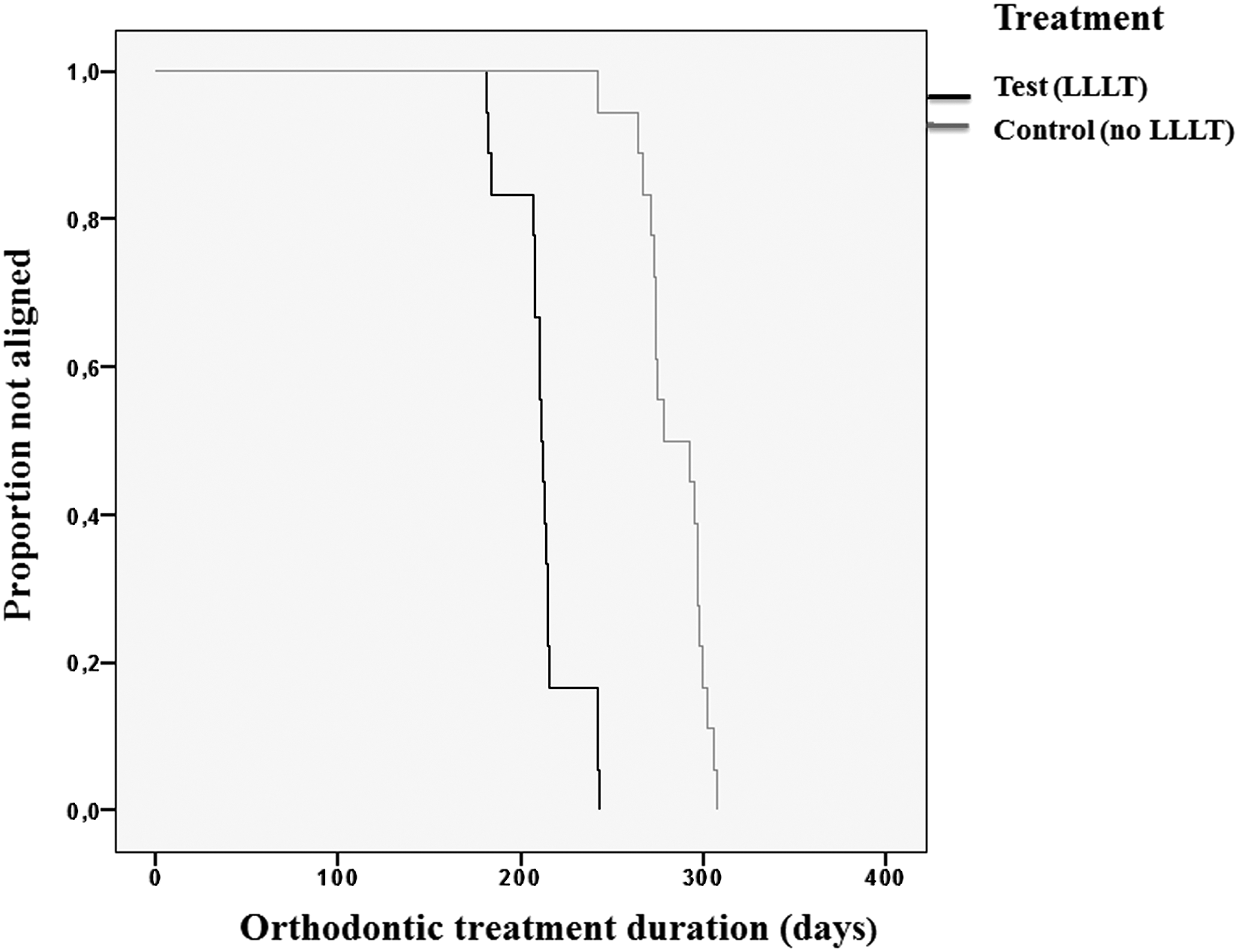
Kaplan–Meier survival curves for test and control group. The separation between the two curves indicates that the treatment time significantly differs between test group and control group.
p Value based on log-rank (Mantel-Cox) test for equality of survivor functions.
p Value based on Mann–Whitney U test.
Discussion
To the best of our knowledge, this is the first randomized prospective interventional study that evaluates the effect of LLLT on the treatment time to align teeth, in subjects undergoing a nonextraction orthodontic treatment plan.
In this study, the mean time needed to resolve mandibular dental crowding was found to be significantly shorter in the laser-stimulated group (211.8 days) than in the nonstimulated group (284.1 days). Because sample variables were equally distributed between the two groups, the results of this pilot study suggest that LLLT might increase the efficiency of orthodontic treatment with fixed appliance.
These findings suggest the crucial role of the biostimulatory mechanisms of LLLT on bone remodeling. At the cellular level, laser light exposure activates the cytochrome c oxidase which, in turn, increases the production of mitochondrial ATP. 10 During orthodontic movements, higher levels of ATP may accelerate cellular turnover (osteoclast, osteoblast, and fibroblasts) due to the increase in metabolic activity. 11,12
LLLT was found to increase cellular viability and the expression of osteocalcin in the tension areas of periodontal ligament, suggesting that bone formation can be rapidly initiated in this area after the application of orthodontic forces. 18
LLLT also stimulates angiogenesis, 9 which is involved in the bone remodeling process. This aspect acquires particular importance in adult patients where tissue blood supply and cellular turnover are decreased and the treatment is commonly associated with a slower and more painful initial tooth movement. 19
The LLLT protocol used in this study included one intraoral administration per month with a total energy density of 150 J/cm2. This is in the monthly range of energy density (150–200 J/cm2) found to accelerate the retraction of canine in two prospective studies. 14,15 However, the different methodology applied, that is, number of teeth irradiated, type of orthodontic movement, and orthodontic biomechanics involved, makes the comparison among these findings unreliable.
The benefits of LLLT are dependent on laser settings, mostly the wavelength and energy density that can determine different penetration depth and biostimulation effects. 20 –24 About the dosage, LLLT seems to influence the rate of orthodontic movement in a dose-dependent manner as reported by previous in vitro and in vivo studies. 4,12 –16,25,26 However, two recent meta-analyses 7,27 reported that it is still not possible to precisely draw conclusion on this aspect, due to the low quality of evidence found among such studies.
The ideal dose of LLLT is still a concern because it is not possible to precisely calculate the light exposure of the cells due to the different amount of energy density lost during penetration through facial structures. 4
Indeed, the advantage of intraoral administration of LLLT over extraoral protocols is the possibility to obtain similar clinical outcomes at lower energy density because it is not necessary to compensate for the absorption of light by the soft tissue of the cheek. 28
Our findings are in agreement with those of a recent nonrandomized preliminary study 28 where dental alignment was faster in the photo-biostimulated group (48 days, alignment rate = 1.27 mm/week) than in the control group (104 days, alignment rate = 0.44 mm/week). However, the alignment treatment time is notably longer in the present investigation (test group = 284.1 days, control group = 211.8 days). However, the LLLT dosage and the intervention schedule were different between the two studies. Shaughnessy et al. 28 tested a daily administration of LLLT (3.8 min per arch/day) with a mean energy density of 9.3 J/cm2, that is, an approximate value of 260 J/cm2 per month (not reported by the authors), using an intraoral device. On the contrary, our protocol was based on a single session of LLLT per month that produced a total energy density of 150 J/cm2.
Nevertheless, a comparative assessment between the two protocols would be unreliable due to some relevant methodological differences found in the two studies: (1) the averaged amount of initial dental crowding was greater in our investigation (8.9 vs. 6.7 mm), (2) in the study of Shaughnessy, the assessment of resolution of dental crowding was limited to the six anterior teeth, and (3) our archwire sequence included rectangular NiTi wires due to the necessity to resolve premolar and molar rotation that is difficult to obtain using only round NiTi archwires. 5,29
In fact, the treatment time discrepancy is consistent also between the control groups of the two studies (211.8 vs. 104 days). Further clinical trials, with parallel arms, are necessary to elucidate the appropriate LLLT protocols with regard to dose, energy, as well as number of sessions that can enhance the efficiency of orthodontic treatment. Ideally, future studies need to be better standardized as to patient age, size, and orthodontic biomechanics used. 30
The extension of the orthodontic treatment affects the overall patient's chair time and, consequently, the management of orthodontic clinical practice. 31 In this study, patients who underwent LLLT needed less control visits (7 visits, as median value) compared to the control group (9.5 visits, as median value). Thus, these data could be positively evaluated from a clinical and managerial perspective.
Therefore, the preliminary data suggest that LLLT could be routinely administered to orthodontic patients to reduce orthodontic treatment time without using more invasive and expensive procedures such as corticotomy and local injections of biomodulators. 7 –11
Limitations
The results of this study must be considered with caution due to the small number of patients enrolled as well as the intrinsic limitations of a pilot study design. Moreover, the data recorded are limited to the phase of dental alignment and must not be linked to the overall orthodontic treatment time. Finally, the results of this pilot study support the clinical validity of performing clinical trials to confirm the efficacy of LLLT in orthodontic dental alignment.
Conclusions and Summary
Within the limits of this pilot study: • Intraoral administration of LLLT significantly increases the efficiency of orthodontic treatment during dental alignment. • Patients who underwent LLLT during orthodontic treatment required less control visits (7 visits) compared to the control (9.5 visits).
Footnotes
Authors Disclosure Statement
No competing financial interests exist.