
Abstract
Introduction
T
Several surveys of current clinical practice in laser therapy have indicated the popularity and apparent efficacy of this approach for the treatment of various causes. 5 In the field of dentistry, the application of LLLT has been described since the 1970s. Because the extraction of third molars includes damage to connective tissue, bone, and masticatory muscles, this model has been widely used to evaluate the effects of LLLT on the inflammatory process. 6 In any event, there has been a limited amount of solid controlled research done using LLLT on human subjects following molar extractions. Some studies have combined a large human patient pool, the use of a good control, and sufficient energy deliverance. It is principally used to relieve pain, reduce inflammation and edema, and to accelerate healing after surgery. 3,7 –14
The purpose of this study is to determine whether either transcutaneous or intraoral LLLT reduces postoperative pain and assists in the healing of mandibular third molar extraction.
Materials and Methods
The subjects of this dual-center study were selected from the Departments of Oral and Maxillofacial Surgery at Gazi University, Ankara, Turkey and Virginia Commonwealth University Medical Center, Richmond, VA. This study protocol followed the Declaration of Helsinki on medical protocol and had been approved by the local ethics committee, and informed written consent was obtained from all the patients.
This randomized, placebo controlled split-mouth design study was conducted on 60 patients (36 female, 24 male), aged 16–35 (21.88 ± 4.32), with full bony impacted, Class II, Class B according to the Pell–Gregory and Winter classification, with similar position mandibular third molars bilaterally. For this study, healthy individuals were defined as individuals with no active infections and no known neurological or neuromuscular disorders. Exclusion criteria were as follows: patients who had severe periodontal disease, acute pericoronitis, local infection or pathology, and participants contraindicated to laser therapy or had systemic disease using corticosteroids or NSAIDs during the previous 3 months. Patients were required to be classified as class I or II by the American Society of Anesthesiology Protocol. General anesthesia or local anesthesia (lidocaine 2% with epinephrine, 2 cc for each quadrant) was administered to the patients. The lasers utilized in this study were the Lumenis (Lumenis, Inc., Santa Clara, CA) gallium aluminum arsenide (GaAlAs) 830 nm diode lasers set at 100 mW for extraoral using and BTL 2000 (Medictinedic, Denmark) GaAlAs 830 nm diode lasers set at 100 mW for intraoral using.
The surgical procedure was standardized using a three-cornered flap followed by a buccal osteotomy, sectioned as needed, elevation of the tooth, and suturing with 4-0 silk sutures. No steroids were administered to the patients pre- or postoperatively. Postoperatively, all patients received amoxicillin 500 mg orally thrice per day for 5 days, chlorhexidine gluconate–benzydamine HCL mouth rinse twice per day for 5 days, and 500 mg acetaminophen orally every 12 h for 3 days. All operations were performed by the same surgeons who used a standardized technique on all patients at the same session for both sides, and the laser applications were administered by a different surgeon for each center to standardize the procedure. As the study was performed in a single-blind manner, patients had not known which treatment was applied in each of the two surgeries. The only different surgeon (not doing surgery) who was to know the treatment performed was the researcher who is responsible for the application of the laser.
The application of laser on the left or right side was chosen randomly, according to a sheet of randomization, and one side treated with laser device to deliver irradiation transcutaneously or intraorally and the other side with the laser emission deactivated in the placebo treatment group. For the patients in the transcutaneous group (n = 30 teeth), the laser handpiece was applied extraorally over the masseter muscle in the third molar region on one side of each patient, while the laser was inserted intraorally over the third molar site for the intraoral LLLT patients. The laser treatment itself consisted of administering the laser energy immediately before and immediately after the extraction procedure. Both applications of the laser lasted for 15 sec (3 J/cm2 of energy, 10.0 Hz, 63 mW), in continuous mode for each application and both lasers. In all respects, the application was identical with respect to time and pressure applied in transcutaneous group with the laser application in all patients. Both the operator and patient wore protective glasses. The study was double-blind in that the patient and clinical assessor (who evaluated the healing and pain) did not know which site had been treated with the laser or placebo. All patients had received postoperative advice verbally and was documented. We advised that they should have a cold or warm soft food diet on the day of surgery. Postoperative pain was measured using a Visual Linear Ranking Scale (1–10 cm). Patients were given a data recording form with a self assessment for pain on the right and left side. Data were recorded each day for 1 week following the extraction. The patients were reviewed on the seventh day following surgery of recovery by measuring the incidence of dry socket or infection by a clinical assessor. This healing was as described by Fernando et al. 15
Data obtained from 53 (26-transcutaneous group, 27-intraoral group) of 60 patients were completed and used in the statistical analysis. Descriptive and bivariate statistics was computed with statistical software (SPSS 15.0), and the p-value was set at 0.05. The Wilcoxon rank test was used to compare pain levels in laser groups with contralateral placebo for each group. The Mann–Whitney U-test was used to explore the differences between pain levels in transcutaneous and intraoral applications.
Results
Neither complications nor complaints were observed during and after surgery. None of the patients showed any adverse reactions to the laser treatment. Seven of 60 patients had incomplete records and were not included in the statistical analysis. The mean values and standard deviations of pain parameters of the groups are shown in Table 1. Data were obtained from each of the 53 patients (106 teeth) for transcutaneous laser (group A: 26); intraoral (Group B: 27) and placebo group (Group C: 53) were paired for analysis. The mean pain level in the intraoral laser group was 2.505 ± 2.92, in the transcutaneous laser group was 3.302 ± 2.97, and in the placebo group was 3.163 ± 2.08. Postoperative VAS scores were analyzed statistically by the Wilcoxon rank test in laser groups with contralateral placebo for the differences in follow-up periods of each group at 5% level of significance. Although there was a statistically significant reduction in pain between the intraoral laser group and the placebo group starting from the first day following surgery (p = 0.001 < 0.05), no statistically significant difference was found in pain levels between the transcutaneous laser group and the placebo group (p = 0.489 > 0.05). The Mann–Whitney U-test was used to explore the differences between pain levels in transcutaneous and intraoral applications. The intraoral LLLT application resulted in a statistically significant reduction in postoperative pain comparison with the transcutaneous laser group (p = 0.001 < 0.05) and the placebo. Graphs of pain levels for each group over time are shown in Fig. 1. The unhealed socket numbers were compared in three groups at seventh day (one unhealed sockets per laser groups, two unhealed sockets in placebo group) and did not observe any differences.
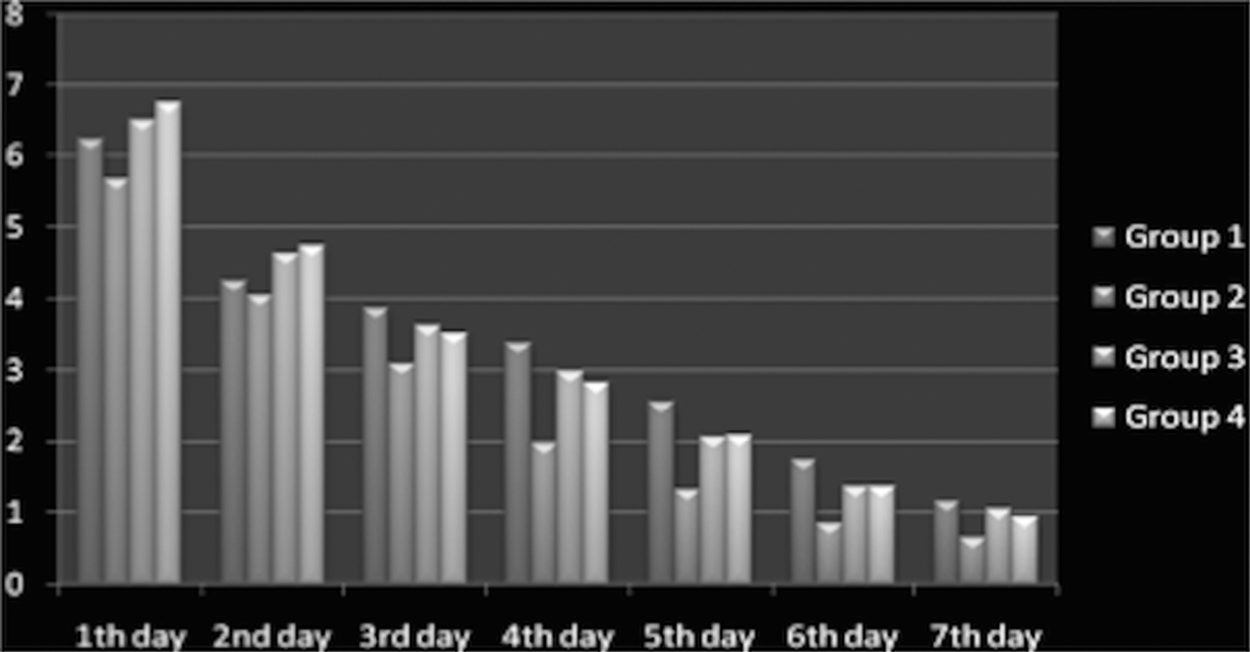
Graphs of pain levels for each group over time. Group 1: Transcutaneous laser; Group 2: Intraoral laser; Group 3: Transcutaneous placebo; Group 4: Intraoral placebo; Group 2–4: p = 0.001 < 0.05; Group 1–3: p = 0.489 > 0.05; and Group 1–2: p = 0.001 < 0.05.
Discussion
LLLT offers a safe therapeutic medical modality that is generally free from side effects. After more than 30 years of use, no harmful side effects have been reported. The FDA has classified the most commonly used LLLTs as class III: no-significant-risk medical devices. The only known potentially toxic effects could be caused by direct exposure of the eyes to the laser beam. 5
There are many types of phototherapy devices with different characteristics, including gallium-arsenide (GaAs), helium–neon (HeNe), and GaAlAs lasers. 16 The GaAlAs diode laser is known to be a high-tissue penetration laser because hemoglobin and water have a low coefficient of absorption for it. The GaAlAs laser, delivered to the skin and oral mucosa, penetrates the tissues and is thought to reach the nerves lying 4–8 mm under the tissue surface. 5 Because of this, the GaAIAs laser has been utilized for the management of the pain for their analgesic and anti-inflammatory effects, increasing pain threshold and biostimulating effects. 16
The primary indications for the use of LLLT after lower third molar surgery are the effects that they may have on wound healing, postoperative pain, and swelling control. A lot of studies have been made to control postoperative pain, such as NSAIDs, long-acting local anesthetics, corticosteroids, ozone, and LLLT. 2,4,6,15,17 –27 NSAIDs are often recommended for postoperative pain, but some of them may manifest side effects such as a tendency to systemic bleeding, gastrointestinal irritation, and allergic reactions. 11,19
Even though the mechanism of pain control and analgesia associated with LLLT is not well understood, an increased pain threshold through the alteration of neuronal stimulation and firing pattern and the inhibition of the medullar reflexes is thought to be involved. 5 This pain-relieving effect might be like transcutaneous electrical nerve stimulation or an acupuncture effect due to laser stimulation of chromophores in the myelin sheaths, stability of nerve cell membrane, and the associated integral proteins of the nerve cell membrane. 5,19 The enhanced redox systems of the cell and an increase in ATP production have been shown to lead to restoration of neuronal membranes and decreasing pain transmission. 19 In addition, LLLT acts on prostaglandin synthesis, increasing the change of prostaglandin G2 (PGG2) and prostaglandin H2 (PGH2) into prostaglandin 12 (PG12). 5 It has been reported that reduction in pain and swelling can be achieved when the operative field is treated with LLLT. 1,2,4,6,7,8,23
The recovery of an extraction wound healing, one of the most studied aspects of LLLT, is a complex process with local and systemic responses and involves several types of cells, enzymes, growth factors, and other substances. It has been hypothesized that this is due to stimulation of fibroblast growth factors. Since fibroblast secretes connective tissue that lines the socket of the molar, this could lead to more rapid healing. 8 This has been shown that depending on the wavelength, dose, and local conditions on soft tissues, it is possible that LLLT effects on wound healing depend not only on the total dose of irradiation but also on the irradiation time and the irradiation mode. 5
Several studies have been done on human subjects showing effects of LLLT on postoperative healing (Table 2). The first study in 1990 reported by Carrillo et al. 21 investigated the efficacy of HeNe laser compared with ibuprofen and placebo in reducing pain, swelling, and trismus following third molar extraction. These investigators found that trismus was significantly less in the laser group, although swelling and pain were the same in treatment groups. In their study, the exposure to the laser was split between the bone and the soft tissue and it was at least 50% greater in time. The effect of laser treatment is likely dose dependent, and it may be that a longer exposure needs to be given, but the time needed to produce a detectable effect on tissues would be unacceptable in clinical practice.
LLLT, low-level laser therapy.
Roynesdal et al. 22 examined the effect of LLLT on pain and swelling after lower third molar surgery in a double-blind crossover study in 25 patients. They found that postoperative trismus, swelling, and pain were not influenced by the application of LLLT compared with the placebo. A study done in 1993 concluded that LLLT neither reduced pain nor stimulated healing. This study included 52 human subjects and delivered the equivalent of 4 J of energy by LLLT immediately following surgery. 15 The results showed no statistically significant differences between the experimental (22 patients) and control group (30 patients). In all studies until 2006, authors found that postoperative swelling and pain were not influenced by the application of LLLT compared with the placebo. This has shown that LLLT effects on postoperative healing depend not only on the total dose of irradiation but also on the laser output power, irradiation time, and the irradiation mode. In this present study, postoperative pain showed differences in intraoral laser group, although wound healing was not influenced, and this result did not support the findings of their study on pain.
Although LLLT has been reported to decrease swelling and trismus after third molar surgery, some of these studies reported a positive effect while others did not. Aras and Güngörmüş 27 compared the effects of extraoral and intraoral Ga-Al-As diode laser device on postoperative trismus and edema following the removal of mandibular third molars. In their study, 48 patients who were to undergo surgical removal of their lower third molars were studied. Patients were divided into three groups: extraoral LLLT (n = 16 teeth), intraoral LLLT (n = 16 teeth), or placebo (n = 16 teeth). Their results demonstrate that extraoral LLLT was more effective than intraoral application. Kazancioglu et al. 23 compared the effect of LLLT and ozone therapy with control group after impacted third molar surgery. They reported that the pain level was lower in the LLLT and ozone groups than control group, although swelling and trismus were significantly lower in the LLLT group. This effect of LLLT depends on the fact that laser light penetrates tissues and tissue fluids. The energy may be absorbed where the concentration of fluid is highest and, thus, absorbed more easily by inflamed and edematous tissue. Another study indicated that postoperative use of LLLT (4 J/cm2) after impacted lower third molar surgery significantly reduces postoperative pain compared with diclofenac in a single dose preoperatively and control group. They explained that this effect is dose dependent, as previous studies point out that output doses of laser energy lower than 4 J/cm2 do not influence the postoperative pain. 19 In this present study, output dose was 3 J/cm2, and postoperative pain was significantly lower in the intraoperative laser group.
Ferrante et al. 1 evaluated the effect of LLLT on postoperative pain, swelling, and trismus. They applied the LLLT both intraorally and extraorally for each patient; they observed that swelling and trismus were significantly less in the laser group than control group, although there was lower pain intensity in laser group but without statistically significant differences. In another study, 13 they examined the effect of extraoral application of LLLT on the pain, trismus, and swelling with 3dMD face system. They reported no statistically significant differences in terms of trismus and swelling levels, but there was significant decrease in the pain level on the seventh day. Eroglu and Keskin Tunc 14 evaluated the effect of single-session extraoral LLLT application on pain, trismus, and swelling after lower third molar surgery in a placebo control study. There were no significant differences, but according to their clinical outcomes, swelling and trismus were less in the laser group than placebo. In another similar study, they observed that single dose laser therapy was effective at reducing the postoperative discomforts. 4 Eshghpour et al. 12 evaluated the effect of three sessions, extraoral and intraoral application, of combined LLLT on pain and swelling after third molar surgery. They found statistically significant pain and swelling level in laser group. Amarillas-Escobar et al., 26 applied LLLT to multiple points in four sessions and, despite not being statistically significant, were in favor of LLLT. According to the results of these studies, researchers should focus on which application is successful because the repetitive sessions cause loss of time for both patient and physicians. 4,14,26
Previous studies have utilized lasers via an extraoral, intraoral, or combination approach. Some of these studies believe that extraoral application is the predominant effective method on swelling and trismus, but effect on pain is still controversial. It was postulated that the penetration differences between skin and mucosa could have effect on the results.
Penetration of diode laser primarily depends on the optical properties of the skin or oral mucosa, which in turn depend on the type and thickness of the epithelium, reflectance, melanin content, and level of vascularization of the submucosa. This ability is related to both the penetrating ability of the diode laser and the distance to the pathologic processes that are to be influenced. The interaction is photochemical in nature; it is dependent on absorption by a tissue chromophore. The absorption likely increases the energy of this chromophore; therefore, its activity is altered in relationship to its environment. Consequently, the metabolism of the cell is changed, affecting tissues and organs. 5
In this present study, we had compared transcutaneous and intraoral laser application effects on postoperative pain depending on skin or oral mucosa penetration differences. Transcutaneous use could be necessitated by the size of some kind of laser device. It could be an important question that using the device transcutaneously or intraorally may have had effects on the results. We observed that LLLT was more effective when it was applied intraorally instead of transcutaneously, although it did not observe any differences in the number of unhealed sockets in two groups at seventh day (one unhealed socket per each group). Because of the data obtained of contralateral third molar extraction at same time, trismus could not be evaluated in this study. Using a large patient population and the contralateral molar as a control provided bases for reliable statistical results in this split-mouth design study. In split-mouth design study, subjects serve as their own control; this design may be more efficient than design at use between subject comparisons. And this design has no carry-across effect. In comparison, the extraoral and intraoral laser was administered pre- and postoperatively, something that has been rarely seen in other studies.
Conclusions and Summary
Many medical scientists doubt the validity of the claims, categorizing LLLT as a fringe medical technique for which there is no convincing evidence. This single-blind, randomized split-mouth study, both transcutaneous and intraoral laser application, was used to examine effects on postoperative pain and healing. The result of this study is that the intraoral using of LLLT is more effective than extraoral application on pain after third molar surgery. It was postulated that the penetration differences between skin and mucosa could have an effect on the results.
Footnotes
Acknowledgment
Supported by Gazi University Scientific Research Projects Fund (Project number: 03/2002-08).
One of the GaAlAs lasers for this project was donated by ESC Medical Systems, Yokneam, Israel.
Author Disclosure Statement
No competing financial interests exist.