
Abstract
Introduction
D
Ever since the laser development by Maiman in 1960, laser radiation has been used in various animal tissues. 3 However, only after 1964, Stern and Sognnaes applied the ruby laser on dental tissue in vitro, with the intent of replacing drills. 4 Afterward, with the performance of in vivo experiments, it was observed that ruby laser application (35–55 J) on teeth caused thermal damage to the dental pulp, odontoblast cell destruction, and pulpal necrosis, even to teeth adjacent to the irradiated one. 5 The temperature increase has been the object of several in vitro and in vivo laser studies aiming at stating safe parameters to different laser wavelengths to avoid pulpal injury. 6 –8
Intra-chamber temperature increase due to visible light cure lamps has been described. Goodis et al. observed that the temperature rise was 3.3°C (6°F), therefore within safe levels for dental pulp. 7 Studies have indicated that high-level laser may increase dental temperature. Er:YAG laser irradiation in ablative parameters to caries removal and resin fillings laser did not exceed the safety threshold of 5.5°C (10°F) in the pulp chamber. 8,9 The potassium titanyl phosphate (KTP) laser study defined as optimum conditions for dentin irradiation 400 mW, pulse width 0.1 ms, repetition rate lower than 50 Hz, and 15 sec of irradiation, since these parameters do not cause pulpal damage, keeping intra-chamber temperature increase lower than 3°C. 10 Usual temperature increases in everyday situations, such as contact with warm food, or during drill cutting, are much higher than the ones caused by these lasers. 11 According to Miserendino et al., there is a lag of 10–20 sec between the incidence of laser radiation and pulpal temperature increase after CO2 laser, followed by a 60 sec lag of stabilization to environmental temperature. 1 For dentin hypersensitivity, Zhang et al. used CO2 laser refrigerated with water and did not observe pulp damage. 12 However, Park et al. suggested the use of air/water spray for a few seconds before Er:YAG laser application to reduce intra-chamber temperature rises even further. 13
Although low-level lasers are defined as those that have power outputs so low that they produce no important thermal effects on the irradiated tissues, 6,14,15 dental temperature increase near the threshold of pulpal safety is also observed with low-level lasers. Four different infrared gallium aluminum arsenide (GaAlAs) lasers applied onto the enamel surface study observed a 3.0°C pulpal chamber temperature increase, within safe limits for clinical use. 8
In his editorial, Brugnera highlights the importance of low-level laser treatment and states the biophotonics and life science interactions. 14 Red diode laser with a wavelength from 650 to 950 nm can penetrate biological tissue to a depth of 3 mm. 15 Laser therapy was effective in preventing and treating oral effects induced by radiotherapy and chemotherapy, thus improving the patient's quality of life. 16,17 The effects of red diode laser therapy applied in repeated doses in adults with a healthy periodontium treated by lingual orthodontic appliances were positive. 18
Medical, dental, and veterinary therapeutic lasers manufacturers have sought to increase power output; however, the appropriateness of higher outputs is not supported by studies demonstrating the effects of laser irradiation in the dental teeth. 6 The low-level laser benefit could be lost if a high-power output reaches thermal increase effect over pulpal safety threshold. 19,20
Laser therapy with 670 nm is a potential method for treating dentinal hypersensitivity. 21 There is a lack of information on thermal effects of InGaAlP laser (670 nm wavelength) at medium power settings, which are necessary for laser use in tissue biomodulation, healing, and dentin-desensitizing procedures. 13,18,19 It is important to determine safe irradiation parameters for clinical use of InGaAlP laser, since its low cost, small size, and portability features demonstrate great potential for deployment in the public health system.
The objective of this study was to evaluate the intra-chamber temperature increase in extracted human incisors, canines, premolars, and molars in vitro, using InGaAlP laser diode radiation at 670 nm wavelength, at different power levels.
Materials and Methods
The Research Ethics Committee approved the study. Twelve extracted human teeth kept in a 0.5% thymol solution were divided into four groups: incisors, canines, premolars, and molars, with three teeth in each group, representing the anterior and posterior teeth. These teeth had been extracted due to chronic periodontal illness. The specimens were transversely cut 3 mm from the cervical line by using a diamond drill (#1014; KG Sorensen, Sao Paulo, Brazil). The root canal was slightly widened with a #2 spherical drill (KG Sorensen, Sao Paulo, Brazil) to insert a thermocouple temperature probe. The specimens were stored in water, since hydration was considered of fundamental importance to maintain thermal conductivity properties.
A mounting device was used to hold the teeth during the experiments. 9 The teeth were glued to the acrylic device by using a Pritt-Multi-Tak-brand plaster (Henkel, Sao Paulo, Brazil).
A thermocouple probe was introduced into the pulp chamber, touching the inner wall across the point where laser radiation was to be applied. The hole was sealed with plaster. All specimens were X-rayed to verify proper positioning of the temperature probe, as shown in Fig. 1.
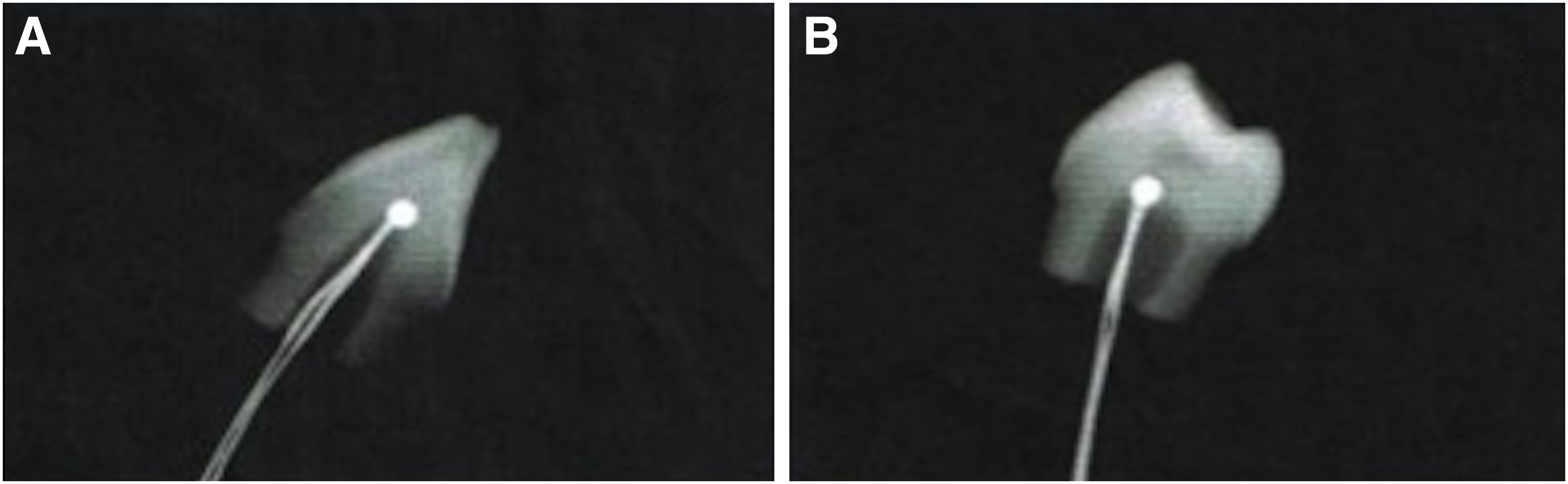
Representative X-ray images of appropriate positioning of the thermocouple temperature probes in anterior
An InGaAlP 670 nm laser diode, model MED-701 (Lasotronic, Platting, Germany), with a maximum output power of 340 mW was used. Laser radiation was applied at a right angle onto the external dental surface, at the point across from the thermocouple probe. Several power settings were used in the experiments: 100% (340 mW), 80% (272 mW), 60% (204 mW), 40% (136 mW), and 20% (65 mW) of the maximum power rating. Continuous wave irradiation was applied for 30 sec at five different power outputs: 340 mW (energy density 144.3 J/cm2), 272 mW (energy density 115.4 J/cm2), 204 mW (energy density 86.6 J/cm2), 136 mW (energy density 57.7 J/cm2), and 65 mW (energy density 28.8 J/cm2). The laser tip was kept ∼1 mm from (no contact) and perpendicular to the tooth surface. Laser setting was adjusted by using the calibrated power meter supplied with the equipment. All specimens were irradiated at each of those predefined power settings. The irradiation spot was determined by using digital radiographs with the thermocouple positioned cervical on the vestibular dental surface.
Temperature readings were taken with a fast-response K-type chrome-alumel thermocouple probe (ICEL, Manaus, Amazonas, Brazil) with 0.5 mm diameter. Thermocouple wires were connected to a digital thermometer that was calibrated according to IEC584 and National Bureau of Standards (NBS) standards for temperatures between 0°C and 50°C and a relative humidity below 80%.
Pulpal chamber initial temperature (Ti) was measured, and final temperature (Tf) was recorded immediately (0 sec) after irradiation. A third measurement was performed 3 min after laser irradiation.
The procedures of four groups of teeth were performed on the same day to avoid the effects of differences in climatic conditions. The measurements were repeated 24 h after removal and reinsertion of the probe in the pulp chamber. In each cycle, temperature was taken for each of the five power levels. Between the first and second cycle, all thermocouple probes were removed and reinserted into the pulp chamber to allow for variations of experimental conditions.
Statistical analysis
The temperature gradients (ΔT) were calculated (ΔT = Tf–Ti) for each group. The medium ΔT (°C) and standard deviation were calculated for each group. Data of temperature alteration (ΔT) were statistically analyzed by two-way analysis of variance (ANOVA) at the 95% confidence level and compared by Tukey post hoc test (α = 0.05).
Results
Data consisted of ΔT values obtained inside the pulp chamber after 30 sec irradiation of the external surface, as a function of laser settings (68–340 mW) in the four dental groups: incisors, canines, premolars, and molars. It has been observed that 3 min after turning off the laser, diode temperature readings returned to environmental values in all cases. Figure 2 shows the mean temperature increase values obtained for each experimental group on time 0 sec.
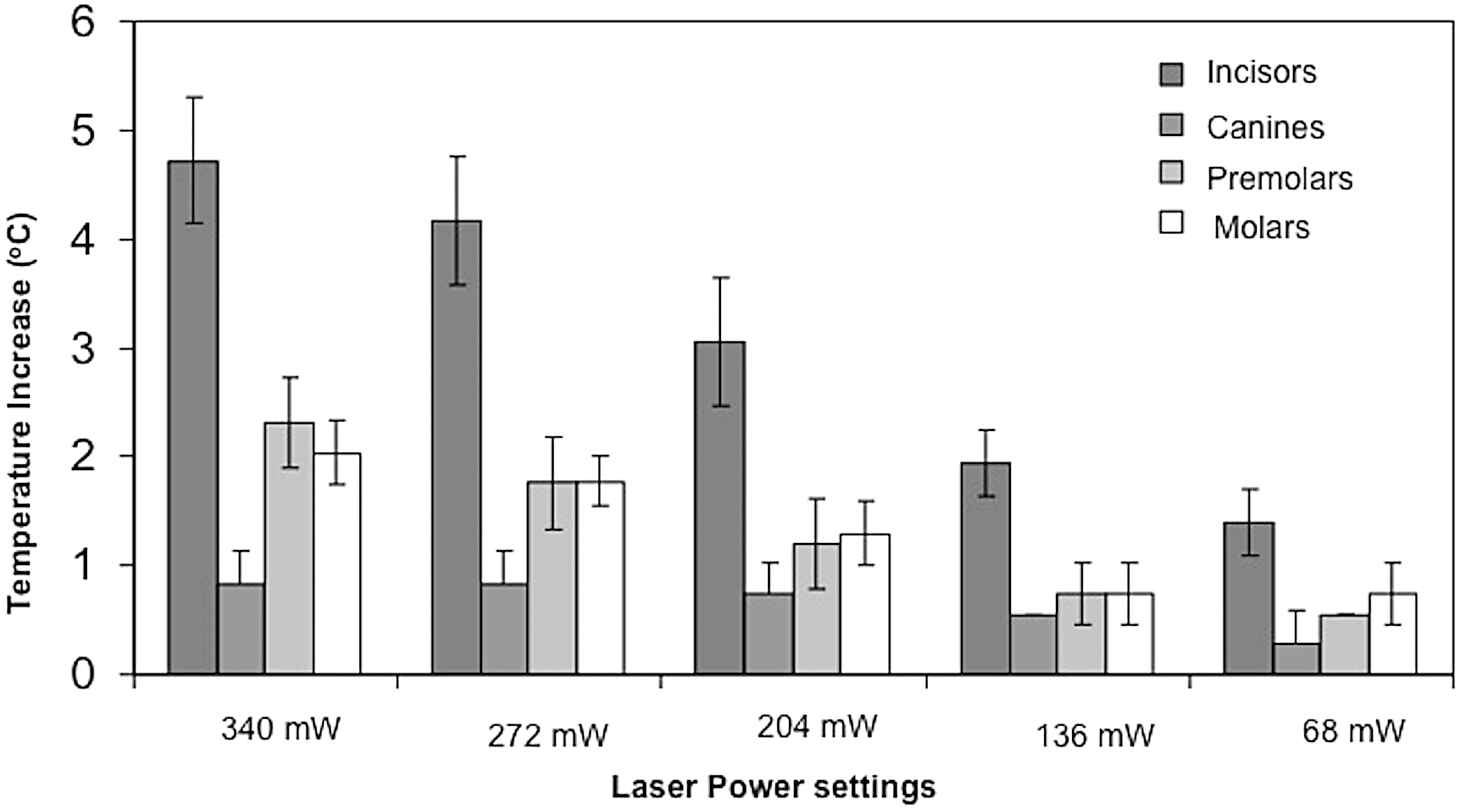
Mean temperature increase for the experimental groups.
Data showed temperature increase proportional to laser settings. Incisors had higher elevation, reaching 4.7°C mean temperature increase and 5.5°C as the highest value with a maximum power of 340 mW. Canines, premolars, and molars showed significantly lower increases, reaching mean values of 2.3°C, 2.0°C, and 0.8°C, and peaking at 2.8°C, 2.2°C, and 1.1°C, respectively.
ANOVA showed statistically significant differences to interaction of factors (p = 0.0001). Table 1 shows the ΔT (°C) obtained in each evaluated group and the results of Tukey's test.
Means followed by different uppercase letters in the column and lowercase letters in the row indicate statistical differences (p > 0.05).
n, sample number; SD, standard deviation.
The ΔT (°C) obtained was influenced by the teeth group and power output. The highest ΔT values obtained were observed to incisors (340, 280, and 210 mW), canines presented the lowest ΔT, and canines were not influenced by power output.
Discussion
Stimulatory and regenerative effects at the molecular level can be reached by application of photon energy to injured tissue, and this therapy is called biostimulation. 22 One biostimulatory method is performed by using sub-500 mW ranges of low-level laser. 22 Low-level laser irradiation with a semiconductor laser (670 nm) is a successful physical adjuvant method of treatment, which, associated with traditional periodontal therapy, leads to better and longer-lasting therapeutic results. 23 The InGaAlP laser diode radiation at 670 nm was selected for the present study based on the limited literature data regarding intra-chamber temperature change caused by tooth irradiation at this wavelength with medium power values, despite its potentially effective clinical use in trophic therapies (biomodulation) and desensitization due to its adjustable power level and wavelength within the therapeutic window. 13,16 –18
Therefore, it is important to establish safe parameters for its clinical use. In our literature search, the thermistors and thermocouples were used to measure intra-chamber temperature in several studies. 8,9,12 The thermocouple associated with a digital thermometer achieves precision, accuracy, and stability, thus making it an accurate method to study thermal effects on the pulpal chamber. Along with irradiation on dentin to hypersensitivity treatment, Zhang et al. also observed the absence of harmful effects on the pulpal chamber when using CO2 laser with water cooling. 12 The application of Er:YAG and diode lasers did not induce high pulpal temperatures after scaling and root planing with hand instruments. Root surface irregularities were more pronounced after irradiation with an Er:YAG laser than with a diode laser. 24 Intrapulpal thermal changes that occurred during the treatment of the root surfaces with a laser system emitting Er,Cr:YSGG 2,780- and 940-nm diode laser irradiation in an alternating sequence have been reported as lower than the critical value of 5.6°C. 25
The immediate and late therapeutic effects of the 660 nm red diode presented positive effects to tooth hypersensitivity. 21 The dentin hypersensitivy treatment using the red laser in low power (sub 500 mW) was a photobiomodulation therapy aiming at both or stimulation of the odontoblast activity for dentin formation or inhibitory activity for pain control. 21 Low-level laser therapies are considered biomodulatory therapies that do not generate heat. 6
It has been related that multiple sessions with 670 nm laser as an adjunctive treatment of inflamed periodontal tissue presented a faster and greater tendency to reduce proinflammatory mediators 26 and led, to some extent, to a slight orthodontical improvement. 27
The present study results indicated that temperature increases proportional to laser power settings, and the incisors showed a higher temperature increase: 4.2°C was the mean temperature increase, and 5.5°C was the highest measured value. Such temperature rises were obtained by irradiating the specimens with maximum laser settings (340 mW) for 30 sec, and they are close to the threshold level for causing irreversible pulp injury, according to Zach and Cohen. 2 Incisors have thinner enamel and dentine walls than the other teeth groups, so heat conduction into the pulpal chamber tends to be higher than others. These values of temperature increase emphasize the concerns on clinical use of such high-power levels at this wavelength, and clinicians must be cautious when treating incisors. This way, each operator must be aware of the parameters for appropriate laser setting. 5
The teeth samples used in this study represent all categories of human teeth, with their morphological and functional differences. The intrapulpal chamber temperature increases observed here come from the heat generated at the enamel surface and conducted into the pulp chamber. Canines showed lower temperature rises than all other teeth types at all power levels. This can be explained by their thicker enamel and dentine walls, which interferes directly with heat conduction into the pulpal chamber, and also due to the larger tissue volume, which distributes the heat and helps decrease the temperature peak.
Since the thermal increase observed in this study was with a 100% power output (340 mW, continuous wave for 30 sec), especially in certain groups of teeth such as incisors, special attention should be paid toward selecting safe power parameters. Based on the results of the present study, the authors want to alert those using photobiomodulation therapy that depending on the type of teeth and the power output applied in the therapy some temperature increase can be observed.
Conclusions
The intrapulpal chamber temperature increase was influenced by the teeth group and power output. The highest temperature values were observed to incisors. Canines presented the lowest values and were not influenced by power output.
Footnotes
Author Disclosure Statement
The authors have no interest in any of the companies or products mentioned in this article.
Author Notation: Even short irradiation periods and low power outputs are likely to raise incisor pulp temperature to dangerous levels in thin dentin regions.
Kreisler M, Al-Haj H, D’Hoedt B. Intrapulpal temperature changes during root surface irradiation with an 809-nm GaAlAs laser. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002;93:730–735.