
Abstract
Introduction
I 1. Nonmuscle invasive bladder cancer (NMIBC): (Cis, Ta, T1) 2. Muscle invasive bladder cancer (MIBC): (T2–T4)
It is generally assumed that 75–85% of newly diagnosed BCa belong to the NMIBC group, and in most cases, they can be treated by transurethral resection of bladder tumor (TURBT). 2 NMIBC is characterized by a high recurrence rate and risk of progression to cancer infiltrating the muscle of the bladder or by progression from a low-grade to a high-grade tumor. 3 One form of cancer that is regarded as a serious problem in the field of oncologic urology is flat high-grade Cis, which can occur in the bladder as local or disseminated forms, or together with other types of BCa. 4,5 Cis has an exceptionally high recurrence rate of as much as 45% in fFU [first follow-up] cystoscopy 3 months after TURBT, 6 and a risk of progression of about 50%: much higher than other types of NMIBC. 7 Currently, white light cystoscopy (WLC), often supported by urine cytology, is considered the “gold standard” in the diagnosis of Cis. 8
Another problem occurring as a result of the use of insufficiently sensitive diagnostic equipment is dysplasia. According to the latest classification proposed by the WHO, dysplasia G3 is a state that is characterized by the same severity as Cis. 9 High-grade dysplasia, which is a precursor of Cis, is often located in apparently normal bladder mucosa and can be easily overlooked during standard cystoscopy. 10,11 It has been demonstrated that in patients with Ta BCa, the most aggressive cancers develop from areas that are adjacent to Cis, 12 and performing random biopsies does not result in significant improvement in the detection of this type of cancer. 13
The unsatisfactory sensitivity of WLC in detecting cancers has required the search for alternative diagnostic approaches. One of them uses minimally invasive molecular biology techniques to identify traces of cancer in the urine or blood. However, this approach does not allow the location and extent of the tumor to be determined. 7 A number of studies over the past 20 years have looked at another approach, photodynamic diagnosis (PDD), to offer greater detection and treatment efficacy than WLC in BCa patients. Finally, narrow-band imaging (NBI) is an invasive diagnostic method adopted from gastroenterology, where it has been used to detect colorectal polyps, high-grade dysplasia, and metaplasia of Barrett's esophagus. 14,15 In the field of urology, it has proved to be an effective way to increase the visibility of capillaries and pathological changes in the bladder urothelium. 16
This article is intended to familiarize the reader with the theoretical principles of PDD and NBI, and to present the current state of medical knowledge on these two relatively new tools in the diagnosis and treatment of bladder cancer.
Materials and Methods
A nonsystematic review of literature was performed. PubMed was searched for articles on the use of PDD and NBI in bladder cancer.
Photodynamic Diagnosis
PDD improves visualization of bladder tumors compared with WLC. The method requires application of a photosensitizer into the bladder before cystoscopy. In situ administration of the photosensitizing agent demonstrates a better safety profile than oral administration, which is associated with a high rate of adverse events, including extended photosensitizing. 17,18 Currently, two agents are in use: aminolevulinic acid (5-ALA) and its more lipophilic ester hexaminolevulinate hydrochloride (HAL), both of which induce the accumulation of protoporphyrin IX in the cells. The test operates on the principle that cancer cells demonstrate stronger absorption and extended excretion of protoporphyrin than normal bladder tissue, 19 and when exposed to light at wavelengths of 375–440 nm, they give off a red fluorescence, whereas the intact tissue appears blue. 20 Currently, the majority of studies evaluating the suitability of PDD are based on the use of HAL, rather than 5-ALA, due to its greater selectivity for tumor tissues, brighter fluorescence, and shorter duration in the urinary bladder needed before cystoscopy. 21 A comparative study of WLC and PDD, based on 5-ALA, by Schumacher et al. revealed no significant differences between these two techniques in terms of detection and time to tumor recurrence, thus indirectly confirming the superiority of HAL over 5-ALA. A clinical trial evaluating PDD after oral administration of 5-ALA showed its safety, as among 181 included patients there was just 1 case of grade 1 (pruritus) adverse drug reaction. 22
Current research indicates that HAL PDD improves the sensitivity of diagnostic cystoscopy, which is reflected in reduced BCa recurrence rates after treatment. 23 The sensitivity of WLC is estimated to be 77%, whereas that of HAL PDD is significantly greater (−96%). 24 However, as is often the case, this greater sensitivity is acquired at the expense of specificity. The rate of false positive results was significantly higher in HAL (37%) than in WLC (26%). 24 One of the major disadvantages of PDD is that a high percentage of identified and electroresected lesions are later found to be benign on pathological examination. The main risk factors for the presence of false positive results are caused by bladder inflammation, urothelium hyperplasia, scarring, dysplasia, and performing the examination shortly after Bacillus Calmette-Guérin (BCG) therapy or viewing the mucosa at a tangential angle. 25,26 Therefore, in the latest elaboration carried out by Witjes et al., PDD was not recommended to be performed in a period of less than 6 weeks after TURBT, nor during BCG therapy. 27 Other PDD restrictions include the high cost of examination and longer duration of the procedure compared with WLC. 7 However, Dindyal et al. found that the costs associated with the purchase of both hardware and photosensitizing agents are recouped if used for follow-up examination for longer than a period of least 1 year after BCa treatment. 28 Similarly, Malmström reported that the use of HAL cystoscopy during the first TURBT, and in all TURBTs after BCa recurrence in the first year of follow-up, helps to limit the number of performed cystectomies and TURBTs, which, in turn, leads to significant cost savings. 29
The past 15 years have seen the publication of a substantial number of articles about PDD. They initially focused on its sensitivity and specificity in the diagnosis of BCa, and they then moved on to evaluating the effectiveness of electroresection and recurrence rates of bladder tumors after surgery. Schmidbauer and al. compared HAL-PDD with WLC in patients with high-risk BCa, focusing on the detection of Cis. In a group of 286 patients, 83 cases of Cis were detected, 96% of them with the use of HAL, and 77% by WLC. This represents an increase of 28% in Cis detection rate using fluorescence compared with standard cystoscopy. These differences were even more pronounced when CIS changes detected in patients without concomitant exophytic tumor were taken into account. Overall, the use of HAL allowed 67% more Cis lesions to be detected than when using WLC, and when detecting all changes suspected of being neoplastic proliferations, sensitivity was found to be 97% for HAL and 78% for WLC. The frequency of false positive results was lower than that found in other studies, with 13% recorded for PDD and 10% recorded for WLC. 17
In a study of diagnostic cystoscopies performed in 776 patients, Stenzl et al. detected at least one more Ta/T1 tumor in 16.9% of cases when using PPD HAL than when using WLC. In addition, 32% of Cis cases were diagnosed as only using HAL, indicating 46% better detectability in comparison to WLC. False positive results were 12% versus 11% for HAL and WLC, respectively. 30 Colombo et al. focused on the value of PDD in the diagnosis of patients with previously diagnosed Cis. Among the patients in whom recurrence of Cis was detected, 77.7% of cases were diagnosed by the use of PDD only, and 22.2% were diagnosed by both PDD and WLC. The frequency of false positive results for the PDD was 33.3% (35% for the 5-ALA and 22.7% for the HAL). 7 In a study of the early detection of dysplasia and Cis in high-risk patients, Blanco et al. found HAL to have a sensitivity of 90.1% and a specificity of 87.5%. 31 Stenzl found that 46% of studied Cis patients had at least one Cis change detected by HAL, and 32% had Cis detected only with the use of HAL. The incidence of relapse (or incomplete resection) 9 months after TURBT was detected in 47% of cases after HAL-TUR and in 56% after WLC-TUR, giving a 16% relative decrease in the frequency of tumor recurrence in favor of HAL. 32
An examination by Geavlete et al. that dealt with 176 patients suffering from NMIBC found PDD to have 95.5% sensitivity versus 85.2% for WLC. Recurrence rates observed during reTURBT were 11.1% for HAL and 31.2% for WLC. The study also found the incidence of recurrence for patients suffering from tumors with a diameter <3 cm, to be 9.1% after HAL-TUR and 20% after WLC-TUR. In multiple tumors or those with a diameter >3 cm, the rates of recurrence were 15.8% versus 36.1%, for HAL and WLC, respectively. 33 Drâgoescu et al. found the diagnostic sensitivity of HAL PDD to be 92.8% and that of WLC to be 79.5%. An analysis of the recurrence rate after TURBT found that the rate of BCa recurrence after HAL-TUR gradually fell over the course of 1 year follow-up when compared with WLC-TUR, with it being 9.1% lower after 3 months and 27.3% lower after a year. More complete results are presented in Table 1. 23 The results of a large (551 participants), prospective, randomized study carried out by Grossman et al. also associated better results with PDD. The median time to recurrence of BCa was 7 months longer (p = 0.04) in the PDD group than in the WLC group. 34
HAL, hexaminolevulinate; PDD, photodynamic diagnosis; WLC, white light cystoscopy.
It seems reasonable to present the data collectively, as although the criteria for allocating patients to participate in the studies mentioned earlier differed, the patients suffering from BCa presented the same general profile. PDD was found to produce higher scores than WLC for both the sensitivity of detected tumors (WLC 77–85.2% vs. PDD 92.8–97%) and the efficiency of TURBT measured by the frequency of relapses after 9 months after surgery (WLC 36.4–56% vs. PDD 13.6–47%). The authors of these studies concluded that PDD is more effective than WLC, especially in the detection of Cis tumors.
These findings are further supported by a meta-analysis by Burger et al., which found PDD to detect 40.8% more Cis lesions than WLC. Further, in 26.7% of patients, Cis was observed only under BLC (Blue Light Cystoscopy) (p < 0.001). 35 These results are reflected in recommendations given by Witjes et al., who propose that PDD should be performed in all cases of primary TURBT, and in cases when patients are positive for urine cytology but no tumor has been detected by WLC. 27
Narrow-Band Imaging
NBI is a new method of imaging used in oncologic urology that is intended to improve the visibility of suspected changes in the urothelium during cystoscopy. In contrast to PDD, it does not require the instillation of a photosensitizer into the bladder, resulting in reductions in the time and costs associated with the procedure. White light is filtered to two beams of 425 and 540 nm wavelengths, which are strongly bound by hemoglobin. This increases the contrast between highly vascular tumors and normal urothelial tissue (Fig. 1). 36,37 A special indication for the use of NBI is the presence of a tumor diameter greater than 3 cm, for which wide infiltration of the bladder mucosa is often unnoticeable under the WLC. 38 Reports have noted a subjective improvement of image quality and better visibility of the bladder structures, giving the urologist the impression of a three-dimensional image. However, as this technique is relatively novel, it is not yet known whether the factors responsible for the false positives in PDD will play an equally important role in NBI. 39
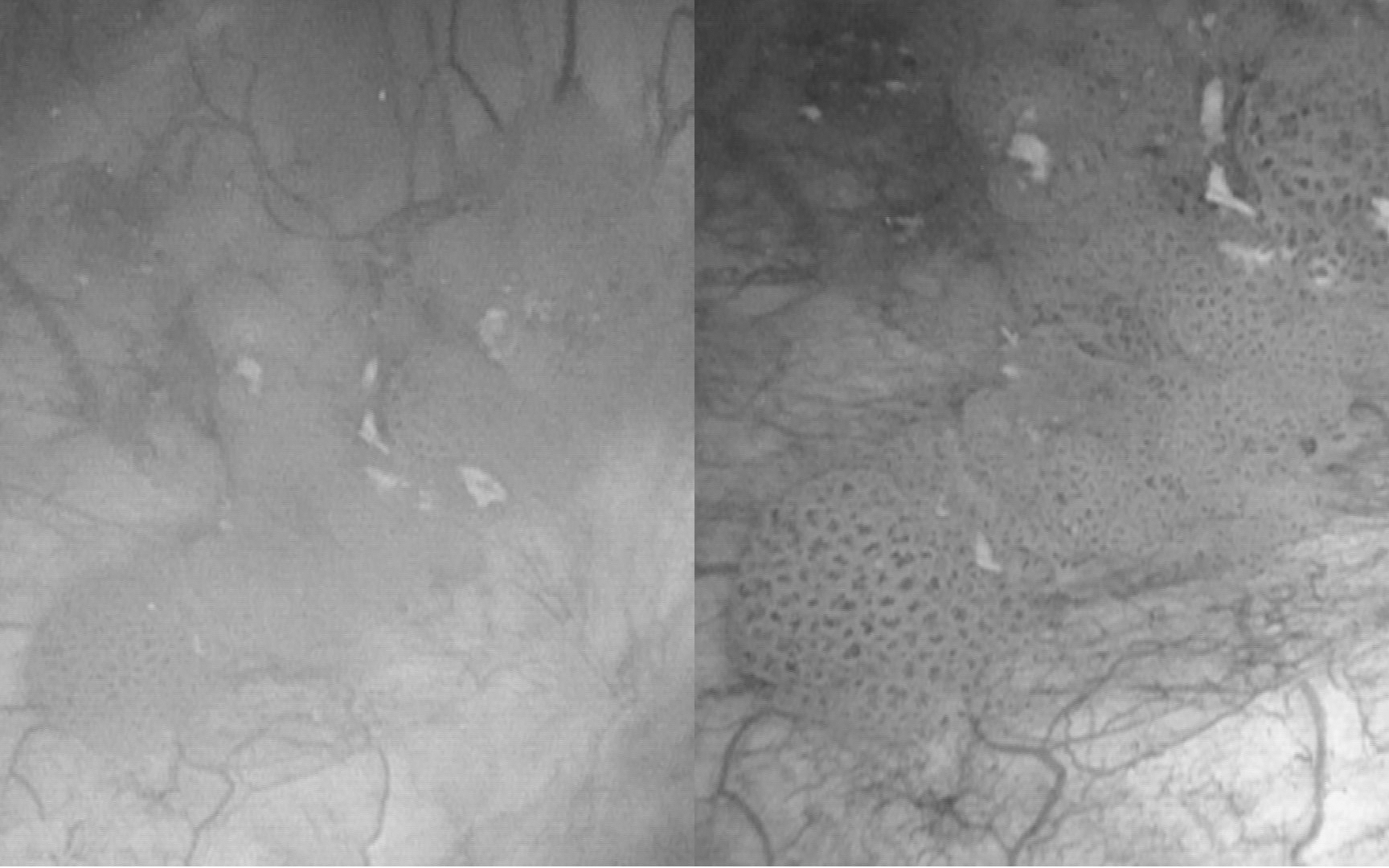
Bladder tumor seen in white light cystoscopy (left) and in narrow-band imaging (right).
Reports based on small populations of patients indicate that using NBI has greater sensitivity to detect BCa compared with WLC. Chen et al. reported the sensitivity of NBI and WLC for detecting NMIBC to be 97.9% and 88.8%, respectively. 40 Geavlete et al. found NBI to have a significantly higher potential to detect bladder cancer than WLC. NBI and WLC were found to have 96.2% and 87.2% sensitivity for all cases of NMIBC, and 100% and 66.7% sensitivity for detecting Cis, respectively. The number of false positive results was slightly higher for NBI than WLC, but the difference was not statistically significant. 41 A meta-analysis performed by Zeng found the sensitivity of NBI to be 94% for the detection of all bladder tumors compared with 87% for WLC. When only Cis detection was taken into consideration, the differences between these two techniques were even more pronounced, with NBI demonstrating 93% sensitivity compared with 77% for WLC. 42
Cauberg et al. compared the frequency of bladder cancer recurrence after transurethral resection by using NBI and WLC. The cancer was found to recur within 3 months in 15% of patients treated with NBI-TUR and in 30.5% of cases treated with WLC-TUR. The absolute difference in RR-fFU was 15.5% in favor of NBI. This is the first study evaluating the relationship between radicality of resection and the frequency of early recurrence with the use of NBI, 43 and these initial results have since been confirmed by other studies. In the first year of follow-up after TURBT carried out by using NBI, the risk of bladder cancer recurrence fell by 10%. 44 According to the comparison of TURBT under conventional WLC and NBI, performed by Kobatake, the procedure done with the use of this optical enhancement technology is associated with a lower recurrence rate after 1-year follow-up (39.7% vs. 21.1%; p = 0.016). 44
The number of false positive results for NBI ranges from 32% to 36%. NBI demonstrates reduced usefulness in case of severe hematuria. The quality of cystoscopy can be impaired by the presence of blood in the bladder or, more precisely, the hemoglobin contained in the red blood cells, which absorbs the light produced by the cystoscope and significantly impedes proper evaluation of the bladder mucosa. 45
So far, many articles have shown better outcomes of procedures performed under NBI compared with WLC in the matter of detection and recurrence rate. However, NBI-TUR seems to have little effect on another major challenge associated with BCa, that is, progression. According to the data presented by Shadpour et al., the tumor progression index was not significantly reduced with NBI compared with WLC. 46
To date, relatively few studies evaluating the diagnostic and therapeutic value of NBI have been published. Nevertheless, the articles that are available are rather optimistic; however, further research is needed to precisely define the role of NBI in endoscopic oncology.
Comparison of PDD and NBI
There are few articles directly comparing PDD and NBI. Naya et al. were the first who compared these two procedures in the same group of patients with flat urothelial lesions. The study showed little advantage in favor of PDD, which revealed all cancer lesions, missing 4% of dysplasia. At the same time, NBI failed to detect 5% of Cis and 10% of dysplastic lesions. Sensitivity for Cis and dysplasia detection was 91.6% for PDD and 62.5% for NBI. 47 Another study performed on the larger group of patients (n = 171) by Drejer et al. confirmed higher sensitivity of PDD and NBI than WLC in the detection of Cis and dysplasia. Although the direct comparison between PDD and NBI did not reveal any significant differences in their sensitivity or specificity, there still seems to be a need of performing larger randomized studies before firm conclusions can be drawn. 48 An intravesical instillation of photoactive drugs is necessary before the procedure, which seems to be the main disadvantage of PDD as compared with NBI. This may lead to the superiority of NBI over PDD in the management of the upper urinary tract.
Conclusions
The level of detection of BCa and the quality of TURBT remain unsatisfactory. To improve the quality of BCa management, there is a need to implement techniques improving both of these parameters. PDD and NBI appear to meet these conditions. Of the two, PDD has a stronger evidence base and has already been recommended for the detection of Cis by the European Association of Urology.
Footnotes
Author Disclosure Statement
No competing financial interests exist.