
Abstract
Introduction
T
Removal of the SL is usually performed by various endodontic irrigations. 7,8 The commonly used irrigants are sodium hypochlorite (NaOCl) and ethylenediamine tetraacetic acid (EDTA). 9,10 NaOCl can remove the organic portion of the SL, and EDTA removes the inorganic portion. However, NaOCl irrigation, EDTA irrigation, or a combined irrigation with NaOCl and EDTA have low efficacies of SL removal at the apical third of a root canal, although they may effectively remove SL at the coronal and middle thirds of the canals. 11,12 This is because the canal is a kind of closed-end channel, which may cause gas entrainment and, as a result, produce a vapor lock effect during irrigant delivery. The apical vapor lock effect has an adverse effect on debridement efficacy. 13
Several techniques have been introduced to enhance the ability of irrigants to remove SL, including the passive ultrasonic irrigation (PUI), an endo activator (EA) system, and an endo vac (EV) system. 14,15 However, these techniques have their drawbacks. For example, the PUI may cause a canal deviation, apical zipping, and even root perforation. 16 The EV system cannot completely remove SL at the apical third. 17 In addition, needle or tips of the techniques need to be placed to ∼1–2 mm shorter than the working length. This may limit their applications in canals of various shapes, such as those that have a pronounced curvature.
Laser systems have been proposed as an adjuvant to conventional chemo-mechanical protocols of endodontic treatment to enhance debridement and disinfection. 18 Studies have shown that laser-activated irrigations (LAI) greatly enhanced the effect of irrigation solutions in removing SL by facilitating the penetration of irrigants to deep dentinal tubules and reaching the apical third of the canals. 19 –22 However, these studies focused mainly on the technique using LAI+EDTA, 14,23,24 and no study has reported the effects of LAI with NaOCl and EDTA (LAI+NaOCl+EDTA) on SL removal.
Therefore, the aim of this study was to investigate the effectiveness of LAI+NaOCl+EDTA on the removal of SL in extracted human root canals. Two laser systems were evaluated, including the Erbium: Yttrium Aluminum Garnet (Er:YAG) and the Erbium Chromium: Yttrium Scandium Gallium Garnet (Er,Cr:YSGG) laser. We hypothesized that the LAI+NaOCl+EDTA would be effective for SL removal from the entire root canal wall.
Materials and Methods
Tooth collection
One hundred permanent human mandibular premolars with straight root canals were selected radiologically from the School of Stomatology, Fourth Military Medical University, China. These teeth were caries free, intact, single rooted, and freshly extracted for orthodontic treatment. Those teeth with external or internal root resorption, calcification, or previous root canal treatment were excluded. The experimental protocol was approved by the ethics committee of the Institutional Review Board of the university, and written informed consent was obtained from the donors.
SL generation
After being stored and sterilized in NaOCl (0.5%; Sigma-Aldrich Co., St. Louis, MO) for 24 h, the selected teeth were decoronated to a standard 12-mm root segment at the cementoenamel junction by using a low-speed diamond disk (Struers, Ballerup, Denmark) at 700 rpm under water-cooling conditions. Root canals were first negotiated and instrumented to a No. 10 K-file (Dentsplay Maillefer, Ballaigues, Switzerland). The #10 K-file was inserted into the root canal until it was visible at the apical foramen, and the distance from the orifice to the apical foramen was measured (M mm). The working length was equal to (M − 1) mm. They were then prepared with sequential M3 nickel-titanium rotary instruments (#19/.02, #20/.04, #25/.04, #25/.06, and #35/.04; YiRui, China) to the working length by using a crown-down technique. The 0.5% NaOCl (5 mL) irrigation was adopted during the instrumentation by using a syringe with a 27G side-vented needle (Patterson Dental Supply, St. Paul, MN). The needle was first placed to 1 mm short of the working length and was then moved back and forth.
Grouping and treatments
The specimens were randomly divided into 10 groups (n = 10), and each group individually received one treatment as follows: (A) untreated group: 10 canals were left untreated. (B) NaOCl group: 10 canals were irrigated with 5.25% NaOCl (5 mL; Sigma-Aldrich) for 60 sec. (C) EDTA group: 10 canals were irrigated with 17% EDTA (5 mL; Sigma-Aldrich) for 60 sec. (D) NaOCl+EDTA group: 10 canals were irrigated with 5.25% NaOCl (2.5 mL) and 17% EDTA (2.5 mL) for 30 sec each. Between the irrigations, the canals were dried with paper points (Anhua Medical Technology Co., Ltd., Guangzhou, China) for 30 sec. (E) LAI+NaOCl groups (a total of two groups): 10 canals in each group were individually treated with 5.25% NaOCl (5 mL) activated by the Er:YAG laser (Fotona M021-3AF/3, Ljubljana, Slovenia) or Er,Cr:YSGG laser (Biolase, Irvine, CA) for 60 sec. (F) LAI+EDTA groups (a total of two groups): 10 canals in each group were individually treated with 17% EDTA (5 mL) activated by the Er:YAG or Er,Cr:YSGG lasers for 60 sec. (G) LAI+NaOCl+EDTA groups (a total of two groups): 10 canals in each group were individually treated with 5.25% NaOCl (2.5 mL) and 17% EDTA (2.5 mL) for 30 sec each by activating with the Er:YAG laser or the Er,Cr:YSGG laser.
For groups B, C, and D, the irrigants were delivered by using a syringe with a 27G side-vented needle (Patterson Dental Supply). The needle was first placed to 1 mm short of the working length, and it was then moved back and forth. For the LAI groups (groups E, F, and G), instructions of laser radiations are detailed in Table 1. In brief, the Er:YAG laser emitted a wavelength of 2940 nm, and it was activated at 20 mJ, 15 Hz, 0.3 W, and the super-short pulse mode with 50 μs. A photon-induced photoacoustic streaming tip (9 mm in length; Fotona) with a diameter of 600 μm was used, and the fiber tip was placed and activated at 1 mm below the orifice of the canal. The Er,Cr:YSGG laser emitted a wavelength of 2780 nm, and it was activated at 25 mJ, 50 Hz, 1.25 W, 24% air, a pulse duration of 60 μs, and with the water spray of the laser closed. Two conical fiber tips, RFT2 and RFT3, were used. The RFT2 (diameter = 275 μm, 21 mm in length) was used for the apical third, and the RFT3 (diameter = 415 μm, 17 mm in length) was used for the coronal and middle thirds. The RFT2 was first introduced into the canal parallel to the root canal wall to 1 mm shorter than the working length, and then it was changed with the RFT3. The fiber tips were pulled out parallel to the root canal wall back to the orifice at a speed of 1 mm/s and for five cycles in total. For the treatments with NaOCl, EDTA, and NaOCl+EDTA, all canals were irrigated with 10 mL of distilled water to deactivate the residual NaOCl and EDTA. In addition, at the end of each irrigation, the canals were dried with paper points for 30 sec.
H, pulse mode; Er:YAG, Erbium:Yttrium Aluminum Garnet; Er,Cr:YSGG, Erbium Chromium:Yttrium Scandium Gallium Garnet; PIPS, photon-induced photoacoustic streaming; RFT, radial fining tip; SSP, super-short pulse.
Examination of the SL removal
Longitudinal grooves were carved onto the mesial and distal root surfaces by using high-speed diamond burs (Brasseler, Savannah, GA), without entering the inner parts of the canals. They were split into two parts with an acuminate chisel and hammer. They were then dehydrated with ethyl alcohol (30%, 50%, 70%, 80%, 90%, and 100% for 10 min each), dried in a desiccator for 24 h, sputter-coated with platinum, and observed under scanning electron microscopy (SEM) (S-4800; Hitachi, Japan). For each specimen (12 mm in length), the canal was divided into the coronal, middle, and apical thirds with equal lengths of 4 mm. For each third, four microscopic fields were taken every 1 mm from the coronal end to the apical end at a magnification of 1000 × . A total of 40 (4 × 10) images from the coronal, middle, and apical thirds of the canals, respectively, were obtained for each group.
Three examiners (kappa value = 0.823) were involved in the image analysis. They were all specialists in endodontics and were blinded to the grouping of the study. The scoring of the SL was done according to the previous criteria, as follows 8 : (Score 1): no SL and dentinal tubules open. (Score 2): small amounts of scattered SL and dentinal tubules open. (Score 3): thin SL and dentinal tubules partially open. (Score 4): partial covering with a thick SL. (Score 5): total covering with a thick SL. Scores of all SEM images were recorded and averaged.
Statistical analysis
The SPSS statistics package for IBM (version 19.0; IBM SPSS, Inc., Chicago, IL) was used for the statistical analyses. The conformance among the three examiners regarding the scoring of SL was evaluated with Cohen's kappa test. For multi-group comparison, the Kruskal–Wallis nonparametric analysis of variance and the Mann–Whitney U test were applied. The statistical significance level was set at α = 0.05.
Results
As shown in Fig. 1, representative SEM images were acquired from the middle buccal surface of the canals. The entire root canal wall of the untreated canals was covered with a thick SL (Fig. 1A). After treatment with NaOCl alone, the entire root canal wall was still covered with homogenous SL, and almost no dentinal tubules were open (Fig. 1B). As compared with NaOCl alone, EDTA alone removed more SL at the coronal and middle thirds of the canals, and more dentinal tubules were open (Fig. 1C1, C2). However, the apical thirds were left unaffected (Fig. 1C3). After treatments with NaOCl+EDTA and LAI+NaOCl, a small amount of scattered, thin, and even thick SL could be observed at the coronal, middle, and apical thirds of the canals, respectively (Fig. 1D–F). In addition, the canals treated with LAI+NaOCl showed a rough (the Er:YAG laser, Fig. 1E) or scaly (the Er,Cr:YSGG laser, Fig. 1F) root canal wall. The LAI+EDTA and LAI+NaOCl+EDTA were the most effective treatments. However, the root canal walls treated with the LAI+NaOCl+EDTA (Fig. 1I, J) showed a shallow fossa-like surface, which was much smoother and more consecutive than that treated with the LAI+EDTA (Fig. 1G, H). Within canals treated with the LAI+NaOCl+EDTA, almost no SL was observed at the coronal and middle thirds of the canals, and all dentinal tubules were open (Fig. 1I1, I2, J1, J2). In addition, only a small number of dentinal tubules were partially open at the apical third of the canals (Fig. 1I3, J3). No obvious difference in SL removal was observed between the Er:YAG laser activation and the Er,Cr:YSGG laser activation in NaOCl, EDTA, or NaOCl+EDTA irrigations, except for the morphological differences of the root canal surfaces.
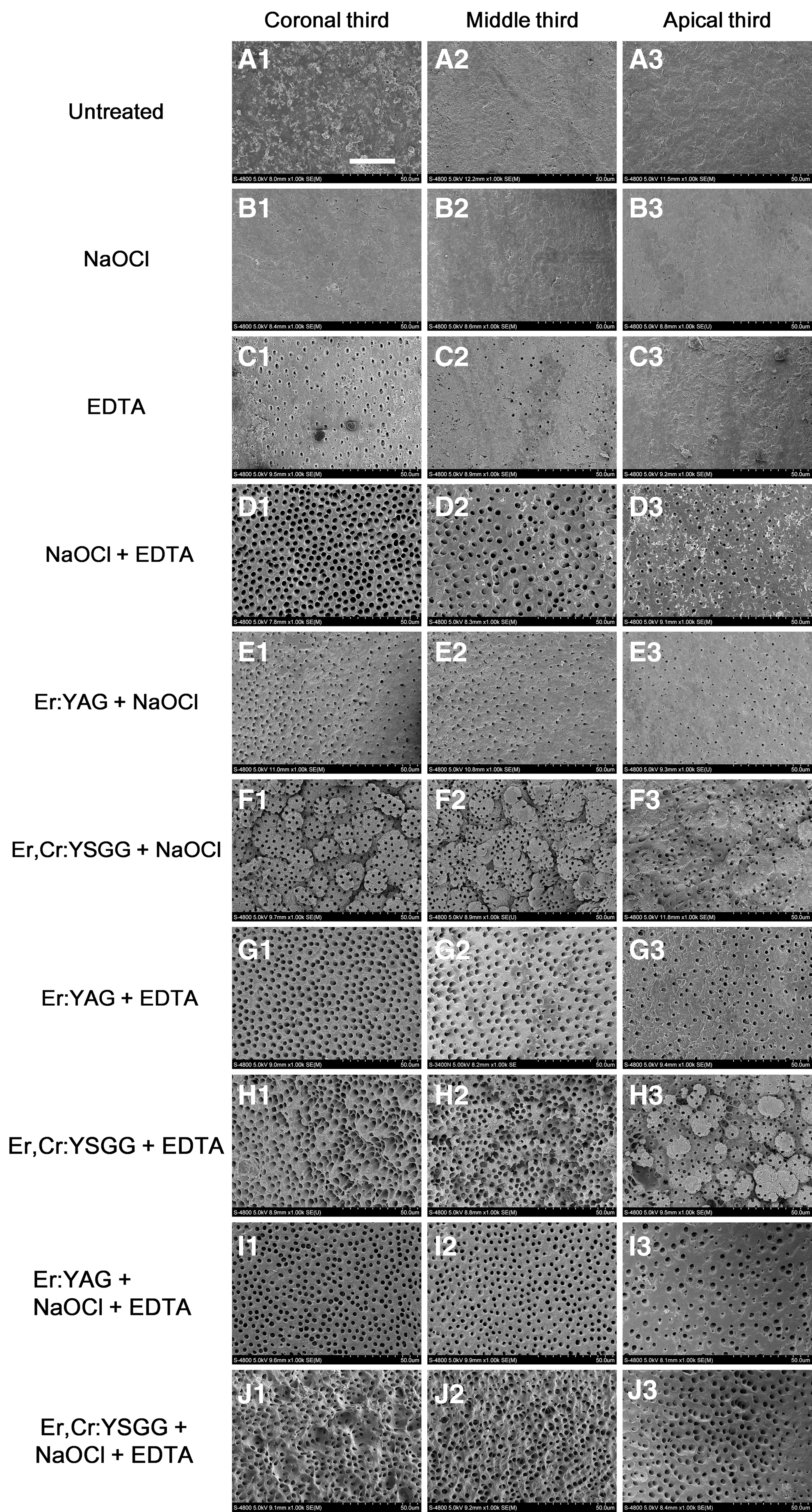
Representative SEM images of the root canal wall after different treatments. Coronal, Middle, and Apical represent the coronal, middle, and apical third of the root canals. A represents the root canals that received no treatment. B–J represent the root canals treated with NaOCl, EDTA, NaOCl+EDTA, Er:YAG+NaOCl, Er,Cr:YSGG+NaOCl, Er:YAG+EDTA, Er,Cr:YSGG+EDTA, Er:YAG+NaOCl+EDTA, Er,Cr:YSGG+NaOCl+EDTA. Scale bar = 30 μm. SEM, scanning electron microscopy.
The frequency distribution of SL scores is presented in Table 2, and SL scores in different groups are presented in Table 3. In the untreated group, the scores were 4.9, 5.0, and 5.0 at the coronal, middle, and apical third of the canals, respectively. After treatment with NaOCl or EDTA alone, the scores significantly decreased compared with those in the untreated group (p < 0.05). However, scores were still more than 3.0 at each third of the canals. In addition, at each third, scores in the NaOCl+EDTA, LAI+NaOCl, LAI+EDTA, and LAI+NaOCl+EDTA groups were significantly lower than those in the untreated, NaOCl-alone, and EDTA-alone groups (p < 0.05). The LAI+NaOCl+EDTA showed the greatest effect on SL removal from the entire root canal wall. The efficacies of SL removal were in a descending order of LAI+NaOCl+EDTA, LAI+EDTA>LAI+NaOCl, NaOCl+EDTA>EDTA>NaOCl.
Coronal, Middle, and Apical represent the coronal, middle, and apical third of the root canals. S1, S2, S3, S4, and S5 represent score 1, score 2, score 3, score 4, and score 5.
EDTA, ethylenediamine tetraacetic acid; NaOCl, sodium hypochlorite.
Coronal, Middle, and Apical represent the coronal, middle, and apical third of the root canals.
Comparisons of different labeled groups were statistically significant at the same third (p < 0.05).
EDTA, ethylenediamine tetraacetic acid; NaOCl, sodium hypochlorite; SD, standard deviation.
Discussion
Conventional irrigations with NaOCl and/or EDTA are not able to completely remove SL from the entire root canal wall, especially the apical third. 12,15,17 Our results showed that root canal walls treated with NaOCl alone were still covered with homogenous SL. The apical thirds were left almost unaffected after treatment with EDTA alone. NaOCl+EDTA was much more effective in removing SL than the NaOCl alone or EDTA alone. However, it failed to eliminate the SL at the apical thirds. This may be attributed to the complicated anatomic structure of the apical third of root canals, the small size of the apical third of canals, and the apical vapor lock effect. 11 These factors impede the circulation and action of the irrigating solutions.
LAI+NaOCl showed an effect similar to that of the NaOCl+EDTA in SL removal. It has been reported that radiation with the Er:YAG laser or Er,Cr:YSGG laser without any irrigant could effectively remove SL and open the dentinal tubules. 25,26 However, root canal walls become rough when treated with lasers only. 25 In addition, carbonization, cracks, and craters may occur in dentin treated with lasers without a coolant. 27,28 It was reported that laser treatments with irrigant solutions, for example NaOCl, reduced the chance of dentin damage. 28,29 Therefore, NaOCl and/or EDTA used in this study decreased the risk of damage to dentin. However, on the basis of the evidence of our study and previous studies, neither the LAI+NaOCl nor the NaOCl+EDTA can completely remove SL at the apical third. This may be because of the limited diffusion ability of the NaOCl+EDTA without the laser activation, which impedes their access to the apical third of the canals. In addition, it was reported that laser radiation alone was not as effective as EDTA alone in removing SL. 30 In our study, LAI+EDTA for 60 sec effectively removed SL from the entire root canal wall. This was consistent with previous reports. 14,23,24 However, because laser radiation enhanced the effect of EDTA, 14,23,24 60 sec of treatment with LAI+EDTA may increase the risk of dentin erosion or damage. It has been reported that dentin can be eroded or damaged when in contact with EDTA for >60 sec. 31
In this study, LAI+NaOCl+EDTA was the most effective treatment in SL removal. This may be related to the synergetic effect of the laser radiation, NaOCl, and EDTA. As previously discussed, laser radiation with NaOCl and EDTA irrigation individually were safe and effective in removing SL. The cavitation effect was believed to be the physical mechanism of LAI. 32 Vapor bubbles form when laser energy is absorbed by irrigant solution, which can cause a volume expansion that is 1600 times the original volume and then collapse and cause an acoustic streaming, which, in turn, causes the cavitation effect. 32 The cavitation effect enables irrigants (NaOCl and EDTA) to access the apical third of the canal. 21 –23,33 In this study, the LAI+NaOCl+EDTA was a treatment with NaOCl (30 sec) and EDTA (30 sec) for a total time of 60 sec, which will reduce the chance of dentin erosion. However, canals treated with the combination of Er,Cr:YSGG+NaOCl+EDTA demonstrated an extensive dentin erosion. It has been speculated that extensive dentin erosion may cause a vertical fracture to the root-treated teeth, 34,35 but this still needs to be further confirmed. On the contrary, the Er:YAG+NaOCl+EDTA combination gave the root canal wall a smooth, consecutive, and shallow-fossa-like surface, which may be beneficial to the adhesion and penetration of endodontic sealers into the dentinal tubules and may decrease the chance of a microleakage.
According to the SL scores, no significant difference was detected between the Er:YAG laser and the Er,Cr:YSGG laser when combined with NaOCl, EDTA, or NaOCl+EDTA. During the LAI, however, the fiber tip of the Er:YAG laser was placed at the orifice of the root canal, whereas that of the Er,Cr:YSGG laser needs to be placed at 1 mm shorter than the working length, which indicates that the Er:YAG laser may be superior to the Er,Cr:YSGG laser because it is applicable for canals of various shapes. In this study, straight canals were chosen to enable a relatively standard quantitative analysis, but more investigations with canals of various shapes should be explored in the future.
Conclusions
Under the conditions of this study, the LAI+NaOCl+EDTA treatment was the most effective in removing SL from the entire root canal wall. Thus, this may be considered an effective protocol for SL removal during an endodontic treatment.
Footnotes
Acknowledgments
The authors appreciate Liebert Language Editing Services very much for the professional editing of this article. This research was funded by the Natural Science Basic Research Plan in the Shaanxi Province of China (No. 2015JZ022) and the National Natural Science Foundation of China (Grant Nos. 81470733 and 81271125).
Author Disclosure Statement
No competing financial interests exist.