
Abstract
Introduction
H
EHs predominantly occur in middle-aged and elderly women; few cases have been reported in children. 3,4 The lesions are small thin-walled cysts, ranging from 1 to 6 mm in diameter. 5 They are predominantly located in the periorbital and malar regions.
The apocrine variant (AH) arises from proliferation of the apocrine glands; lesions are usually solitary, with a diameter of 3–15 mm. 2 Apocrine lesions are also found mostly on the head and neck, especially along the eyelid margin near the inner canthus. 2
Differential diagnosis of solitary EH is chiefly versus apocrine HCs, cysts, and pigmented basal cell carcinoma.
At present, HC usually result from dilation of the cystic excretory eccrine glands, due to retention of sweat, in conjunction with dilation or blockage of the sweat duct. Under microscopic observation, EH appear as unilocular cysts that usually comprise a single cystic cavity, delimited by one or two layers of cuboidal cells. 5
The etiology of EH remains unknown. One possible cause might be occlusion of the intradermal portion of the eccrine duct. Tokura et al. have suggested that solitary EH derive from the secretory coil, whereas multiple EH derive from the sweat duct. 6 Murayama et al. have suggested that EH is a hamartoma-like disorder that becomes more pronounced as a result of retaining sweat. 7
EHs may be associated with syndromes such as the Gorling Goltz syndrome, and they are usually exacerbated by high temperatures, disappearing in cold climates. 8 In the authors' view, the latter hypothesis might explain the atypical presentation in this case.
The case described is an atypical labial commissure presentation that was treated with a 980 nm diode laser. The 980 nm diode laser is a semiconductor device emitting infrared radiation, with good affinity for oxidized hemoglobin and melanin. It can be used in continuous or interrupted wave modes, through optical fibers of different diameters. The immunophenotype is characterized, and differential diagnosis is discussed.
Case Report
A 36-year-old man was referred to the Department of Oral Pathology, University of Genoa, in January 2015, for evaluation of a nodular lesion on the labial area adjacent to the commissure (Fig. 1), which had been present for 1 year and that caused psychological and aesthetic problems.

Left lower lip showing a nodular irregularly shaped lesion 7 × 5 mm in size.
The lesion appeared pink in color and translucent, with a soft-elastic consistency. It was 7 × 5 mm in size. There was no history of surgical or pharmacological treatment, with the exception of Gentalyn βgel applications (MSD Italy S.r.l.). In agreement with the patient, the lesion was removed surgically.
Surgery
Under local anesthesia with mepivacaine (Mepimynol, mepivacaine chloridrate 30 mg/mL; Curaden Healthcare, Saronno, Italy), a longitudinal incision was performed in direct contact with a hot tip by using a 980 nm diode laser (DM 980; DMT Lissone, Italy) in continuous wave mode, with a 320 μm fiber at 1.8–2.0 W of power (Fig. 2).

The lesion was excised with a 980 nm diode laser.
On exposure, the lesion appeared to adhere closely to the surrounding connective tissues. Complete hemostasis was easily achieved without the use of sutures, and the patient was shortly discharged (Fig. 3).

Appearance of the labial commissure immediately after excision by diode laser.
Gentalyn β gel applications (MSD Italy S.r.l.) twice daily for 7 days were prescribed, together with a soft, cold diet for 2–3 days.
Histology
Histological examination showed a multilocular cystic cavity lined with a single, or sometimes double, cuboidal-flat epithelium, filled with red blood cells, which covered the inner luminal surface without decapitation (Fig. 4). Immunohistochemistry revealed a positive immunophenotype for S-100 (Fig. 5) and a negative immunophenotype for cytokeratin 5/6. One month later, clinical follow-up showed complete tissue healing. The case was followed up at 3 months and after 1 year (Fig. 6).
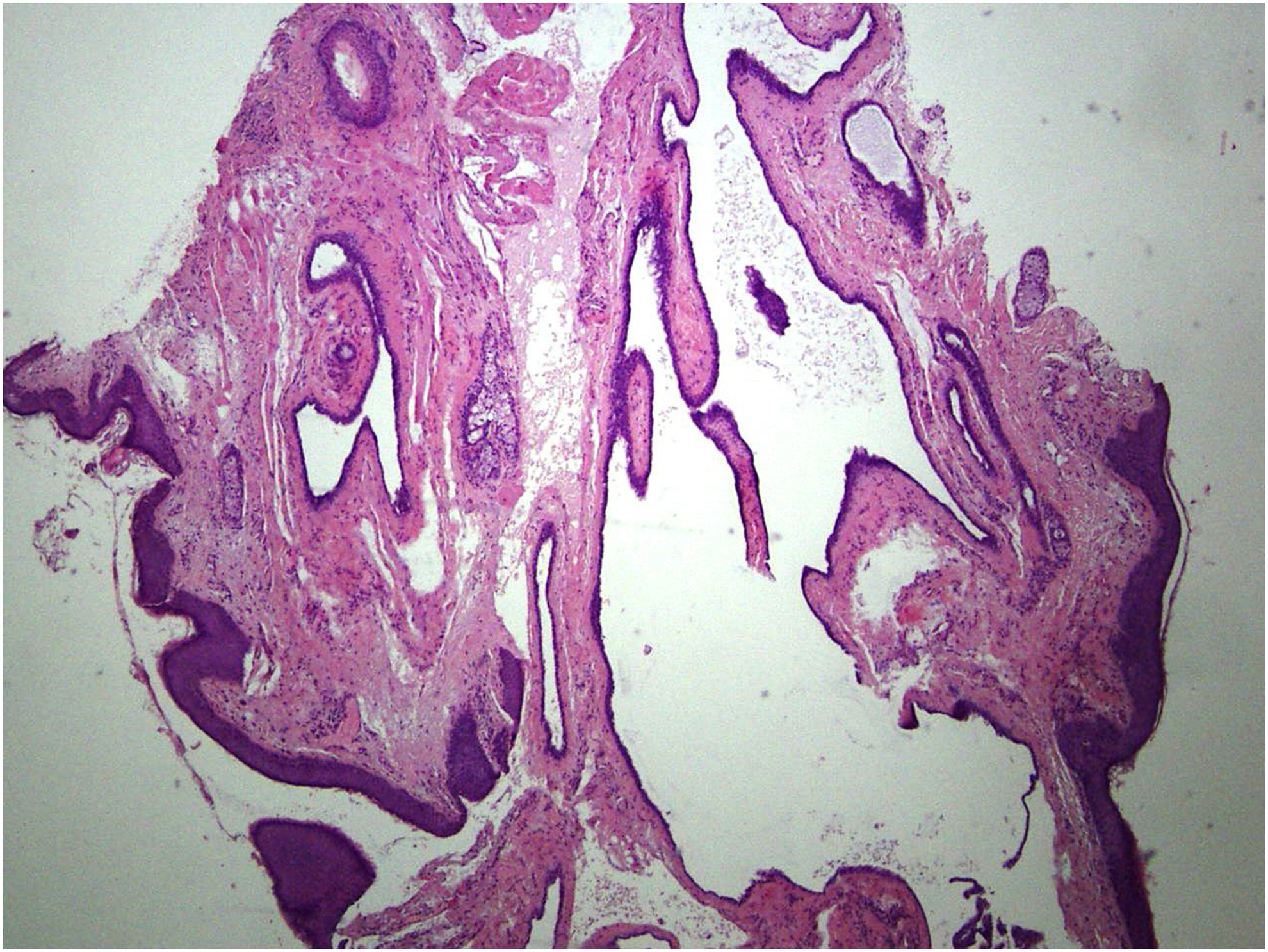
Microphotograph of hydrocystoma showing a cystic cavity lined with a single cuboidal-flat epithelium (EE original magnification 4 × ).
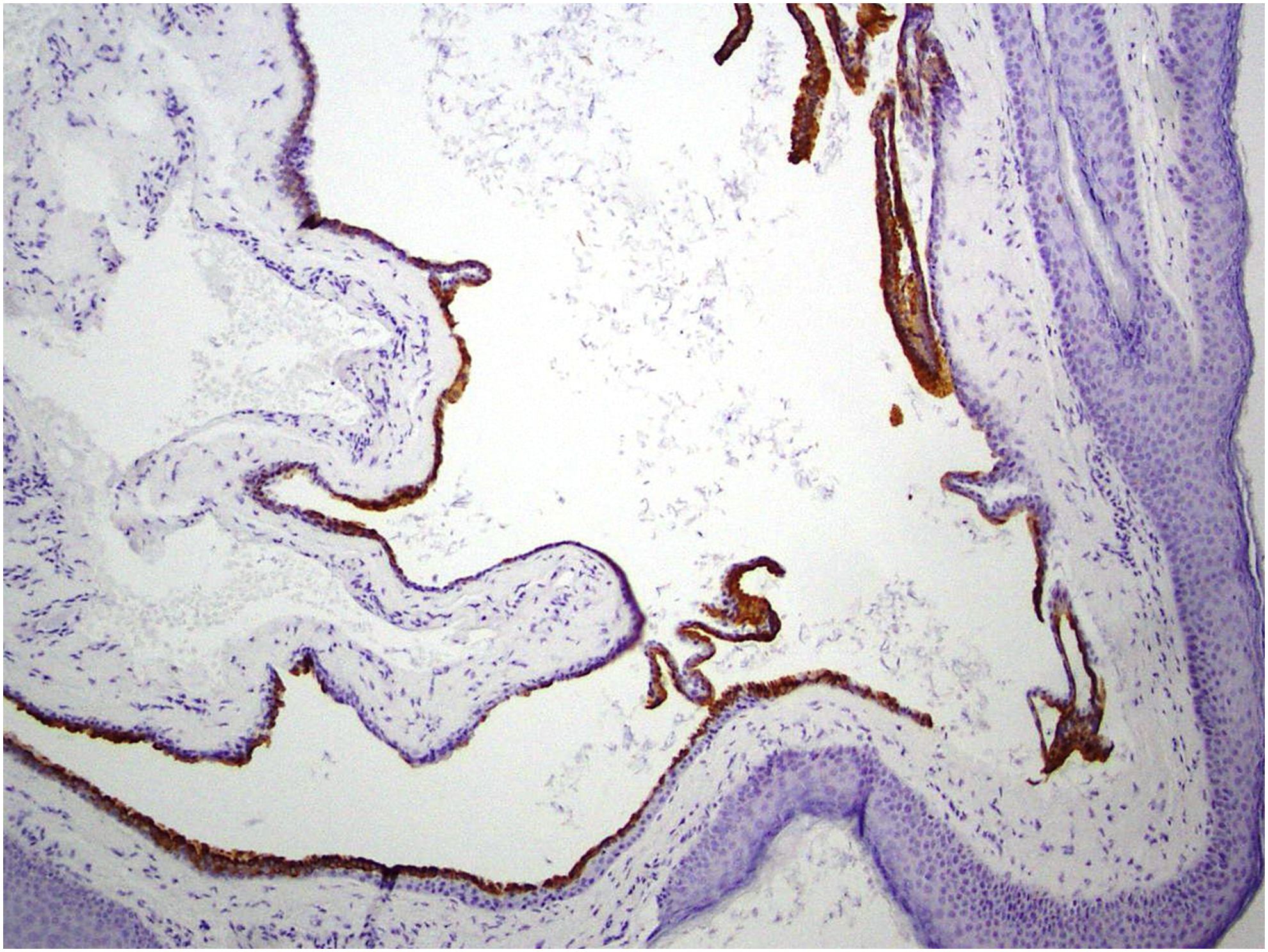
Immunohistochemistry revealed a positive immunophenotype for S100 (original magnification 10 × ).

After 1 year of follow-up.
Discussion
HCs are also known as cystadenomas, sudoriferous cysts, Moll's gland cysts, or adenomas of the apocrine or eccrine sweat glands. Apocrine-HC (apocrine cystadenoma) was first described by Mehregan in 1964 as a benign skin cystic lesion derived from the secretory portion of the apocrine gland. 9 This lesion arises through proliferation of the apocrine glands and is usually solitary, with a diameter of 3–15 mm. 7,8 Eccrine HCs, first described by Robinson, 1 present as small, tense, thin-walled cysts that are 1–6 mm in diameter, and they can occur as single or multiple lesions. 7,8 Both apocrine and eccrine HCs are prevalent in adults between the ages of 30 and 75, and the lesions are generally distributed in similar sites on the body. 10 –12 HCs occur very rarely on the lips. 1 Clinically, solitary lesions are more likely to be apocrine-HCs than eccrine-HCs. Multiple apocrine-HCs occur in Goltz-Gorlin syndrome and Schopf-Schulz-Passarge syndrome. 8 Morphologically, apocrine-HCs have a double lining of epithelium (inner layer, tall columnar or cuboidal cells) with decapitation secretion, and an outer layer consisting of myoepithelial cells; whereas eccrine-HCs are lined with flat epithelium without myoepithelial cells. 3,12 Immunohistochemically, apocrine-HCs are positive for human milk fat globules, GCDFP-15, CK7, and CK18 in the inner layer of the epithelium, and also positive for α-SMA in the outer myoepithelial cells; whereas eccrine-HCs are negative for all these antibodies. 10 Therefore, the most compatible pathological diagnosis in the present case was eccrine-HC. The histomorphological aspects are very important for differential diagnosis.
Differential diagnosis includes cysts and tumors such as cystadenoma, cystadenocarcinoma, and sclerosing polycystic adenosis. Clinically, sweat gland lesions are distinguishable by swelling of the skin. Immunohistochemically, solitary EHs typically show CK7 positivity in luminal cells, and S100 positivity in abluminal cells, whereas multiple EHs and AHs do not. 11,13 Despite this difference, it is not always simple to differentiate EHs from AHs, 10 not least because they both affect the same age groups. EH must also be distinguished from the cystic variant of basal cell carcinoma, which is very similar in appearance but tends to ulcerate and, consequently, to bleed.
Although a solitary EH can easily be treated through surgical excision, treatment of multiple EHs is difficult because of their number and cosmetic location. 14 Until recently, there were no effective treatments for EH, but a number of different therapeutic options are now available, including medical and surgical approaches. In the case of solitary type, total surgical extirpation is the most viable option, but the multiple variety offers greater challenges due to the high risk of recurrence. Multiple lesions can be treated with topical scopolamine, topical atropine, botulinum toxin, or surgically, using a 980 nm diode laser.
The diode laser has significant beneficial properties: ablation of soft tissues, hemostatic and bactericidal effects. It is an excellent surgical laser for use in dentistry, because it can cut all oral vascularized soft tissues, and it also has the advantages of providing excellent hemostasis, high precision tissue destruction, no suture requirement, wound sterilization, and minimal postoperative pain and edema. 15,16 Considering these advantages, the diode laser was chosen as an alternative to the traditional scalpel to remove the EH in the present case, especially due to the location of the lesion. No pain medication was required after surgery, and wound healing was both excellent and rapid. 15 Obviously, to prevent worsening of symptoms, it is important that patients avoid hot temperatures and humid conditions during the healing period.
Conclusions and Summary
This case shows that HCs should be taken into consideration in the differential diagnosis of patients presenting with multiple adnexal tumors. Despite an atypical distribution, the pink-gray translucent appearance of these lesions is helpful in making the correct diagnosis.
Minimal postoperative pain and rapid wound healing make laser-assisted surgery a tolerable procedure when oral neoformations must be removed.
Informed consent was obtained from the patient included in this study.
Footnotes
Author Disclosure Statement
No competing financial interests exist.