
Abstract
Introduction
A
The commonly used irrigation technique is conventional syringe irrigation (CSI), a limitation of which is that the irrigant is incapable of reaching and cleaning the full length of the canal. 10 Therefore, many irrigant-activation techniques have been suggested not only to increase the efficacy of irrigant delivery and improve root canal cleanliness but also to remove debris or medicaments from the root canals more effectively. 10 –13
An endodontic microbrush, the CanalBrush (CB, Roeko CanalBrush™; Coltène/Whaledent, Langenau, Germany), is used manually with a rotary action. This highly flexible microbrush is molded entirely from polypropylene and has been found to be more efficient when operated at 600 rpm by using a contra-angle handpiece. 13 The EndoActivator (EA; Dentsply Tulsa Dental, Tulsa, OK), a sonically driven canal-irrigation device, has been shown to better irrigate the root canal system by energizing the irrigants with a flexible, non-cutting polymer tip. 11 Photon-induced photoacoustic streaming (PIPS), a light-energy phenomenon, differs from other activation techniques in that it places only the tip into the coronal portion. This technique uses an Er:YAG laser with a novel, tapered tip that has a radial firing end. The short-level laser energy creates a strong photoacoustic shock wave, improving the irrigant's penetration into the root canal system without any contact of the laser tip with the root canal wall. 12
Previous studies have focused on preventing precipitate formation by using a chemical substance as an intermediate flush to remove residual NaOCl before irrigation with CHX. 3,14,15 However, data are lacking on removal of precipitate from the root canal system when it accidentally forms in the root canals. Only one study in the literature examined the effectiveness of two irrigant-activation techniques to remove the precipitate from the root canals, and it concluded that both passive ultrasonic activation and the agitated F-file technique failed to completely remove precipitate. 16 However, it is still unclear whether manual instrumentation (MI) and different irrigant activation systems can effectively remove precipitate that is firmly attached to the root canal walls. Therefore, the aim of the present study was to compare the efficacy of various irrigation techniques (CSI, CB, EA, and PIPS) with the MI technique for removing precipitate from the root canal walls.
Materials and Methods
The study selected 82 recently extracted, single-rooted, non-carious, anterior teeth with similar dimensions and intact apices from a collection of teeth extracted under conditions unrelated to the study. The teeth were stored in distilled water until used. Calculus, bone, and residual soft tissue were removed from the external surfaces of the teeth. After preparation of the endodontic-access cavities, the length of each tooth was measured by inserting a size 15, stainless-steel K-file (DentsplyMaillefer, Ballaigues, Switzerland) with its tip visualized at the apical foramen. To obtain a standardized root length of 19 mm and a working length (WL) of 18 mm, the crowns of the teeth were partially removed. The teeth were then fixed in modified Eppendorf vials (Eppendorf-Elkay, Shrewsbury, MA) with a silicone material (Optosil; Heraeus Kulzer, Hanau, Germany) to create a closed system resembling clinical conditions. This prevented the escape of irrigants from the root apex and allowed ease of handling during instrumentation.
After rubber-dam isolation, the root canals were instrumented by using the ProTaper rotary system (DentsplyMaillefer) up to size F4 (size 40) as the master apical file. Between each instrument change, irrigation was performed with 2 mL of 5% NaOCl (Wizard; Rehber Kimya, Istanbul, Turkey) from a 27-G, double side-vented needle (ScaniaDental AB, Knivsta, Sweden). After instrumentation was completed, 5 mL of 17% EDTA (Wizard; Rehber Kimya) was used for 1 min, followed by 5 mL of 5% NaOCl for 1 min. Finally, with the exception of 5 teeth (negative controls), the root canals were irrigated with 2% CHX (Werax, Izmir, Turkey) for 1 min by using the aforementioned syringe and needle, which were positioned 1 mm short of the WL. Irrigants were delivered with an in-out motion and concomitant aspiration by using a surgical suction tip placed next to the pulp chamber. Then, the canals were aspirated and dried immediately with absorbent paper points.
To facilitate the splitting of the roots, two longitudinal grooves on the buccal and lingual surfaces were prepared with a diamond disk under water cooling while paying close attention not to perforate the canal space. The roots were then split into two halves with a chisel. The half that was covered with more parachloroaniline than the other one was coded and evaluated. The halves that showed the evidence that the teeth were not split in two equal sections were discarded and replaced by a new specimen.
The coded half was photographed by using a stereomicroscope (Nikon SMZ 1000; Nikon, Tokyo, Japan) with 15 × magnification attached to a digital camera. The images were transferred to a computer. Apical, middle, and coronal thirds were determined by marking the roots into three sections at 4, 8, and 12 mm from the apex. The area of the root canal surface covered with orange-brown precipitate was calculated in mm2 by using image-analyzing software (Kameram Digital Microscopy CCD). A small amount of Super Glue (Scotch Super Glue Gel; 3 M, St. Paul, MN) was used to obtain a close adaptation of the root halves, and then the specimens were repositioned in Eppendorf vials.
Precipitate removal procedures
The specimens were randomly divided into five experimental groups (n = 15) according to the precipitate-removal technique used. In addition to the negative control group (n = 5), 2 teeth that did not receive any removal procedures were used for scanning electron microscopy (SEM) analysis as a positive control group.
Group 1: CSI
Irrigation was performed with a 27-G, double side-vented needle and 5 mL of distilled water for 1 min. The needle was inserted to 1 mm short of the WL without binding.
Group 2: CB
Agitation of 5 mL of distilled water was accomplished by using a CB with a tip diameter of 0.30 mm in a handpiece set at 600 rpm. Distilled water was agitated with the CB for 1 min in a gentle up-and-down motion at 1 mm from the WL.
Group 3: EA system
Five milliliters of distilled water was flushed into the canal by using a 27-G irrigation syringe and agitated by using an EA handpiece with a medium polymer tip (no. 25/.04) set at 10,000 cycles/min and inserted 1 mm short of the WL for 1 min.
Group 4: PIPS technique
The PIPS protocol was performed with an Er:YAG laser (Fidelis; Fotona, Ljubljana, Slovenia) with a wavelength of 2940 nm. A 12-mm-long, 400-mm quartz tip was tapered, and 3 mm of the polyamide sheath was stripped back from its end. The tip was applied with 0.3 W, 15 Hz, and 20 mJ per pulse, as recommended by the manufacturer, without water/air spray. Then, 0.5 mL of distilled water was placed into the root canal, and the optical tip was placed into the coronal reservoir. When the irrigation solution in the coronal reservoir decreased, fresh distilled water was applied through the canal opening. The optical-fiber tip was activated during placement of the solution. The total activation time was 1 min, and the total volume of distilled water was 5 mL.
Group 5: MI
The canals were filled with 0.5 mL of distilled water and a stainless-steel, 45-K file was inserted to the WL for apical enlargement. Then, an MI technique was performed by using stainless-steel H-files (#45). The files were used in a circumferential motion while pressing against the root canal walls for 1 min. During instrumentation with the H-files, the roots were irrigated with 4.5 mL of distilled water by using a 27-G irrigation syringe inserted 1 mm from the WL.
For all groups, the total volume of distilled water used was 5 mL and the duration of the removal procedure was 1 min. The root canals were dried with paper points. After the roots were separated again, the mean area of remaining orange-brown precipitate was calculated. The mean percentage of precipitate removed from the canals in each third was calculated according to the following equation: [(The area of precipitate formed in the root canal − the area of precipitate after removal) × 100/The area of precipitate formed in the root canal]. After the removal procedures, two randomly chosen specimens from each group were prepared for SEM analysis. Tooth halves were individually dehydrated by a serious of graded ethanol solutions, mounted on aluminum stabs (Silverpaint; Agar Scientific Ltd., Stansted, Essex, United Kingdom), sputter coated with gold-palladium, and examined under SEM (Leo-440; Leo Electron Microscopy, Cambridge, United Kingdom) at a magnification of 2000 × .
Statistical analysis
Statistical analysis was performed with non-parametric tests, since the Shapiro–Wilks test showed no normal distribution. Kruskal–Wallis tests were used for overall comparisons, and Mann–Whitney U tests were used for pairwise comparisons, both of which were at the 95% confidence interval. The Friedman test was used to compare the percentages of precipitate removed from all root thirds (apical, middle, and coronal) within the same group, using a significance level of p < 0.05. All data were analyzed by using IBM SPSS Statistics version 22 software (IBM SPSS, Inc., Chicago, IL).
Results
Table 1 shows the results of statistically analyzing precipitate removal for all tested groups. None of the groups showed complete removal of the orange-brown precipitate from the root canal walls. The Kruskal–Wallis test showed statistically significant differences in precipitate removal among the experimental groups (p < 0.05). The MI group showed the highest percentage of precipitate removal (p < 0.05). The CB group removed significantly more precipitate than the EA group (p < 0.05). The CSI and PIPS groups showed the least precipitate removal (p < 0.05), with no statistically significant differences between the two groups (p > 0.05).
Median ± standard deviation in percentage (n = 15 for each group). Calculation was done as ([a − b]100/a), where a was the area of precipitate formed in the root canal and b was the area remaining after removal.
CSI, conventional syringe irrigation; MI, manual instrumentation; PIPS, photon-induced photoacoustic streaming.
Wilcoxon signed-rank tests showed that the CB and EA techniques were significantly more efficient for removing precipitate from the apical third than from the middle and coronal thirds (p < 0.017). The CSI, PIPS, and MI groups showed no significant differences in the amount of removed precipitate from the apical, middle, and coronal thirds (p > 0.05).
SEM examination showed no obvious debris and complete removal of the smear layer in the negative control group (Fig. 1A). However, in the positive control group, CSI group, and PIPS group, a flocculate precipitate seemed to block the dentinal tubules (Fig. 1B, C, F). In the CB and EA groups, there was sparser distribution of precipitate and partially opened dentinal tubules (Fig. 1D, E). In the MI group, the dentinal tubules were thoroughly covered with debris and smear layer instead of with a flocculate precipitate layer formed by orange-brown precipitate (Fig. 1G).
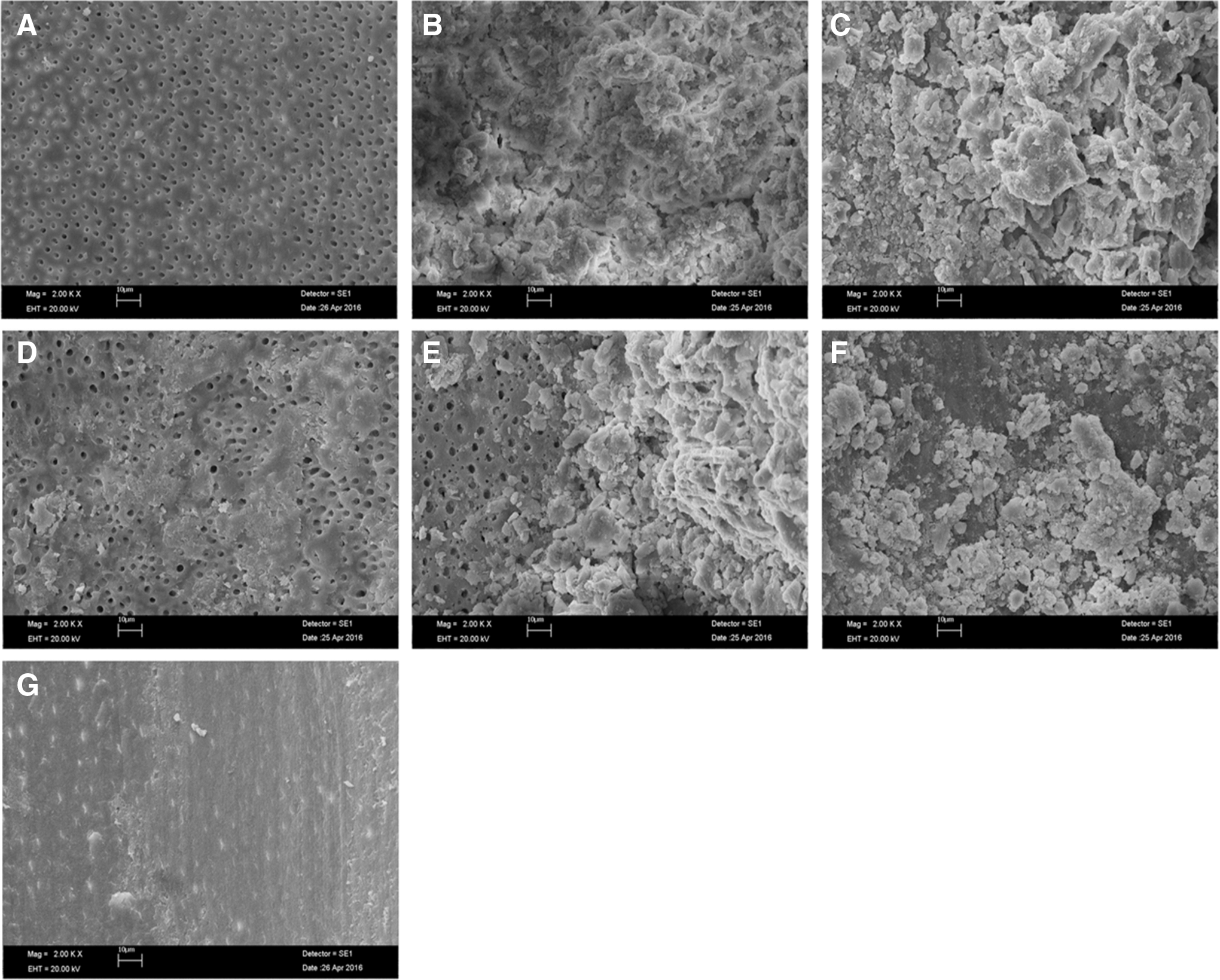
Scanning electron microscopy images of the middle thirds of the root surfaces (2000 × ).
Discussion
The literature contains no data regarding the efficiency of the five tested techniques in removing orange-brown precipitate formed on dentin surfaces irrigated with NaOCl and then CHX. However, the results of this study can be compared with those of studies that evaluated the efficacy of irrigation-activation techniques on removing debris, medicament, or antibiotic paste from the root canal walls.
Results of the present study showed that using the CB technique to agitate the distilled water improved precipitate removal from the apical thirds. Similarly, Salman et al. 17 reported that agitation using the CB technique enhanced root canal debridement in the apical portions of the root canals. Another study found that irrigation activation using the CB technique was better than that using the CSI technique for removing calcium hydroxide from the root canals. 18 In this study, the increased capability of the CB technique to remove precipitate may be explained by the fact that the brush used in this technique maintained better contact with the narrower parts of the root canal surfaces than did the other tips tested.
The present study showed that the EA technique was more effective than the CSI technique, especially on the apical thirds. This is consistent with the results of a recent study 11 that reported that the EA technique removed more of a modified triple-antibiotic paste than did the CSI technique, including the most apical parts of the root canals. The reason for the increased efficacy of the EA technique compared with the CSI technique could be due to the movement of the irrigant in the root canals, caused by the interaction of sonic vibration with bubbles. 19 Nevertheless, it is important to emphasize that in the current study, the percentages of precipitate removed by both the CB and EA techniques did not enable us to draw conclusions regarding clinical success.
Laser-activated irrigation using PIPS tips has been shown to be significantly more effective that the CSI technique at debriding root canals. 12,20,21 However, in the present study, the PIPS technique was inefficient, comparable to needle irrigation for removing precipitate. Unlike the other irrigation-activation techniques, the PIPS tip does not need to reach the root apex, and it is placed into the coronal reservoir of the root canal. Thus, the longer distance between the PIPS tip and the apical third of the root may explain the unsatisfactory results of the PIPS technique compared with the other tested techniques, in which the tips reached the root apices. In addition, another shortcoming of the PIPS technique may be its use of lower energy levels and short microsecond pulse rates (50 μsec). Therefore, further research is necessary to establish the appropriate laser types, parameters, and application times that are needed to efficiently remove orange-brown precipitate.
The use of an additional file in the MI technique made it superior to the other techniques for removing orange-brown precipitate. However, some precipitate remained in all specimens, even when an additional file was used in a circumferential motion while pressing against the root canal walls. Therefore, based on results of the present study, one may conclude that removing precipitate once it is formed in the root canal remains a challenge in root canal therapy. Thus, every precaution should be exercised to avoid precipitate formation during endodontic treatment.
In the present study, the SEM images were similar to those from previous studies, which showed that after successive use of NaOCl and CHX, a precipitate formed, coating the root surfaces and obliterating the dentinal tubules. 4,7 Akisue et al. 7 reported that this flocculate precipitate acted as a “chemical” smear layer that reduced the dentinal permeability. The present study showed that after MI, the chemical smear layer was replaced with debris and smear layer. Future studies should characterize the nature of this “replaced” smear layer and determine whether the precipitate is still present in the dentinal tubules after removal procedures.
Previous studies have recommended using chemicals, including alcohol and ethanol, as an intermediate flush between NaOCl and CHX to reduce precipitate formation. 2,3 However, the biocompatibility of such solutions with the periapical tissues remains a concern. 3 Therefore, the current study used agitated distilled water because of its biocompatibility 22 and because it enabled observation of only the mechanical effects of the irrigant agitation techniques. However, the results of the present study reflect the challenges associated with removing orange-brown precipitate from the root canal walls by using distilled water agitation.
Conclusions
According to the findings of the present study, no tested technique completely removed the orange-brown precipitate from the root canal walls. However, the MI technique showed better results than the CSI, CB, EA, and PIPS techniques. Further research is warranted to identify techniques and irrigants that can completely remove precipitate from the root canal system.
Footnotes
Acknowledgments
The authors would like to thank Dr. Aslihan Usumez for supporting the laser tips.
Author Disclosure Statement
No competing financial interests exist.