
Abstract
Introduction
P
Despite the large number of studies available, there is still lack of consensus to date regarding the protocols of treatment. All the authors agree on two fundamental aspects: control of the inflammation and degranulation of diseased tissue. However there is no general agreement to date about the devices and the instruments to be used to obtain these objectives. Most studies available involve laser therapy, with its use increasing in recent years. Studies can be divided into pre-clinical (in vitro and animal models) and clinical sectors. Generally the in vitro studies on the use of laser on titanium surfaces are made on disks or implants using mainly diode or Er:YAG and Nd:YAG lasers and, less frequently, CO2 lasers, and they all report reasonable results in terms of decontamination capacity. 5 –14 No major differences are reported when different types of lasers are compared. All the studies on animal models give excellent results following the use of the laser, be it Diode, Er:YAG, or CO2. The most important contribution from these study types is the histological information on new bone to implant bone formation (BIC). This is an actual reosseointegration, which seems to reach levels markedly higher after the use of the laser. 15 –24
Clinical studies and case series are subject to extreme variability, and this applies even more when it comes to laser studies. Data vary with different types of lasers used or when using the same type of lasers, different settings are often used. For example, in some studies, the laser is used as the only device, while in other studies the laser is used in conjunction with other therapeutic modalities.
In general, the outcomes considered in clinical trials are parameters like probing depth (PD), bleeding on probing (BOP), clinical attachment level (CAL), and radiographic bone fill. Microbiological samples are analyzed less frequently. In principle, almost all clinical trials in which the use of laser is evaluated in comparison to other devices or agents, the results vary between slightly superior to no differences in terms of clinical and radiographic parameters. In contrast, in the few studies analyzing microbiological parameters, the results are better, showing lower pathogenic bacterial rates detected in the sites treated with laser. 25 –40
Many of the above studies have explored the possible advantages using an adjunct photosensitive dye combined with laser irradiation, namely photodynamic therapy (PDT). 5,14,17,19,20,23,25,26,36,37
The photosensitization, also known as PDT, is based on the application of photosensitive dyes activated by light, with a specific wavelength, to destroy bacteria. It usually includes three basic elements: low-level diode laser, nontoxic photosensitizer, and oxygen. When activated by light, the photosensitizer produces a reactive singlet oxygen, which in turn, causes bacterial cell death. 41 –44 Several dyes have been used as photosensitizers, such as toluidine blue, methylene blue, and porphyrin and its derivatives. 45 –48 These dyes can be excited by light sources that fall in the range of visible-red spectrum (630–670), with penetration capacity in biological tissue of ∼8 mm. In contrast, near-infrared wavelengths (800–1100 nm) have a penetration of up to 10 mm or greater. 49
While it is commonly accepted that peri-implant infections are mostly associated with periodontal species such as Porphyromonas gingivalis, Tannerella forsythia, Prevotella intermedia, and Treponema denticola, it is not the specific aim of this study to assess the efficacy of the diode laser against these bacteria, which has already been demonstrated in other studies. Moreover, the colonization of the surface by these late phase bacteria is possible only due to early colonizers (Streptococcus sanguis ex.), which are the initiators of the biofilm on the implant surface. 5,11,12 Biofilm disruption can be accomplished with the aid of the mechanical devices. However, decontamination of the bacterial populations more closely adherent to the implant surface (namely the early colonizers) is served well by the use of laser therapy. The laser's nonmechanical action has the capacity to eliminate the bacteria from those surface areas inaccessible by classic instrumentation.
Based on this assumption we justify the sole use of an early colonizer in our study.
The aim of this ex vivo study is to evaluate the efficacy of diode laser, used at two different wavelengths, with or without the aid of indocyanine green (ICG) photosensitization, in reducing the colonization of Streptococcus sanguinis on smooth dental implant surfaces.
In addition, since an increase of >10°C above body temperature is considered to cause injury in bone and to compromise regeneration, the variation of temperature on the implants during irradiation with the two diode lasers under conditions that closely replicate those of the human body was assessed. 50,51
The null hypothesis was defined as: there is no difference in surface decontamination potential after use of different wavelengths of diode laser with and without photosensitizer dye.
Materials and Methods
Manipulation
Model: Swine ribs were used in this ex vivo study and cut into blocks of about 1 cm for placing implants. Nobelpharma MKIII machined implants (Brånemark; Nobelpharma AB, Gothenburg, Sweden), with a diameter of 4 mm and different lengths, were glow discharged to preserve surface characteristics from corrosion and then placed in the bone blocks according to manufacturer's instructions. 52 Angular bony defects were created before implant placement using a pilot drill, with the dimensions of 2 mm wide and 2 mm deep, adjacent to the implant site (Fig. 1). The defect exposed the side of the implant to allow bacterial adhesion to the surface. The bone blocks with the implants were then sterilized in steam autoclave. Three bony specimens were separately placed in tryptic soy broth and incubated for 48 h to assess any bacterial growth. The peri-implant defects were all inoculated with 10 μL tryptic soy broth transporting S. sanguinis. The samples were then placed in an incubator with the atmosphere of 5% CO2 at 37°C for 24 h to allow for bacterial colonization. The bone blocks containing the implants were kept in sterile screw cap glasses.
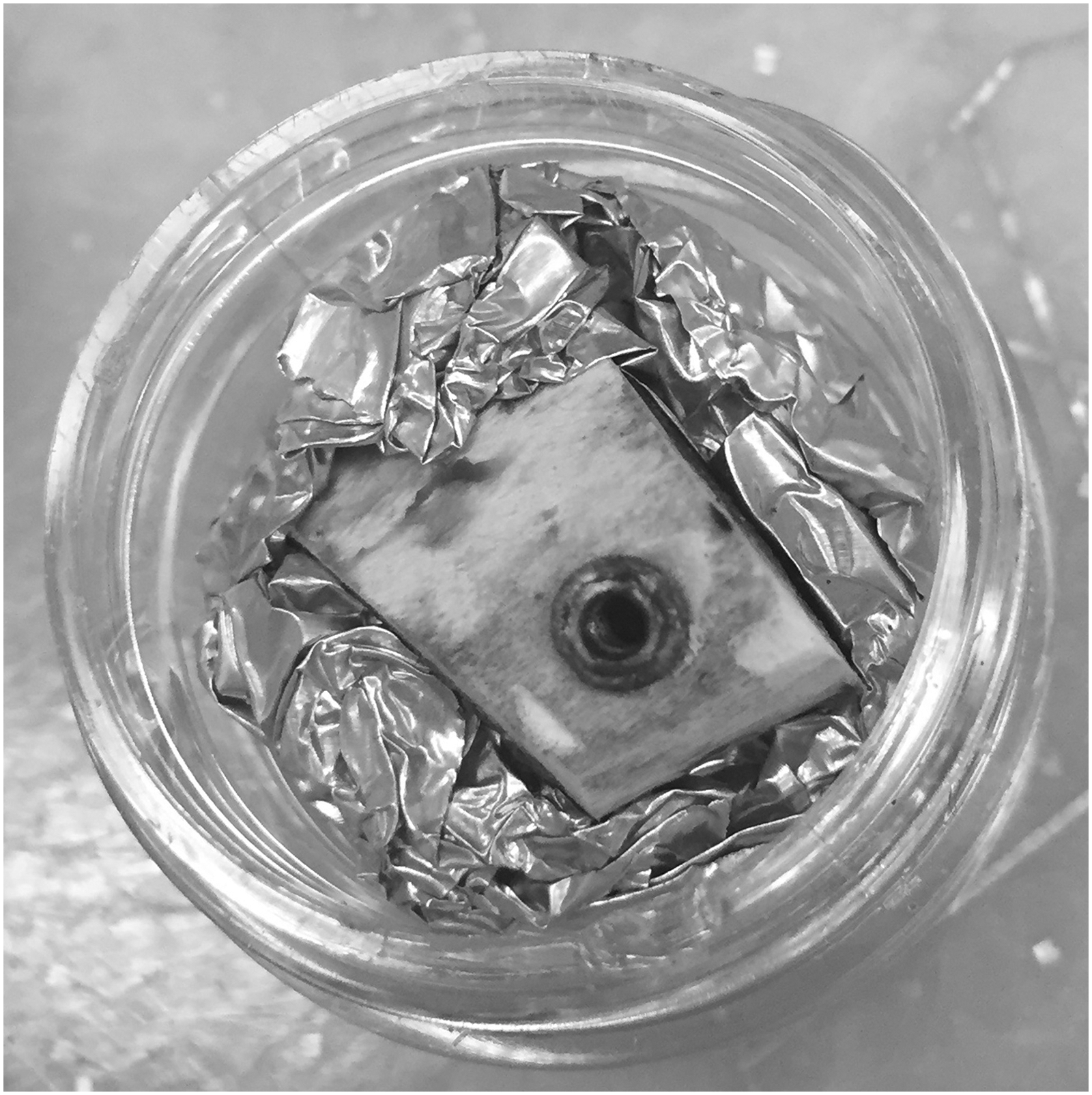
Study model. Implant placed in a bone block with a coronal angular defect created on its side.
Experimental groups: The samples were then divided into four experimental groups and two control groups. The first experimental group division was made according to the laser wavelength that was used, 810 or 980 nm. Two main groups were divided into two subgroups each depending on the application of photodynamic or normal laser therapy. Two control groups, one not treated by laser and a second not treated but coated with ICG dye, were used, for a total of six groups with 22 samples each (Fig. 2).
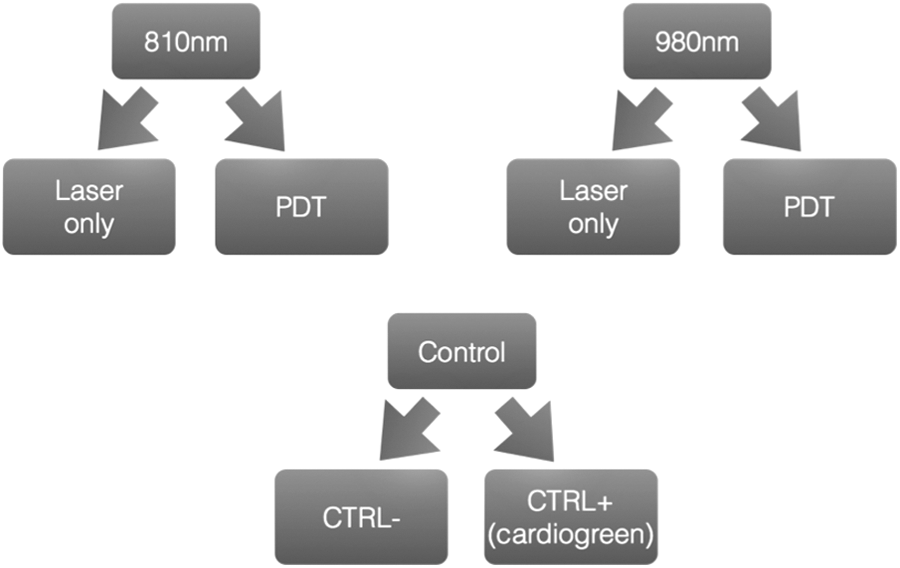
Experimental group subdivisions. The graph represents the division of the groups according to the use of the different types of laser and the adjunct of the photosensitizer dye. PDT, photodynamic therapy.
Photodynamic therapy: ICG is supplied as a stable dry (tablet) form, which is readily soluble in water (1 mg/mL). In dispersed soluble form, ICG binds to cellular lipoproteins and when exposed to laser photonic energy (<200 mW), with optimal peak absorption at 805–810 nm, near-infrared wavelength is able to produce photosensitized cellular damage. 53 –55
ICG was diluted in sterile phosphate-buffered saline with a concentration of 1 mg/mL and kept in the dark.
Decontamination
After 24 h, the experimental group was treated either with the 810 nm (2.4G Odyssey; Ivoclar Vivadent, Amherst, NY) or the 980 nm (Sirona SIROLaser, Bensheim, Germany) diode laser, with or without the aid of PDT according to group allocation. The laser fiber optic tip was placed into the defects for 60 sec set at 1.0 W continuous and kept 3 mm away from the implant surface. An up and down and side to side motion was used to apply the laser to the angular defect.
In the PDT group, before laser irradiation, 65 μL of ICG was applied into the defect with a pipette, allowing the dye to wet all the surrounding surfaces, and the laser light was applied immediately in the same manner as in the Laser Only groups.
The choice for the laser power settings used in this study was made after the results of pilot studies showed that data following decontamination with wattages of 0.6 and 0.8 W were inconclusive and that wattages exceeding 1 W showed histologic alteration of the bone. 56,57
Analysis of decontamination
After laser treatment, the implant defects were rinsed using transport media to ensure that the S. sanguinis was successfully retrieved. Each defect was rinsed thrice, and the media retrieved was then placed in 200 μL of tryptic soy broth contained in sterile microtubes. The microtubes were vortexed, and 100 μL of the media plated on tryptic soy agar plates. The plates were placed in an incubator with the atmosphere of 5% CO2 at 37°C for 48 h. After incubation the colony forming units (CFU) were counted on each plate by eye and recorded.
Statistical analysis
The statistical analysis of the CFU count was done using independent sample Kruskal–Wallis test, and a multiple comparison between groups was performed using pairwise comparisons of treatments. The significance level was established at 5% (α = 0.05), and the analyses were performed using SPSS software (IBM Corporation).
According to the a priori test, given an α of 0.05, a power (1−β) of 0.95, and a number of groups of 6, to have an effect size of at least 0.40, we needed a total sample size of 132, with 22 per group. The a priori test was performed with G*Power software (Franz Faul, Edgar Erdfelder, Albert-Georg Lang, and Axel Buchner, 2006, 2009).
Temperature measurements
In a second phase of the study, a 4 × 14 mm implant was placed in a bone block with the same characteristics and with the same angular defect used in the first part of the study, to test the thermodynamic effects of the laser application on the implant surface using thermocouples. Two lateral perforations, one central and one on the lower margin, were drilled on the side of the bone block for access for the thermocouples; three thermocouples were then positioned, coronally (at the contact interface between the bone and the implant shoulder), centrally, and apically on the implant surface, and the implant was then irradiated in the same way as in the first phase of the study (Fig. 3). Initial temperatures were recorded, and the change in temperature was monitored for 60 sec. Temperatures were registered at every 10 sec time point. The experiment was repeated at room temperature (around 22°C) and in a 37°C water bath with the same settings used during the decontamination test; while the bone block was under water, the coronal part was kept slightly above the water level to mimic the actual clinical condition and to avoid any distortion of the laser light given by the water.

Specimen with thermocouples. The three thermocouples are placed on the coronal, central, and apical aspect of the study model to record the temperature changes during irradiation.
Results
Decontamination
The results for the CFU counts are summarized in Table 1 and graph (Fig. 2). Our study shows that both laser's wavelength minimizes CFU counts with mean values for the groups treated with laser only or PDT being lower than those of the control groups. The use of PDT showed a modest increase in the decontamination effect, with the difference being more marked in the 810 nm groups. The 810 nm PDT group had a mean CFU count 3.591 lower than the 810 nm group; the 980 nm PDT group had a mean CFU count 0.227 lower than the 980 nm group. The 980 nm laser had a mean CFU count 6.727 lower than the 810 nm laser. The 980 nm used with indocyanine photosensitizer had mean CFU count 3.364 lower than the 810 nm with indocyanine (Table 1). However, as showed in the pairwise comparisons table, none of the test groups reached statistical significance compared with each other (p > 0.05). All the test groups showed a statistically significant increase in decontamination compared to the control groups, except for the 810 nm groups compared with the control+cardiogreen group (p < 0.05; Fig. 4).
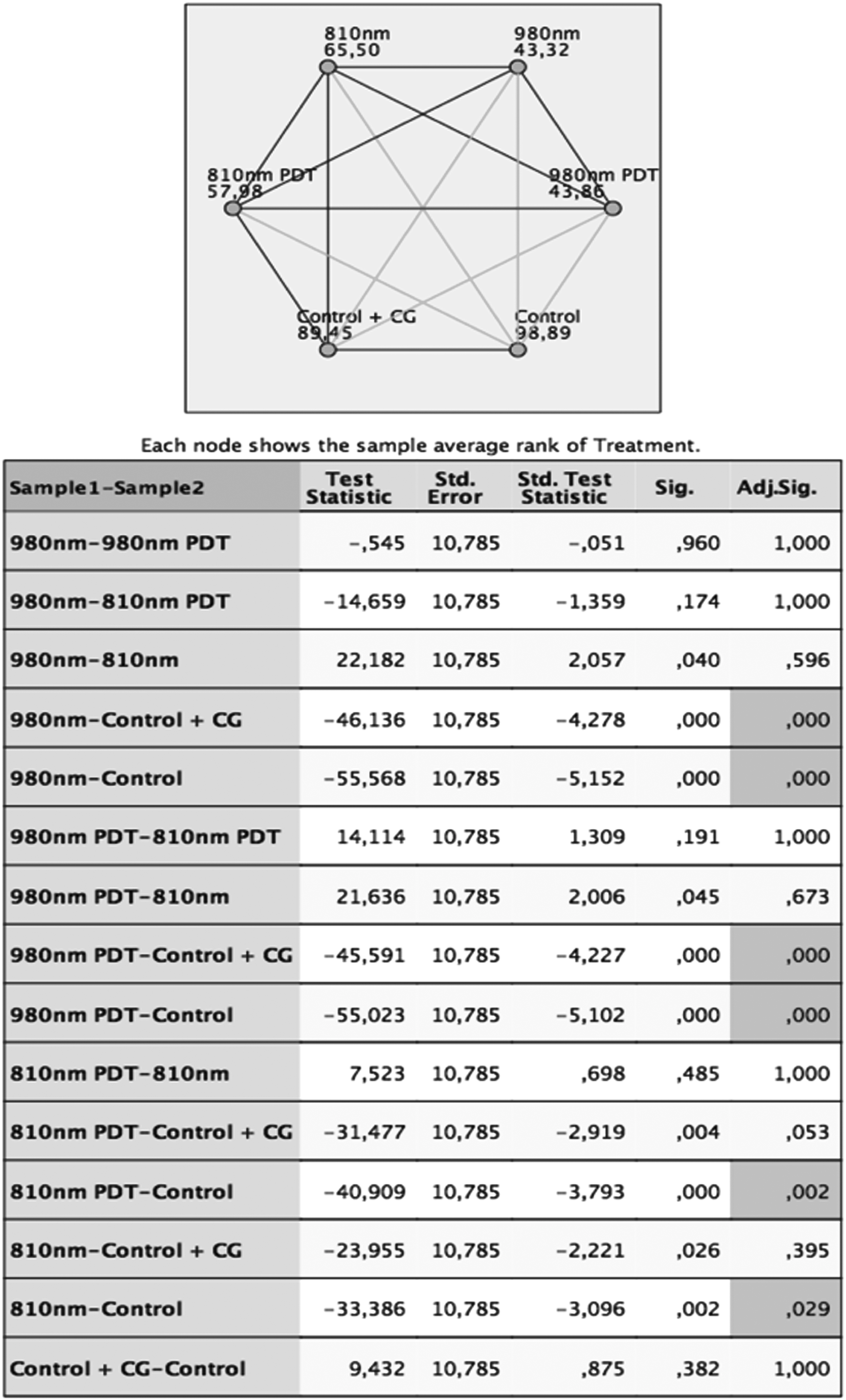
Pairwise comparison of treatment. Each row tests the null hypothesis that the sample 1 and 2 distributions are the same. The significance level is 0.05. CG, cardiogreen.
Groups, number of samples, mean CFU count, and standard deviation.
CFU, colony forming units.
Thermodynamic effects of laser
The results of the heating test are summarized in the table and graphs (Table 2 and Figs. 5, 6). ΔT is the difference between the temperature at 60 sec and the initial temperature. From the analysis of the results, it seems that a critical increase of >10°C is reached both with the 810 and 980 nm laser only when used at room temperature. No critical increase of temperature was registered when the bone block was placed in a 37°C water bath.
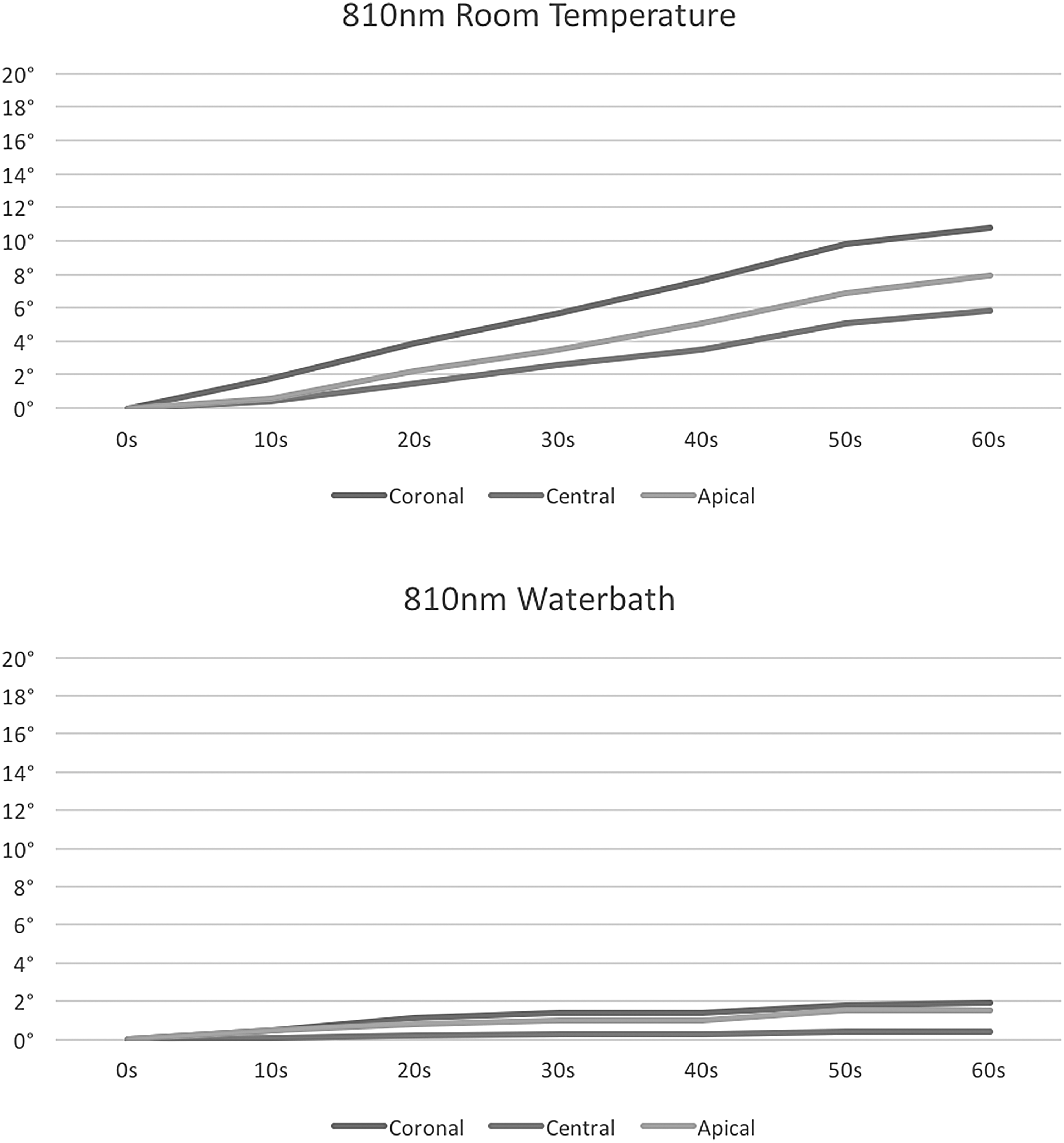
Temperature increase with 810 nm laser. Heating trend during 60 sec period at room temperature and in a 37°C water bath.
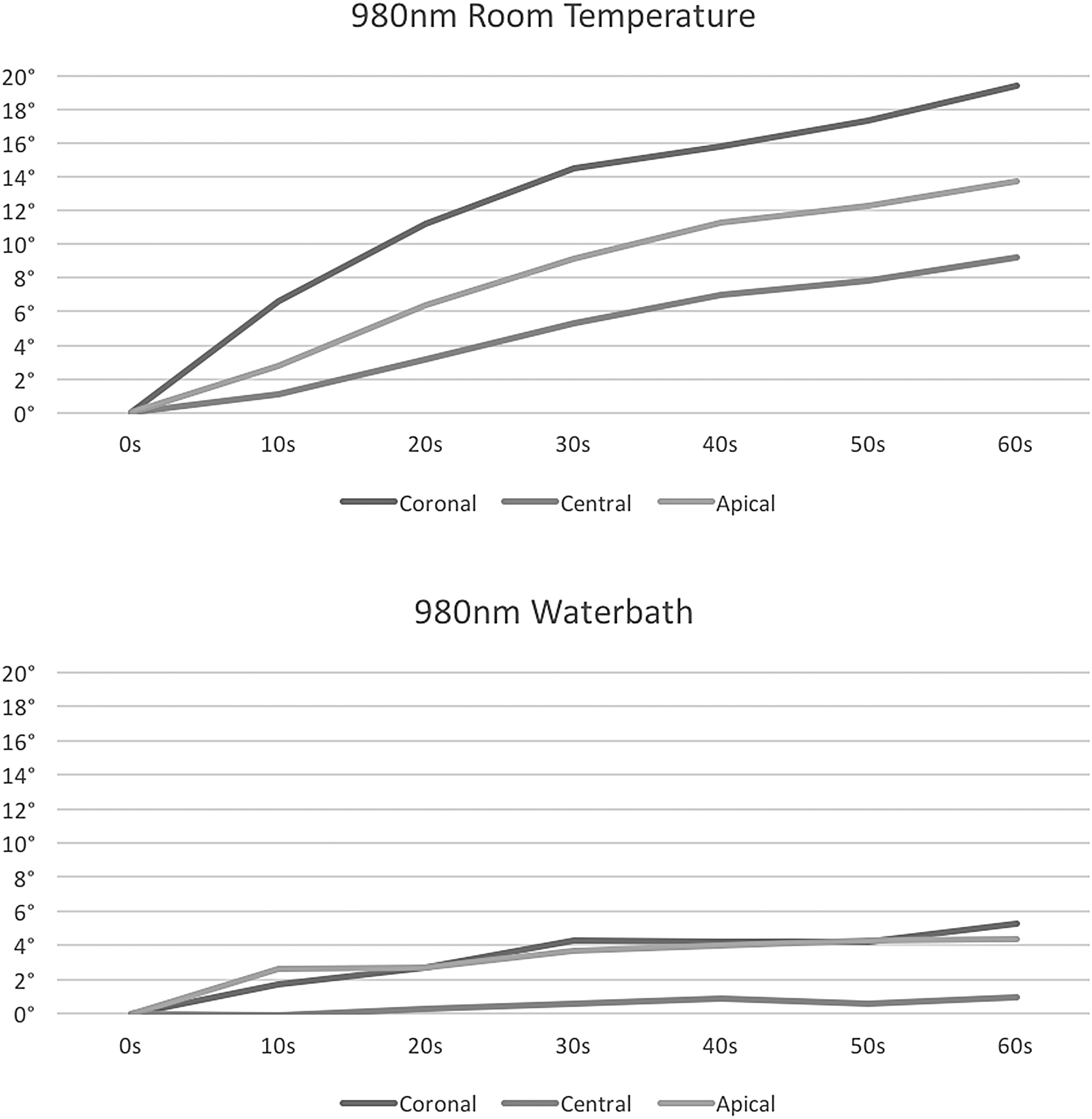
Temperature increase with 980 nm laser. Heating trend during 60 sec period at room temperature and in a 37°C water bath.
Cells in boldface report values that passed the critical temperature (10°C), cells in italic are <1.5°C under the critical temperature.
The highest increase in temperature was registered, as expected, always at the coronal point, which was the closest to the laser application; the lowest increase was registered at the central thermocouple.
Discussion
The use of diode lasers at 810 and 980 nm for implant surface decontamination was efficacious in this ex vivo study, with slight to no improvements given by the additional use of the ICG photosensitizer dye. There was a statistically significant difference when comparing the use of laser to the control groups, but not between the laser only and the PDT groups; the null hypothesis was then only partially rejected. In addition, the results of this study suggest that the use of these diode lasers does not cause a harmful increase in temperature when used under temperature conditions, which mimic those of the human body.
The results of the comparison between the two wavelengths, after CFU count, are consistent with those reported by Sennhenn-Kirchner et al. 9 in which, after comparison of the decontamination effect of 810 nm diode laser versus 980 nm diode laser on titanium sleeves contaminated with oral grown biofilm, no significant differences were found in either wavelength group. Both laser wavelengths produced rates of bacterial reduction around 99%. Concerning the comparison of the laser irradiation versus the use of photosensitization, our results are at odds with those obtained by Haas et al. 5 in which a significant difference was found between PDT group bacterial count and laser only bacterial count, with the second giving higher values. In the above mentioned study toluidine blue 100 μg/mL was used with a diode laser with a wavelength of 905 nm and left on the surface for 1 min before treatment. The wavelength used by Haas et al. does not correspond however to the wavelength at which toluidine blue has its peak of absorption (630 nm); the positive results obtained are therefore surprising. In our study, although the mean CFU counts for the PDT groups were lower compared to the laser groups, statistical significance was not reached. Moreover, the mean CFU counts show a noticeable difference between photodynamic and non-PDT only in the 810 nm groups. That was expected because ICG has its absorption peak around 800 nm, which rapidly drops after this wavelength. 58,59 This particular absorption peak represents one of the big advantages of this photosensitizer. In fact it can be used with a laser wavelength, namely the 810 nm, that can be applied for numerous other applications in dentistry (other than PDT) and has a deeper penetration in biological tissues (up to 10 mm) compared to the wavelengths (around 660 nm) that can be used with the most commonly used photosensitizers (8 mm). 60 An incubation of the photosensitizer was not provided before treatment in our study, and the laser light was applied after a few seconds from the application of the dye on the surfaces. The effect of different times of incubation of the dyes on the treated surface will be the object of a future research in our laboratory.
In the evaluation of the thermodynamic effects of the irradiation, when considering the coronal thermocouple, consistently with the study from Leja et al., 61 the 810 and 980 nm lasers at 1 W in continuous reached an increase over the critical threshold when used at room temperature. The 980 nm attained an increase of temperature that was double the critical one (10°C). Higher wattages of 2 and 5 W were not tested in this study, as their effects were already histologically analyzed in a previous pilot study and were considered to be harmful. 57
The apical thermocouple had an increase of temperature over the critical threshold, when the laser was used at room temperature, only when used at 1 W in continuous with the 980 nm laser. The central thermocouple never registered an increase over 10°C.
When the sample was placed in a 37°C water bath to mimic body temperature conditions, none of the power settings reached a critical temperature.
The highest temperatures registered have always been those at the coronal area, which was the closest to the irradiation area. The lowest trends were always registered for the central thermocouple.
While the coronal portion of the implant will be most probably exposed due to the peri-implant disease related bone resorption, the apical and central portion of an implant affected by peri-implantitis is more likely to be completely surrounded by bone in the clinical setting. A critical increase of temperature in the apical portion of an implant would be at a higher risk of causing bone necrosis. The fact that, even at room temperature, we did not exceed critical temperatures in the implant's central and apical areas is encouraging as far as clinical use is concerned.
A limitation of this latter experiment, similarly as in Leja et al. study, is that the irradiation was performed freehand by an operator, thus possibly causing an uneven heating of the implant surface because of irregularities in the movement. However, this represents the true clinical procedure, therefore, clinically relevant. The principal strength was the fact that the sample was placed in a 37°C water bath to replicate the temperature and conditions of the human body, and under these conditions, the samples showed no biologically critical increases in temperature.
The diode laser is the most common type of laser produced with a wide range of uses in dentistry. It is a relatively safe, easy to use, and cost-effective option compared to the other types of lasers. For these reasons, we consider it useful in the treatment of peri-implant disease. We decided to test its capabilities in terms of antibacterial action. Moreover, previous pre-clinical and clinical studies that have used diode laser, with or without photosensitization, have shown encouraging results. 5,7,9,12 –14,17,19,20,23,25,26,36,37,39,62
The dye used in this study, ICG, is a tricarbocyanine that belongs to the large family of cyanine dyes and exhibits a molecular structure with amphiphilic properties that has both hydrophilic and lipophilic properties. Through photon-induced electron transfer, ICG is able to produce powerful photosensitized cellular damage. 55 ICG, which is FDA approved for cardiovascular use, has low toxicity, rapid elimination, and an absorption peak near 800 nm, which is close to most of the commercially available diode lasers' wavelength. 58 This dye has proven effectiveness as a light-activated antibacterial agent, for adjunctive use in wound healing or treating chronic infections of mucous membranes and skin; it has also been studied for the use in the decontamination of dental surfaces, but it has never been tested for decontamination of titanium dental implant surfaces. 63,64 For these reasons we studied the efficacy of its use with ICG as a photosensitizer in light activated decontamination of titanium implant surfaces.
Smooth implants were used because of their ease of handling during the microbiological laboratory procedures. The retrieval of residual bacteria, after contamination and decontamination, from a rough surface, using mechanical methods (vortexing and sonication) might give inconstant results due to the more retentive anatomy of the rough surface. Anyway, no significant differences have been found in terms of survival, microorganisms' adhesion, and colonization between machined and modern treated surfaces; as a consequence, we believe that our choice does not affect the significance of the study. 65 –67
The ex vivo model described in this study represents a unicum in the literature about in vitro experimental peri-implantitis model. A similar model, using bovine rib, has been used by Leja et al. 61 In that study, the model was used only to register the temperature changes after irradiation with different type of laser (not for decontamination purposes). To our knowledge, the model described herein is novel and has been used only in this and in our previous pilot studies. 56,68 Its uniqueness is represented by the similarity of the actual clinical condition represented by peri-implantitis, thus mimicking the challenges that the clinician has to face during the instrumentation of a peri-implant bone defect. The model is also reproducible. We can evaluate the antimicrobial property of the device used not only on the implant surface but also within the bone defect through use of our reproducibly designed defect.
Within the limits of this ex vivo study and the necessity of augmenting the sample size, the clinical relevance of this experimental protocol can be inferred by the optimal results that the use of laser gave in terms of decontamination. The decontaminative potential is supposed to be reproducible in the clinical environment when we are treating cases of peri-implant mucositis or peri-implantitis. Given the almost equal potential of 810 and 980 nm diode lasers, the slightly increased risk of overheating of the 980 nm diode, and the better potential of taking advantage from the green dye of the 810 nm diode, the latter might be preferred for the clinical use. The use of the ICG in the clinical oral environment must be further investigated.
Conclusions
In conclusion, the use of diode lasers, at 810 and 980 nm, for implant surface decontamination is efficacious in this ex vivo study, with slight to no improvements given by the additional use of the ICG photosensitizer dye. In addition, the results of this study suggest that the use of these diode lasers does not cause a harmful increase in temperature when used under conditions similar to those of the human body.
Footnotes
Acknowledgments
The authors thank Dr. Erica Lavere for her precious contribution in the realization of this study.
Author Disclosure Statement
No competing financial interests exist.