
Abstract
Introduction
O
The prevalence of leukoplakia is variable among geographical oral sites and demographic groups and its range in the general population is from <1% to >5%. 9 Its appearance in oral cavity usually takes place after the age of 30 years, resulting in a peak of incidence above the age of 50. 10
Several authors suggest that the risk of malignant transformation is higher in smoker patients. 11,12 The role of Candida albicans as a possible etiological factor in leukoplakia and its possible role in malignant transformation need further investigation, 13 as well as a possible influence of genetic factors in the development of this pathology. 14,15 Further, there are conflicting results of studies related to the possible role of human papilloma virus infection. 15,16
From a histopathological point of view, it is important to distinguish the dysplastic lesion (leukodysplasia) from the nondysplastic one (leukokeratosis). Even if it is generally accepted that the first carries a decisively greater risk of malignant transformation than the second, it should be recognized that some of the dysplastic lesions remain clinically unchanged, whereas carcinomatous transformation may occasionally take place in nondysplastic ones. 10 However, a single, evidence-based, and clinically useful predictor of malignant transformation for dysplastic and nondysplastic leukoplakias is not available at the moment.
Leukoplakias may occur either as a single, localized change of the oral mucosa or as diffuse, often multiple, lesions. Any oral site may be affected.
Clinically, two main different forms are recognized
5,7,8
: (a) Homogeneous leukoplakia: a lesion of a uniform flat appearance that may exhibit superficial irregularities, but with a consistent texture throughout. (b) Nonhomogeneous leukoplakia: a predominantly white or white and red lesion (erosive leukoplakia, erythroleukoplakia) with an irregular texture that may present as a flat, nodular, or verrucous lesion.
Proliferative verrucous leukoplakia (PVL) presents with multiple, simultaneous leukoplakias as the disease is visibly multifocal, frequently covering a wide area. PVL may progress into verrucous or squamous cell carcinoma.
For a nonhomogeneous leukoplakia, the risk of malignant transformation is 23.4–38%; in the presence of epithelial dysplasia, the possibility is 36.3–43%. 9,17
On the basis of the reported annual malignant transformation rate of this disease, the estimation of the annual rate of oral leukoplakia malignant transformation is 1.36% in various populations and geographical areas. 18,19 The patients with oral leukoplakia carry a fivefold higher risk of developing oral cancer than controls. In several studies on malignant transformation, the border of the tongue and the floor of the mouth have been mentioned as so-called high-risk sites, which need more monitoring and care. 18,20
The management of oral leukoplakia includes various treatment modalities with a low success rate at long follow-up: surgical treatment, medical therapy, and nonsurgical treatments [vitamin A and retinoid, beta carotene or carotenoids, nonsteroidal anti-inflammatory drugs (NSAIDs), herbal extracts, including tea components, a Chinese herbal mixture and freeze-dried black raspberry gel, bleomycin, and Bowman–Birk inhibitor]. 21
The conventional types of surgical treatments are done by scalpel excision, electrosurgery, and cryosurgery. The recurrence rate varies for scalpel excision from 10% to 34% and for cryosurgery from 12% to 25%. These modalities cause tissue scarring and contraction, and they can mask early signs of recurrence. 6,7
The use of laser for surgical treatment of leukoplakia was reported. 22 Different laser wavelengths were proposed: CO2, 23 –27 Nd:YAG, 28 Er:YAG, 29 and diode. 30 The laser beam can superficially remove the soft tissues by evaporation with minimal thermal damage to adjacent tissue, which results in minimal tendency to scar and little postoperative pain and edema. 31 The surgical procedures and their success rates are different and multiple.
However, a gold standard surgical protocol for the treatment of leukoplakias by laser beam is still needed to improve the success rate of our treatments.
The aim of our study is to evaluate the long-term success rate of oral leukoplakia treatments using different laser-supported surgical protocols.
Patients and Methods
Preoperative observations
Two thousand three hundred forty-seven lesions of oral leukoplakias in 1282 patients (845 men and 437 women; age range: 40–82 years) affected by oral homogeneous leukoplakia were treated and evaluated. A detailed clinic evaluation of each patient was recorded at the first oral examination. Overall, 511 patients had a lesion at a single site and 771 patients had multiple isolated 0 lesions (Table 1). The lesions were localized on different parts of the mouth: tongue, alveolar rides, palate, on the gum, and on the floor of the mouth (Table 2).
Diagnosis of homogenous leukoplakia was established after exclusion of clinical etiologies and/or histopathologically definable white lesions.
Subclassified into “high risk,” including the floor of the mouth, lateral borders of the tongue, and soft palate.
Diagnosis of leukoplakia was established after exclusion of clinical etiologies and/or histopathologically definable white lesions.
Diagnostic procedures
At the first visit, each patient affected by white oral lesion was examined to exclude lesions with evidence of etiological factors to orientate the diagnosis of “true leukoplakia” or other diseases or conditions. The clinical diagnosis of the lesions was based on the criteria adopted by the WHO, and the histopathological diagnosis of epithelial dysplasia was established according to the WHO definitions.
We respected the protocol proposed by Warnakulasuriya et al. 5 for the differential diagnosis (Table 3).
Warnakulasuriya et al. 5
The management of oral white lesions respected the procedure proposed by Van der Waal et al. 32 (Fig. 1).
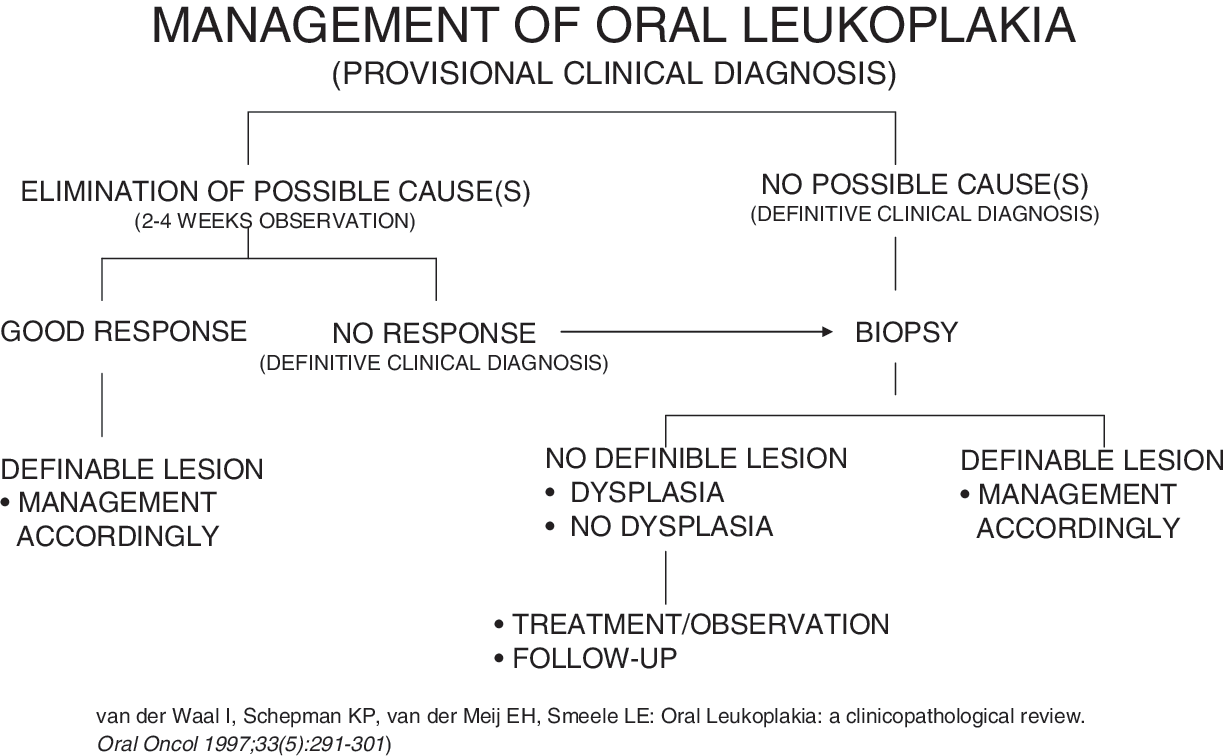
Schema representing the management of oral leukoplakias.
We collected information for establishing a differential diagnosis to classify lesions as “homogeneous”or “nonhomogeneous.” We identified some etiological factors such as a family history of similar lesions (white sponge nevus, hereditary benign intraepithelial dyskeratosis), duration of the process (to exclude geographic tongue consisting of a temporary process of dekeratinization and hyperkeratinization), and identification of oral habits such as cheek or lips biting (cheilophagia) and parafunctions (bruxism). Dermatological disorders were evaluated to find some oral mucosal manifestations. Tobacco consumption (type and frequency) was considered to recognize the typical lesions of nicotine stomatitis. A careful history and clinical examination should indicate the nature of reactive lesions (aspirin burns and frictional hyperkeratosis). The hyperkeratosis of the tissue represents the protective response to low-grade long-term trauma. Some white oral lesions where diagnosed when they exhibited clinical or histopathological findings that were typical for specific different diseases (lichen planus).
Laboratory data (including serologic, hematologic or microbiologic information) were collected as evidence of systemic diseases or infections that were potentially related with white lesions (HIV, HCV positivity) and candida sur-infection.
Subsequent to clinical examination when it was possible to identify some suspected etiological factors, these elements were eliminated and, in the case of persistent lesion after 4–8 weeks, biopsies for histological examination were performed.
When white lesions were detected to be in contact with amalgam or other metallic restoration (galvanic keratosis), we advised patients to replace the dental metallic fillings.
In small and homogeneous lesions, a biopsy was performed, including a margin of apparently normal tissue, whereas in nonhomogeneous forms or in multiple leukoplakias, a map biopsy was made to detect epithelial connective alterations at every site of altered tissue. In mixed red-and-white lesions, a simple or map biopsy was performed after the identification of the most suspicious areas through the use of toluidine blue.
Leukoplakias, even clinically similar, may display a wide range of histological appearance. The presence of epithelial dysplasia may be predictive of a transformation to oral cancer, and the risk of cancer occurrence is likely to increase with the increasing of the severity of dysplastic changes. Leukoplakias are not a morbid or lethal disease and they do not have a relatively high risk of malignant transformation. 7,21 The lesions are classified according to location and clinical appearance.
Exclusion and inclusion criteria
To allow a possible evaluation of surgical protocols and to reduce variables, only diagnosed homogenous oral leukoplakias were reported in this study. Nonhomogeneous leukoplakias and lesions with dysplasia or malignancy in situ were excluded. We classified the location sites of leukoplakia into two subclassifications: high-risk and low-risk sites related to their potential risk of malignant transformation. The lesions were subclassified as high-risk lesions affecting oral locations (the floor of the mouth, lateral borders of the tongue, and soft palate), and lesions located under removable dentures and subjected to continuous friction were only recorded in our study. The lesions subclassified as low-risk lesions, including gums, hard palate, dorsum of the tongue and cheek mucosa, were only monitored. Some leukoplakias subclassified as low risk may regress in time or disappear in patients who had no treatment. 32 The lesions having a dysplasia or malignancy were excluded from the study.
Only leukoplakias located in the oral cavity were considered. All selected patients were healthy. We excluded risky cases of patients from our study. No medications were prescribed before surgeries.
According to the ethics committee recommendations of our university hospitals, the decisions for surgery were made after informing patients about the different steps of each surgery, risks, and expected postoperative discomforts, and surgery was performed only after receiving the consent of the patient.
Surgical protocols
Several criteria were respected. Anesthesia was administrated by local infiltration covering the area of the lesion and a minimum of 5 mm of surrounding healthy tissues.
A carbon dioxide (CO2) laser machine (10.6 μm: Smart US20 D Laser 10,600 nm; High Tech Laser, Herzele, Belgium) was used. The parameters of irradiation were as follows: output power of 3–8 W in focus and in noncontact mode. The distance between the laser handpiece and the tissular impact point respected the focal distance of the manufacturer: 10 mm. The beam diameter was 0.3 mm. The delivered power density was from 42.44 to 113.17 W/cm2. The treatment was almost the same for all patients. All surgeries were done under local anesthesia (articaine with vasoconstrictors). Appropriate safety regulations for the use of lasers were respected by all medical staff and patients by wearing adapted protective eyewear to protect eyes against CO2 laser beam (protective glasses).
Overall, 2347 diagnosed homogeneous oral leukoplakias (Table 2) were treated with CO2 laser and were included in this study. Different surgical protocols (P) were used: (1) P1 (SV = superficial scanning): this was a complete superficial vaporization of the leukoplakia by a scanning mode with an overlapping in two passages. Only the visible white area was treated in one surgical session independently of the lesion size. (2) P2 (CR1x1): this was a complete removal of the lesions, preferentially by excision, until a tissular depth of 1 mm and 1 mm of surrounding healthy-like tissue were attained. The visible white area was treated in one surgical session independently of the lesion size. (3) P3 (CR1x3): this was a complete removal of the lesions, preferentially by excision, until a tissular depth of 1 mm and 3 mm of surrounding healthy-like tissue were attained. The visible white area was treated in one surgical session independently of the lesion size (Fig. 2). (4) P4 (PR1x3): this was similar to the protocol P3, but for patient comfort and to allow patients to continue their normal life, the large involved leukoplakias (lesion size greater than 20 mm) were excised in several surgical sessions. The complete surgical excision of the leukoplakia was performed in multiple sessions spaced by 1 month (partial surgical removal of 10 mm per session).
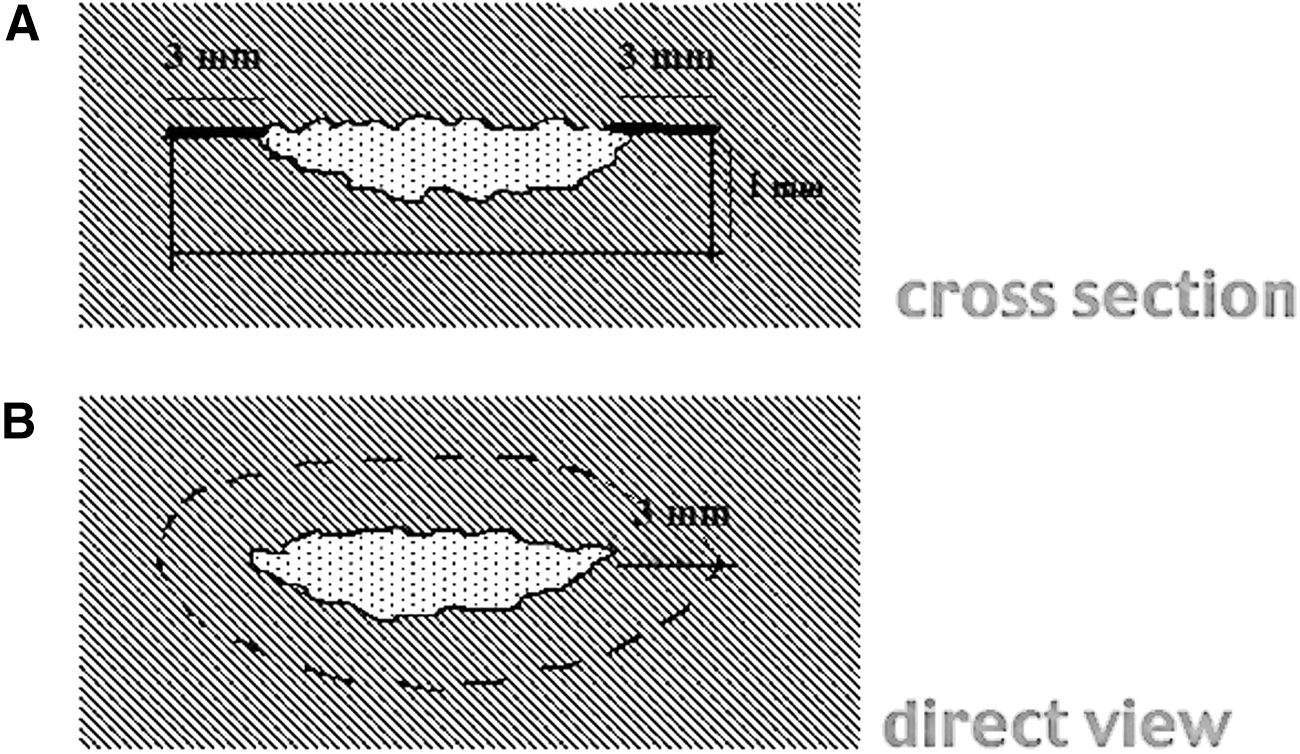
Schema showing the surgical protocol respected in protocol 3.
When needed, a biopsy was done in the surgical site once a year during the follow-up period. The control consisted of checking the nature and the aspect of the healed mucosa to exclude an eventual recurrence of the leukoplakia.
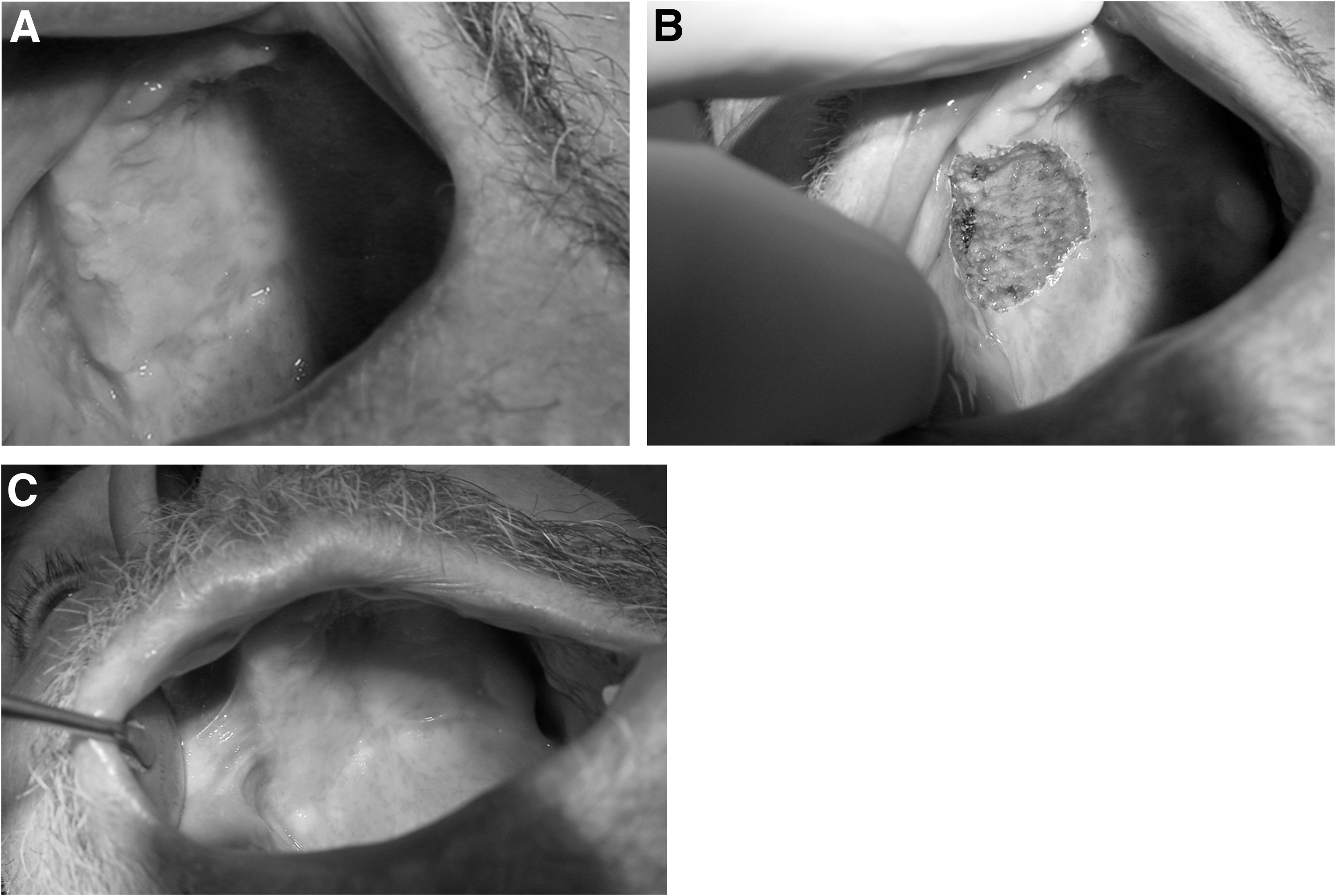
The surgical procedures for the protocols P2, P3, and P4 respected the following: – Excision of the entire part of the lesion in one session (except for the protocol P4) until a minimum tissular depth of 1 mm was attained. The ablation of the lesion involved a minimum of 1 mm of surrounding healthy-like tissues for the protocol 2 and 3 mm as a minimum for the protocols 3 (Fig. 2) and 4 to be attained. – In case of the treatment of multiple lesions in one site and when the distance between two lesions was ≤6 mm, the lesions were considered and treated as one (Fig. 3). The complete treatment in one surgical session was done in the protocols 2 and 3. – Vaporization of the surgical site to harmonize the depth and to allow complementary hemostatic effect. – A Lotagen® solution (meta cresol-sulfonic acid and formaldehyde in concentrated solution) was used to remove the carbonization from the surgical site. – The bottom of the wound was examined visually to detect the presence of eventual abnormalities in the connective tissues (white or gray colored). After the visual inspection or after removal of eventual abnormalities, the bottom of the wound should be soft with a normal appearance. – No sutures were used (Figs. 4A, B and 5A, B), and the wound healed by secondary intention. – Oral disinfecting solution was prescribed to be used three to five times a day during 10 days with the aim of avoiding a wound secondary infection. – The wound was left without any make up. – In case the dimension of the wound was >2 cm, an antibiotic was prescribed for 8–10 days. Analgesics coupled to anti-inflammatory drugs were also prescribed.
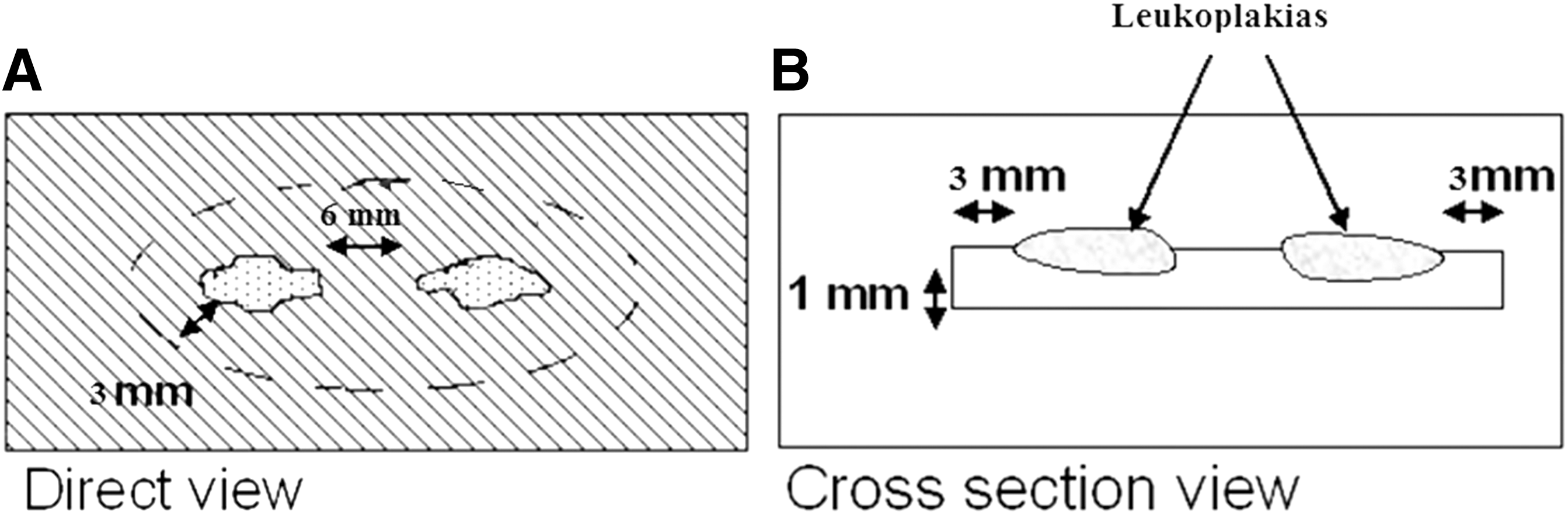
Schema showing the procedure to treat close lesions in the protocol 3.
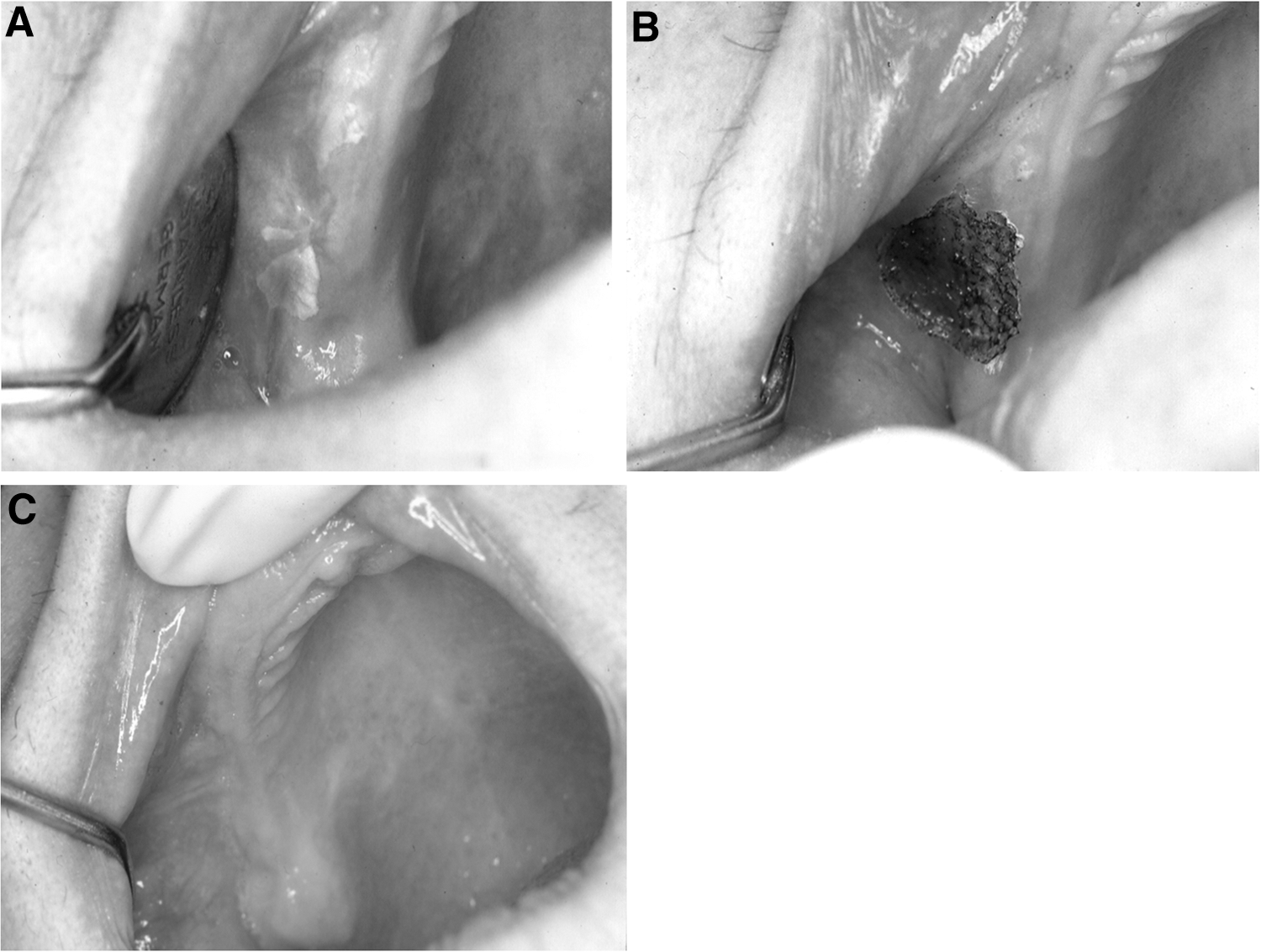
Multiple oral leukoplakias affected the maxillary crest and a part of the vestibule
The leukoplakia, under a denture, affected the posterior part of the palate
These steps were used for healthy patients. For risky cases, an adapted and specific treatment was administrated.
Follow-up
Believing that malignant transformation cannot be excluded by any of the treatment modalities described earlier (P1–P4), we respected a severe control during the follow-up period.
All patients were recalled at 2 and 8 weeks after surgery, and then every 2 months during the first year, every 4 months during the second year, and once a year for the follow-up period of 6 years. The control dealt with the nature and the aspect of the treated mucosa to exclude recurrences or early signs of oral malignancy.
The chronology of the study was started as follows. In 1986, we started the surgical protocol 1 (P1: SV) and in 1990, we started the protocol 2 (CR 1 × 1). Whereas in 1994, we started the protocols 3 and 4. A long-term follow-up of a minimum of 6 years (range of 6 up to 26 years) was respected.
The data from different treatments were collected and analyzed. Statistical analysis of different results was done.
Results
The one-way analysis of variance statistical analysis coupled to the Newman–Keuls multiple comparison post-test showed that the averages of all groups are significantly different (p < 0.0001; F: 26,350 and R 2: 0.9712). Thus, we can affirm that the averages of success rates in all groups are significantly different.
The results of different protocols followed on 2347 lesions of leukoplakias pointed out a Global percentage of success of 5.7% for the first protocol (P SV), 69.7% for the second protocol (CR 1 × 1), and 71.9% for the fourth protocol (PR 1 × 3) (Fig. 6). The third protocol, consisting of a complete excision of lesions in one surgical session and respecting the ablation of a minimum of 1 mm in tissular depth and 3 mm of healthy-like surrounding tissue (group CR1x3), had the highest percentage success rate of 97.8% (Fig. 6). The percentages of recurrence and reappearance of leukoplakias in treated sites were 94.3% for protocol one (P SV), 30.3% for the second, 2.2% for the third, and 28.1% for the fourth protocol (Table 4).
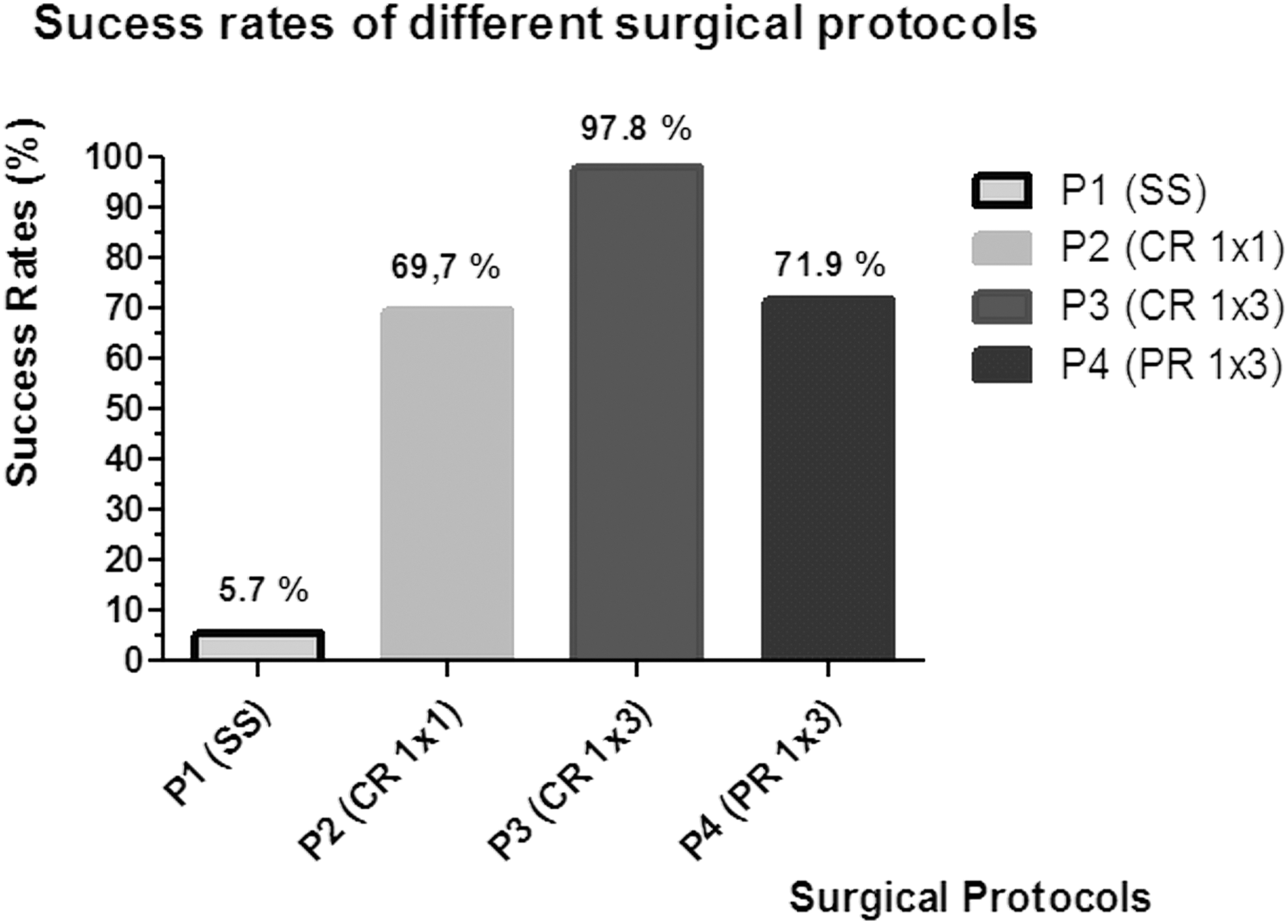
The different rates of success are shown for each surgical protocol.
The complete removal of the lesion was made in one surgical intervention.
The complete excision of large lesions was treated in several sessions of surgical interventions.
During the follow-up period, the number and the rate of the appearance of dysplasia in treated patients were 9 and 26% of treated cases by the first protocol (P SV), 6 and 1.2% for the second protocol (CR 1 × 1), and 2 (0.32%) for the fourth protocol (Table 4).
During the follow-up period, the appearance of malignant transformation after laser treatment was 20%, 1%, and 0.2%, respectively, for the groups treated by the protocols: 1 (SV), 2 (CR 1 × 1), and 4 (PR 1 × 3). On the contrary, the appearance of malignant transformation in failed treated cases (recurrences and reappearance of leukoplakia) was 21.21% for the protocol 1 (SV), 3% for the protocol 2 (CR 1 × 1), and 0.6% for the protocol 4 (PR 1 × 3).
Only in the third group CR1x3, no dysplasia or malignant transformation was noted during the follow-up period of 6 years (Table 4).
Figures 4C and 5C showed the healing aspect of operated sites after the use of the protocols 4 (PR 1 × 3) and 3 (CR 1 × 3), respectively. The healing of tissue after laser surgery was excellent and satisfactory.
Discussion
Leukoplakia monitoring shows that the lesion may regress unpredictably, may remain stable, or may progress to carcinoma. The primary treatment of oral leukoplakia focuses on the suppression of associated etiological factors (smoking, local irritating factors, etc.). 33 In case of persistence of the hyperkeratosis, an oral biopsy is necessary. As oral leukoplakia is potentially malignant and as some leukoplakias will unpredictably progress to carcinoma, oral leukoplakias should be treated. 21,34 The prevalence of leukoplakia in the general population varies from <1% to >5%. 10 Moreover, the natural annual limit of oral leukoplakia malignant transformation rate is unlikely to exceed 1%. 19 Nonhomogeneous leukoplakias carry a higher degree of risk of malignant transformation when compared with the homogeneous variants. 35
Regarding nonsurgical treatments (retinoid, bleomycin, local use of corticosteroid, etc.), the available evidence on medical and complementary interventions for treated leukoplakias is very limited. The relapses and adverse effects are common. 36 The recurrence of oral leukoplakias after surgical treatment has been reported in 10–35% of cases. 37 Further, Kuribayashi et al. 38 observed a long-term outcome (10 years) of nonsurgical procedure treatment of oral leukoplakias. Their results indicated that on 237 observed lesions, 135 lesions (57.0%) remained unchanged, 30 (12.7%) lesions were characterized by a reduction in size or clinical severity, and 44 (18.6%) lesions had disappeared. Another 11 (4.6%) lesions developed oral squamous cell carcinoma. 38 In their conclusion, the authors indicated that the development of appropriate treatments for oral leukoplakia is required, which will enable successful differentiation between surgical and observation cases. 38 Those results show the necessity to device a more efficient prophylactic and acceptable permanent therapy for patients. In an observational retrospective study published by Schepman et al., 39 they compared the incidence of squamous cell carcinomas in two groups of subjects with oral leukoplakia: one comprising patients received some active treatments (medical and/or surgical) and the other involving patients kept under clinical follow-up. No significant difference was observed in the risk of malignant transformation between the two groups. These results perhaps suggested that the natural history of oral leukoplakias might be independent of the treatment received and that there is a subgroup of lesions destined to undergo malignant transformation regardless of the therapeutic strategy adopted. The recurrence rate varies for excision from 10% to 34% and for cryosurgery from 12% to 25%. These modalities cause scarring, contraction, and can mask early signs of recurrence. 9
The advantages of the use of oral laser surgery, when compared with other modalities of treatment, are the minimal postoperative edema, little postoperative scarring, minimal postoperative pain, reduced risk of secondary infections of the wound, 40 and based on our results, lower recurrence rates. Another advantage of the CO2 laser in comparison with the cold surgical blade is the control of bleeding by thermal coagulation, which allows operators to observe the presence of eventual tissue abnormalities (white/gray appearance involving connective tissues) still remaining after the removal of carbonized areas. In this case, the abnormalities can be easily localized and removed by vaporization. 40
The newly formed epithelium appeared normal and was soft on palpation. 25 We observed similar results in our study. The re-epithelialization was complete after 2–4 weeks depending on the lesion size and location. We also observed a minimal scar formation and no subsequent interference with normal lip function. CO2 laser excision permits the possibility of removing the entire lesion with acceptable readability of the surgical margins. The morbidity, wound contraction, and impairment of functions due to scar formation and anatomic distortion were reduced because of the physical properties of beam energy and its biomodulation activity involved in the healing process. The use of CO2 laser reduced the recurrence rate and malignant transformation in the protocol 3 (CR 1 × 3) and also the postoperative dysfunction in comparison to the literature. 22,24,26,41,42
van der Hem et al. 43 indicated that after a long-term follow-up study, the CO2 laser can devise an acceptable prophylactic treatment. In a follow-up period of 1–219 months (mean 52), 251 treated leukoplakias (89.0%) did not show a recurrence. Recurrences were observed in 5–168 months after treatment. Three (1.1%) squamous cell carcinomas occurred in the treated area 7, 17, and 19 months, respectively, after CO2 laser evaporation.
Our study has a similarity to previous studies published by Kuribayashi et al. 44 and by López-Jornet and Camacho-Alonso; 31 our surgical protocols (P2–P4) included the necessity to excise a safety margin of surrounding healthy-like tissue to guarantee a higher successful clinical outcome by reducing all epithelial abnormalities during the surgical procedure. The results of the study by Kuribayashi et al. 44 indicated that the recurrence rate after curative surgical resection was 15.1%, with the most common site being the gingiva. 44 Malignant transformation occurred in a single patient (1.9%). Minimal resection margins (<3 mm) were observed in many patients with recurrent disease, and recurrence was more likely in cases with positive margins (epithelial abnormalities at the resection margins) than in those with negative margins. There was no significant association between recurrence and the degree of epithelial dysplasia. 44 The importance of the minimal resection margins of 3 mm may explain the high success rate of our protocol 3 (CR 1 × 3) and the low success rate of the protocol 1 and 2, in which the minimal resection margin of 3 mm was not respected. 45,46 On the contrary, the low success rate of the protocol 4 (PR 1 × 3; partial removal of leukoplakia per session) may probably be explained by the tissular healing process, by secondary intention, inducing a centripetal regeneration of all margins of the wound, including the ill parts invaded by the leukoplakia. The healed area newly regenerated may be inseminated again by leukoplakia mucosa cells. Future studies can provide more information about this hypothesis.
The literature is rich in studies treating the nonhomogeneous leukoplakia. For that reason, we decided to limit our study to the treatments of homogeneous leukoplakias. Knowing that the need for a gold standard protocol to treat this kind of lesion is necessary, we compared different common proposed protocols to point out the best one that can offer a high success rate of permanent healing.
Conclusions
The results of this long-term follow-up of patients treated with CO2 laser for oral homogeneous leukoplakias pointed out that the surgical protocol respecting the complete excision of leukoplakias, in one session, by the removal of a minimum of 1 mm lesion tissue depth and 3 mm of surrounding healthy-like tissues (CR 1 × 3) offers significantly the highest success rate.
Footnotes
Author Disclosure Statement
The authors declare that there is no conflict of interests regarding the publication of this article.