
Abstract
Introduction
I
Several studies on the prevalence of WSLs have revealed a high prevalence varying from 50% to 97%. 1,8,9 In addition, orthodontic treatments usually take a long time and are mostly performed in young patients, which make it more difficult to control the development of WSLs. 1,5 –10 Thus, more efficient and long-lasting therapeutic approaches for preventing WSLs around the brackets have been proposed, including enamel irradiation with Nd:YAG laser, 10 argon laser, 11,12 and CO2 laser. 10,13 –15 These lasers are promising in the prevention of dental caries due to their ability to alter the morphology and the chemical composition of the tooth structure. 14 –24 In fact, in one of our previous studies, we found a short-term preventive effect of dental demineralization around brackets after CO2 laser (10.6 μm wavelength) irradiation. The outcomes were similar to fluoride treatment. 10
Zuerlein et al. 25 have already shown that the CO2 (10.6 μm) wavelength laser has deep penetration and affects a thick enamel layer. This can cause long-term preventive demineralization. The hypothesis of this study is that the enamel demineralization preventive effect observed after CO2 laser irradiation could be extended after successive acid challenge cycles due to permanent enamel structural alterations. To test this hypothesis, a second pH-cycling challenge was done on the top of the same enamel surfaces that were already submitted to a pH-cycling challenge.
Materials and Methods
Sample preparation
Sixty-five human enamel samples were retrieved from a previous study 10 after approval from the School of Dentistry Research Ethics Committee of the Ibirapuera University (CEP No. 87613).
The 65 enamel fragments were bonded to brackets and were submitted to five different superficial treatments according to the following experimental groups: (G1): topical application of 1.23% acidulated fluoride phosphate gel (AFP—control); (G2): Nd:YAG laser irradiation (0.6 W, 84.9 J/cm2, 10 Hz, 110 μs, contact mode); (G3): Nd:YAG laser irradiation associated with AFP; (G4): CO2 laser irradiation (0.5 W, 28.6 J/cm2, 50 Hz, 5 μs, and 10 mm focal distance); and (G5) CO2 laser irradiation associated with AFP. Afterward, all specimens were submitted to the first pH-cycling challenge as proposed by Featherstone et al., 26 with the solutions proposed by Argenta et al. 27 The specimens were immersed in a demineralization solution (2.0 mmol/L of calcium, 2.0 mmol/L of phosphate, 0.03 ppm of fluoride, and 75 mmol/L of acetate in pH 4.5) for 6 h followed by a remineralization solution (1.5 mmol/L of calcium, 0.9 mmol/L of phosphate, 150 mmol/L of potassium chloride, 0.05 ppm of fluoride, and 20 mmol/L of Tris buffer at pH 7.0) for 18 h at 37°C. The entire procedure was repeated daily for 14 days, and the solutions were changed on the fifth day of pH-cycling. Quantitative light-induced fluorescence (QLF) was used to assess enamel mineral loss. 10 These samples were then stored in water for 1 year and submitted to a second acid challenge and QLF.
Enamel surface analysis after second pH-cycling challenge
Demineralization was evaluated using quantitative light-induced fluorescence (QLF—Inspektor Research Systems, Amsterdam, Netherlands). The QLF images were taken before and after the second pH-cycling. The images were analyzed using commercial software (QLF 2.0.36; Inspektor Research System BV). The percentage of fluorescence change was calculated by subtracting the percentage of fluorescence taken at the end of the second pH-cycling from the percentage of fluorescence before this pH-cycling (baseline values).
After the QLF measurements, one specimen from each group was prepared for scanning electron microscopy (SEM) morphological examination. Scanning electron micrographs obtained with a Philips XL30 (Eindhoven, The Netherlands) operating at 20 kV were taken at the same working distance, using a same magnification (800 × ).
The results of the mineral losses were compared via one-way analysis of variance complemented by the Tukey's test. The level of significance was set at 5% (p ≤ 0.05).
Results
Figure 1 illustrates the results of enamel mineral loss in all experimental groups after the second pH-cycling challenge. The mineral losses observed varied from 28.21% ± 2.19% to 50.87% ± 4.57%. The groups irradiated with CO2 laser were associated (G5) or not (G4) with fluoride. They showed significantly lower mineral loss percentages than those observed in all other groups (p = 0.0002). The groups submitted to irradiation with the Nd:YAG laser (G2 and G3) showed mineral losses similar to that of the fluoride group (G1).
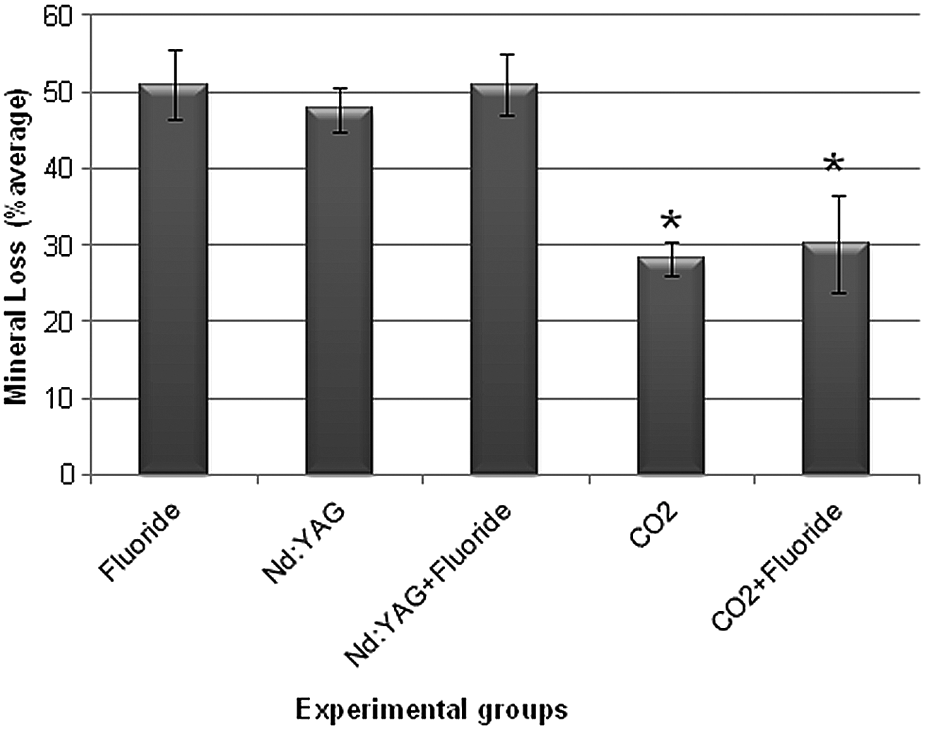
Graphic representation of the results of mineral losses in all experimental groups after the second pH-cycling challenge. Bars indicate the standard deviation. *Significantly different from all other groups (p < 0.05).
SEM analysis
After the second pH-cycling, the specimens from different groups had differences in the overall superficial enamel morphology (Fig. 2). The positive group treated only with fluoride (G1) had an enamel surface with exposed enamel prisms (Fig. 2A). These prisms had rounded tips and seemed to be compact with a homogeneous distribution.
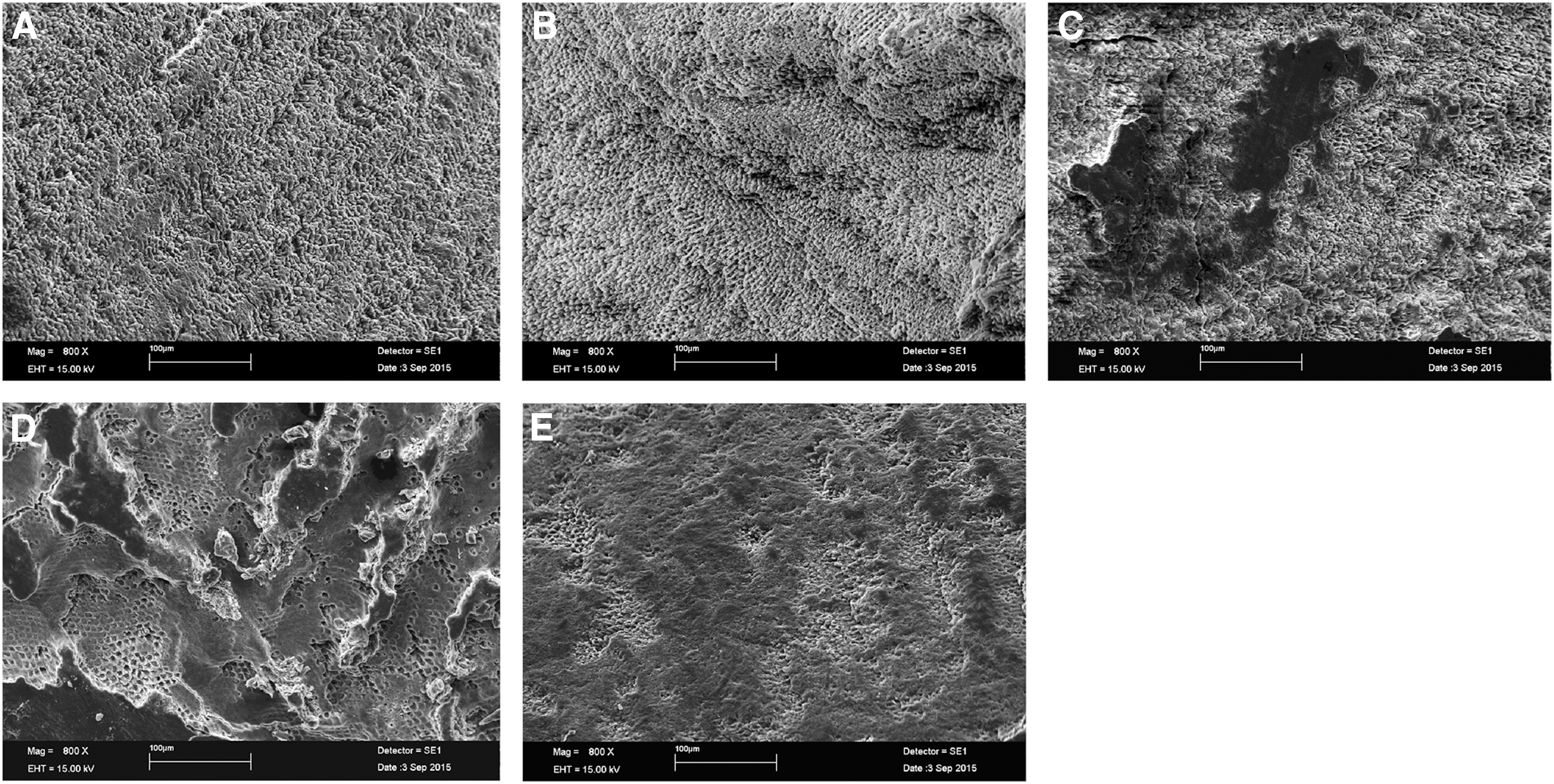
Representative scanning electron micrographs of the enamel surfaces after second pH-cycling.
The groups treated with the Nd:YAG laser were associated (G3, Fig. 2C) or not with fluoride (G2, Fig. 2B). They were also devoid of the aprismatic enamel surface. In the G2, the surface was irregular, and the enamel prism centers were partially removed resulting in sharp ending prisms. In G3, there was preferential removal of prism core material, and the prism peripheries were relatively intact.
The groups treated with CO2 laser irradiation (G4 and G5) were mostly covered by structures, interpreted as a melted layer that resembled the aprismatic enamel surface (Fig. 2D and E, respectively). In G4, this melted layer presented different thicknesses and in some areas it was possible to observe the underneath enamel prisms in a honeycomb arrangement. In G5, the thickness of the melted layer was homogeneous and there was a honeycomb arrangement of the enamel prisms.
Discussion
The prevention and control of the WSLs around brackets are a problem for orthodontists and patients. 1 –3 The most common WSL preventive therapy is the use of fluoride. However, the first randomized, triple-blind, placebo-controlled study with patients undergoing orthodontic treatment, which tested the continued use of fluoride mouthwash, revealed that although the fluoride group is more effective than the placebo group, 36% of patients in this group still showed some WSLs. 5 This justifies the search for more effective preventive approaches.
High-power laser irradiation is an alternative method to prevent enamel demineralization, and our research group has shown in a previous study that CO2 laser irradiation (10.6 μm) is a preventive therapy equivalent to fluoride therapy after a first pH-cycling challenge analysis. The hypothesis of this study is that the enamel demineralization preventive effect observed after CO2 laser irradiation could be maintained in response to a second pH-cycling challenge due to permanent and deep enamel structural alterations. In fact, confirming our hypothesis, the enamel irradiated with CO2 laser had significantly lower mineral losses than those observed in all other groups, including those submitted to fluoride therapy after the second pH-cycling challenge analysis.
The high-power lasers have been studied as an alternative for preventing dental caries because they can modify the chemical and morphological enamel structure. This reduces the teeth acid reactivity without compromising pulp vitality. 15 The major advantage of these therapies is that laser applications do not depend on the patient involvement versus fluorinated mouthwashes nor does it need frequent reapplication. 10
As expected, if the fluoride was applied before the first pH-cycling challenge, then there was no need for a second application. The samples in this group had the highest mineral loss. This does not mean that reapplication of fluoride in those specimens would result in a smaller mineral loss. However, the aim of this study was to verify the response of irradiated enamel to a second pH-cycling challenge that avoids fluoride reapplication.
The Nd:YAG laser irradiation could prevent the development of WSLs after the first pH-cycling challenge 10 when associated with fluoride. Thus, it was expected that after the second pH-cycling challenge analysis, the Nd:YAG laser-irradiated samples resulted in mineral losses similar to those in the fluoride group. Thus, confirming the results of the previous study, the Nd:YAG laser irradiation is not a choice for preventing WSLs around brackets. The parameters for the Nd:YAG laser irradiation used in this study were similar to Boari et al., 28 which were considered safe for using in caries prevention.
The lowest mineral losses in the present study were observed in the samples treated with the CO2 laser at 10.6 μm. This loss was similar in groups where the irradiation was or not associated with fluoride. This result was the same as previously observed after the first pH-cycling challenge analysis of these samples 10 and also in other studies. 29 –31 The CO2 laser irradiation parameters applied here were previously presented by Hossain et al. in a similar study that confirmed acquired acid resistance of enamel and dentin when they used CO2 laser irradiation with sodium fluoride solution. 32
Thus, the preventive effects in these groups are exclusively due to the changes in enamel structure elicited by the CO2 laser irradiation. In fact, the SEM images showed striking superficial morphological changes after the second pH-cycling in the function of different treatments. Only in the enamel specimens irradiated with the CO2 laser, there was preservation of the honeycomb-like aspects of the prisms protected by a layer of melted enamel. This indicates that CO2 laser at 10.6 μm can alter enamel even below the superficial layer. After the first pH-cycling, the resulting exposed layers kept the demineralization resistance and showed that preventive effects of CO2 at 10.6 μm laser irradiation could last longer because these deep layers were also altered.
The literature offers different explanations for the greater enamel acid resistance after CO2 laser irradiation, including the morphology of the irradiated enamel acts as a mechanical barrier to the acid challenge, 29,33 a decrease in the permeability of the enamel either by sealing the irregularities and pores of the enamel 34 or by changes in the organic components of this tissue, 35 enamel chemical changes, 29,36 or enamel physical changes represented by diminution in the crystal size due to loss of water and CO2 37 and, finally, due to the microhardness characteristics of the irradiated enamel. 38
Despite all explanations presented above, the association of the morphological aspects of the irradiated enamel surfaces with the smallest mineral losses of the samples irradiated with a CO2 laser observed in the present study is evidence of the effectiveness of such irradiation in preventing mineral loss in deep layers of enamel. Concurring with these results, in a clinical trial, although using a CO2 laser with different characteristics, Rechmann et al. 39 showed that CO2 laser inhibited demineralization of human tooth enamel. Thus, further in situ and then in vivo studies must be done to confirm our results using the 10.6 μm CO2 laser. These studies should also verify the quality of the shear bond strength of braces adhesion to enamel irradiated by CO2 10.6 μm laser.
Although this study was only done in vitro, the results are encouraging and offer to orthodontists a new tool against WSLs around the brackets. These professionals cannot always count on the collaboration of their patients especially those requiring successive office visits.
Conclusions
CO2 laser (10.6 μm) irradiation with the parameters of the study prevented enamel demineralization around brackets in deeper layers of enamel. While further clinical trials are needed to confirm the long-lasting effects, this wavelength is promising in the prevention of WSLs.
Footnotes
Acknowledgments
The authors thank the assistance rendered by the Department of Restorative Dentistry, School of Dentistry (FOUSP) and Special laboratory on Laser dentistry (LELO-FOUSP) for the use of their research facilities.
Author Disclosure Statement
No competing financial interests exist.