
Abstract
Introduction
T
The bactericidal action of the used irrigants such as NaOCl, ethylenediaminetetraacetic acid (EDTA), and MTAD (doxycycline, citric acid, and a detergent), requires a direct contact along the dentin surface. 2 Besides, Berutti et al. reported a limited penetration depth of these irrigants to about 100 μm because of surface tension compared with bacteria that can breach ∼1000 μm in dentin. 3 Further, the high percentage of ramifications and variations of the apical root third escapes the debriding action of conventional chemomechanical preparation procedures, leading to recurrent infection. 4 Enterococcus faecalis, as a gram-positive nonspore-forming bacterium, belongs to the phylum Firmicutes with streptococci as the nearest neighbor and can form intra- and extraradicular biofilms, allowing cells to survive under extreme conditions. This fact highlights this species as the stubborn invader of root canal dentin 5 and it is—together with Candida albicans—frequently found in secondary root canal infections and recrudescence, 6 consequently it is a suitable indicator of the clinical relevance of this in vitro study.
Laser-assisted endodontic treatment has been postulated as an innovative approach to disinfect the deep layers of radicular dentin. Depending on the wavelength, lasers show a better access to formerly unreachable part of the tubular network. 7 –9 Klinke et al. reported an antibacterial effect of Nd:YAG laser within the root canal dentin up to a depth of 1000 μm with an efficiency of 84.8%. 7 According to the absorption spectra of dental hard tissue, diode lasers possess the ability to penetrate deep inside dentinal tubules. 10 Besides, Hmud et al. described the formation of a limited form of cavitation in aqueous fluids around the top of the fiber that could potentially disrupt bacterial biofilms, rupture bacterial cell walls, and remove smear layer and debris. 11
An average bacterial reduction of 58% was achieved when Er,Cr:YSGG laser with a distal output of 0.25 W and a frequency of 20 Hz was used to irradiate dentin slice thickness of 500 μm. 12 In another study conducted by Beer et al., an average bacterial reduction of E. faecalis of 68.15% was reported with the 940 nm diode laser when irradiating prepared root samples with 1.5 W, 0.05 ms pulse duration, and 0.15 ms pulse period. 13 Despite the good results achieved by different wavelengths in endodontics, there is still some improvement in the fiber tip delivery. When irradiating the root canal system, although a large part of this radiation will be propagated toward the apex of the root, part of this beam will be expanded to a certain degree when leaving the end of the fiber tip because of total reflectance at the fiber wall. A new generation of radial firing fiber tips (RFTs) has been developed to allow a more homogeneous irradiation of the root canal walls. The ends of these radial-emitting fiber tips show a conical outline with a cone angle of 60°. The laser light is expanded to a broad cone, aiding a homogenous coverage of the whole root canal wall. This can positively influence debris removal and bactericidal efficiency of the laser along the root canal system. 14 Using an RFT, an Er,Cr:YSGG laser at 0.9 W, 20 Hz pulse repetition rate was capable of removing E. faecalis to an extent of 3 to 4 log steps. 14
The aim of this in vitro study was to investigate the bactericidal effect of a 940 nm diode laser delivered through prototype RFTs in elimination of E. faecalis by indirect irradiation of bovine dentin slices of different thicknesses in comparison with bare fiber tips (BFTs).
Materials and Methods
Samples preparation
Fifty-five caries-free bovine teeth were cleaned and sectioned at the cementoenamel junction with the aid of a diamond band saw (Exact GmbH, Hamburg, Germany). Using a saw microtome (Leitz Wetzlar GmbH, Wetzlar, Germany), a total number of 100 slices of bovine root dentin were prepared parallel to the root canal lumen with two different thicknesses (500 and 1000 μm). The thickness of the dentin slices was checked by a vernier, and slices of tolerance less than ±5 μm were excluded from the study. Afterward, the slices were immersed in an ultrasonic bath with 17% EDTA for 1 min to remove the inorganic portion of the smear layer followed by irrigation with NaOCl for removal of the remaining organic components according to the guideline of the American Association of Endodontists regarding cleaning the root canal in clinical cases. 15,16 The resulting cleaned slices were stored individually in 1% thymol added to sterile physiological saline solution at temperature of 4°C until further use.
Bacterial inoculation
To simulate the in vivo clinical situations, the bacterial suspension was applied onto the dentin slices in the shape of a line to have the same size and length of an ISO 40#. The inner circumference of an ISO 40# prepared root canal is almost 1.26 mm (π·0.4 mm) and with a typical length of 16 mm, which results in a root canal wall surface area of ∼20 mm2. A region of 16 × 1.26 mm was marked on both sides of the slice for bacterial inoculation and laser irradiation from the noninoculated side. The slices were randomly assorted into a sterile plastic polymerase chain reaction (PCR) tube (Eppendorf Vertrieb Deutschland GmbH, Wesseling-Berzdorf, Germany), labeled only with numbers to conduct the study blinded without knowing allotment of slices to any of the eight test groups or the two control groups (n = 10). The instruments and the dentin slices were sterilized in an autoclave (Napid 30; SMS GmbH, Emmingam-Liptingen, Germany) at a temperature of 121°C for 30 min to remove all contaminants. Then, with a calibrated micropipette, 1 μL of a standard (2.0 × 107 cells per microliter Luria broth medium) E. faecalis (strain ATCC 29212) suspension was inoculated on one side of the slices. After 30 sec drying period, laser irradiation was performed. 17
Samples grouping and laser irradiation
A commercially available 940 nm diode laser (EPIC 10; Biolase, Inc., Irvine, CA) was used. The delivery system was through a 200 μm diameter and 21.17 mm length prototyped RFT fiber that allows laser light to be emitted laterally and a 200 μm diameter and 21.17 mm proprietary BFT. A total number of 100 slices were prepared for the two selected dentin thicknesses, 500 and 1000 μm (each n = 50). The inoculated surface was then irradiated indirectly from the noninoculated side for 8 sec in a close contact situation. A 5° incident angulation was maintained between the fiber tip and the dentin slice to simulate the situation in the root canal. For each thickness, 10 samples were irradiated with each fiber tip design; RFT and BFT, with a power of 1 and 1.5 W in continuous wave (CW) mode 18,19 that was checked before each irradiation using a wattmeter (Type LM3; Coherent, Inc., Auburn, CA). The laser fiber was moved in a scanning pattern of 2 mm/sec for 8 sec, resulting in a total energy of 8 and 12J for the output power of 1 and 1.5 W, respectively. For each sample, the laser output power was measured and a new fiber tip was used to ensure stable and standardized power outputs from the distal fiber tip. The laser irradiation cycle was repeated four times with a 10 sec time interval in between. The remaining 10 samples of each thickness were treated in the same way as the tested samples except for the laser irradiation, and served as a positive control.
Bacteriological analysis
The inoculated dentin slices, including the tested (treated) and control slices, were placed individually into sterile plastic PCR tubes (Eppendorf Vertrieb Deutschland GmbH) containing 1 mL of a physiological salt solution (0.9% NaCl). The surviving bacteria were separated from slices by vortexing. The plastic PCR tubes were stored on ice over the whole experiment to reduce unintended bacterial growth or death to a minimum. From this 1 mL suspension, serial dilutions of log 10 steps were produced, and a 20 μL aliquot of the last three dilutions was plated onto CASO blood agar plates with 5% defibrinated sheep blood and incubated overnight at 37°C in an atmosphere of 10% CO2. After this incubation period, the E. faecalis colony-forming units (CFUs) of treatment survivors and controls were counted and evaluated. Statistical analysis to compare CFU values using the nonparametric Kruskal–Wallis and post hoc Dunnett tests for multiple comparisons was performed by SPSS Statistics 20 (IBM® Corp., Armonk, NY). p Values of <0.01 were considered as statistically significant.
According to Rooney et al.,
20
the results were indicated in “log kill.”
where a is the CFU in the inoculation suspension and b is the CFU in the eluate of the test or control group.
To recalculate log kill data into a percentile reduction R, R yields as
Examining these formulas makes it visible that an increased bacterial reduction from 99% to 99.9% is not just 0.9% but also a 10-fold increase or as high as 1000%, as the log kills in this example increases from 2 to 3.
Temperature measurements
To investigate the thermal impact of 940 nm diode laser delivered through RFT and BFT, temperature changes in the external root surface were measured. For this measurement, the experimental setup was implemented as described by Al-Karadaghi et al. 21 and Falkenstein et al. 22
A number of human single-rooted teeth were prepared up to ISO 50# and cleaned with NaOCl (2.5%) and EDTA (according to the American Association of Endodontists). Then, the sample was fixed in polyurethane resin material (ISO-PUR K 760; ISO ELEKTRA, Elze, Germany) mixed in a ratio of 6:1 to possess a thermal conductivity of 0.7 W/m K and a density of 1.4 × 103 kg/m3. Four K-type thermocouples (Omega Engineering, Inc., Stanford, CT) with wire diameter of 0.13 mm and an accuracy of ±0.691°C were fixed with adhesive wax on the external root surface. The position of thermocouples was radiographically confirmed to be 1000 μm, 4, 8, and 12 mm from the apex. To improve heat conduction from the root surface to the thermocouples, a thin layer of heat conductive silicone compound (Fischer WLPF 50, 0.7 W/m K) was applied. The model with the attached thermocouples was submerged in a water bath (36.6°C ± 0.05°C). With a sampling rate of 5 Hz, the data were logged to the PC through an USB data acquisition module (OM-USB-TC; Omega Engineering, Inc.). The difference values between baseline and maximum temperature after laser irradiation with the standard deviations of the five measurements per laser setting were calculated subsequently and analyzed.
Results
Bacteriology
Table 1 gives an overview about all results of bacterial counts measured and calculated reduction of log kill, average and minimum/maximum reduction after 940 nm diode laser irradiation with different fiber tips (RFT versus BFT), and output power (1 vs. 1.5 W) on bovine dentin slices of different thicknesses.
Indicates significant (p < 0.0001) difference in comparison with control group.
Indicates significant difference (p < 0.0001) between laser groups.
BFT, bare fiber tip; CFUs, colony-forming units; RFT, radial firing tip.
The number of E. faecalis cells recovered from slices in the untreated control group (2.31 × 107 CFU/mL) was slightly higher than that of the suspension inoculated (2.00 × 107 CFU/mL). This could be because of several processes such as multiplication of some cells and death of others during the time between inoculation on slices and plating on agar, resulting in a negative log kill value of about 0.15 (Fig. 1). Further, it shows that the vortexing process did recover attached E. faecalis cells quantitatively.
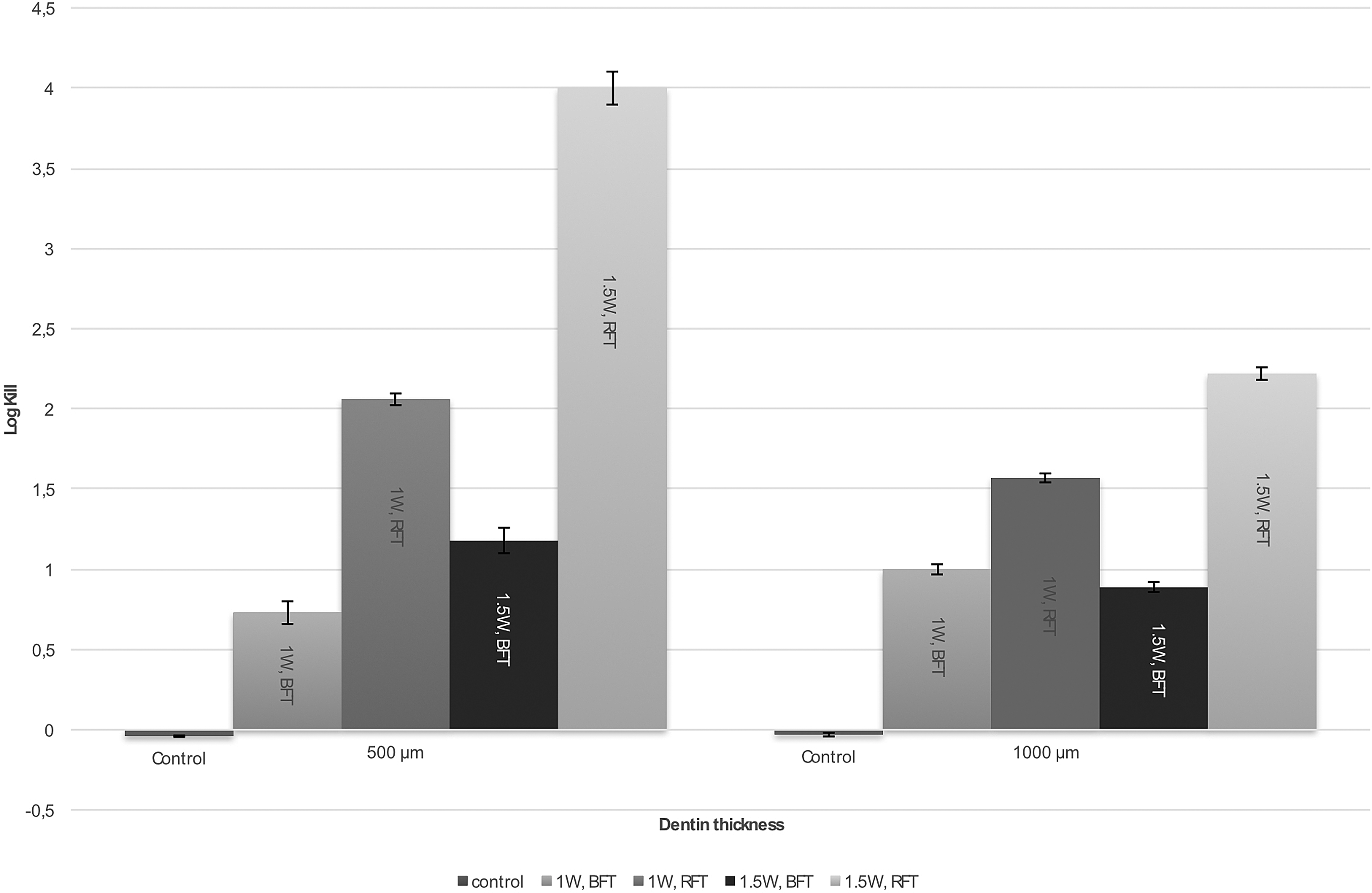
The average log kill and standard deviation of dentin slices of different thickness irradiated with 1 and 1.5 W output power of 940 nm diode laser emitted through two fiber designs, RFT and BFT, compared with nonirradiated control samples. BFT, bare fiber tip; RFT, radial firing tip.
The diode laser delivered by RFT fiber succeeded in a major reduction of E. faecalis cells, even at an output power of 1 W with a log kill of 2.06 (99.13%). By increasing the power to 1.5 W, one could reckon a more effective bacterial reduction to 4 log kill (99.99%) in 500 μm-thick dentin slices (Fig. 1; Table 1). As the dentin slice thickness was increased to 1000 μm, a decrease in the bacterial log kill by RFT fiber group at 1 W to an average log step of 1.57 (97.31%) left about 4.4 × 105 CFU/mL of survivors. In contrast, diode laser delivered by BFT removed E. faecalis cells to an extent between 0.73 (81.38%) (500 μm, 1 W) and 1.18 log kills (93.39%) (500 μm, 1.5 W) (Table 1).
The Kruskal–Wallis (nonparametric analysis of variance) analysis showed that in both control groups, significantly more viable bacteria were found than all test groups (p < 0.0001). For multiple comparisons between the groups, the Dunnett test was used and the results showed significantly more surviving bacteria in the BFT group than in the RFT-treated group, both more than 500 and 1000 μm dentin slices (p < 0.0001). Interestingly, in samples of 1000 μm thickness, there was no significant difference in the bacterial count of the BFT group as we increased the power from 1 to 1.5 W (p = 0.08). Significantly, a higher bacterial reduction was recorded in RFT design when the power was increased to 1.5 W (p = 0.0002) as shown in Table 1.
Temperature measurements
When an output power of 1 W was tested, samples irradiated with both fiber designs resulted in a temperature difference of less than 2.9°C from baseline temperature in the apical part of the root. A higher output of 1.5 W yielded a higher average temperature of 3.2°C in the BFT group (Fig. 2). All temperature measurements at specific dentin thickness are presented in Table 2. Although a higher irradiation power results in greater temperature increase in bare fiber design at 1000 μm from root apex, the temperature stays within safe boarders in all tested groups.

Maximum temperature changes (ΔT) and standard deviation on the external root surface, 1000 μm from the apex, after irradiation with 1 and 1.5 W diode laser delivered by two fiber designs.
Discussion
Various types of lasers have been used successfully in endodontics for removal of smear layer, pulp remnants, and disinfection of dentinal tissue. However, the laser delivery system and fiber optic still show some space for development. The objective of our study was to evaluate the effectiveness of the 940 nm diode laser irradiation delivered through a 200 μm RFT fiber compared with a BFT in relation to an output power of 1 and 1.5 W. To our knowledge, this fiber delivery system and the antibacterial depth of 940 nm diode laser have not yet been investigated.
The reported results of this study showed that diode laser applied through RFT at an output power of 1.5 W described a high bacterial reduction of 4 log steps equivalent to a reduction of 99.99% at 500 μm dentin slice thickness.
The bactericidal effect of different wavelengths has been reported to range between 13% and 99.7% as shown in Table 3. Bergmans et al. reported a reduction in the bacterial load to 99.7% after irradiation of root canals inoculated with E. faecalis with 1.5 W and 15 Hz of Nd:YAG laser for 20 sec. 23 The fiber, therefore, was held in direct contact with the bacteria. On the contrary, an average bacterial reduction of 99.4 was achieved in this study by indirect irradiation given by samples of thickness of 1000 μm by means of a diode laser and an output power of 1.5 W in conjunction with RFT. Owing to the compact size, low cost, and the wide variations of power settings and operation modes, the use of diode lasers remains interesting. 10 Even when the diode laser was delivered through the conventional BFT design, a satisfactory reduction in the bacterial load of 1.18 log steps equal to reduction percentage of 93.39 has been achieved as the output power increased to 1.5 W in 500 μm slice thickness, this is in agreement with Gutknecht et al. 17 and Beer et al. 13 (Table 3).
RFT indicates results with a radial firing tip, BFT indicates results with a bare fiber tip. Rows are sorted with ascending wavelengths. For continuous operation (CW) modes, the power is listed next to the pulse duration.
n.a., not applicable.
In a recent study conducted by Gutknecht et al., 24 the bactericidal effect of new wavelengths combination of both 2780 nm Er,Cr:YSGG laser and 940 nm diode laser in prototype dual laser delivered through RFT has been assessed. A high reduction in the bacterial load to 3.5 log steps was reported in 1000 μm specimen thickness, whereas the Er,Cr:YSGG laser could eliminate an average of 99.2% (2.1 log kills) of the E. faecalis bacteria. In this study, the same methodology and fiber design have been adapted; however, a comparable reduction in the bacterial load to 2.22 was achieved using 940 nm diode laser at 1.5 W in CW mode with slice thickness of 1000 μm. The differences in the bacterial reduction could be because of differences in the laser wavelength, output power, and emission mode.
Irrespective of the used wavelength, the beam geometry in the RFT design tends to spread the beam in a broad cone with an angle of 60°. This could improve the distribution of laser emission in the root canal, allowing a more uniform coverage to the whole dentinal wall. Owing to the geometry of the BFT, the laser light tends to propagate in a forward direction, delivering most of the laser energy toward the apex of the root; this could explain the higher temperature elevation in the apical root portion in the bare fiber laser delivery. In addition, an inhomogeneous distribution of the laser light on the canal wall may explain the superior bactericidal effect of the diode laser in conjunction with the RFT laser fiber.
Even though the bare fiber achieved higher temperature than the RFT fiber, the temperature rise recorded during laser irradiation utilizing both tips design did not exceed 3.2°C at the external root surface. This temperature is far lower than the critical threshold temperature of 10°C, 25 which has been described by Eriksson and Albrektsson as unsafe for periapical structure. Therefore, possible damage to the tooth-supporting tissue could be excluded. To simulate the in vivo conditions, polyurethane casting resin has a thermal conductivity of 0.6 W/m K, and a density of 1.4 × 103 kg/m3 was used in this study, in which thermal conductivity of the bone 26 ranges from 0.58 to 1.2 W/m K with a density 27 of 1.3 × 103 kg/m3.
Further investigations regarding the morphological changes of radicular dentin are now inspected for this fiber design, besides, a long-term clinical study should be implemented to confirm the in vivo effectiveness and to assess the efficacy of 940 nm diode laser in conjunction with RFT.
Conclusions
Within the limitation of this in vitro experiment, one could conclude that 940 nm diode laser delivered through BFT and RFT fiber systems tested in this study may be suitable for disinfection of root canals. Radial firing laser tips obtained a satisfactory bactericidal effect up to 1000 μm depth of dentin and can be safely applied if the laser settings and irradiation time remain within the proposed range.
Footnotes
Acknowledgments
The authors thank Beate Melzer-Krick and Patricia Buttler-Bucher from the Department of Conservative Dentistry, Periodontology and Preventive Dentistry, RWTH University Hospital Aachen, for the technical support.
Author Disclosure Statement
No competing financial interests exist.