
Abstract
Introduction
T
Conventional irrigation using a syringe and a needle (syringe irrigation; SI) is the standard procedure, and today it is routinely used in endodontic practice. A number of different techniques have also been developed with the aim of improving the efficacy of root canal irrigation. Some studies described the enhanced irrigation efficacy of passive ultrasonic irrigation (PUI), in which an ultrasonic instrument is oscillated in the root canal irrigant. 7 –13 The efficacy is ascribed to the generation of cavitation, which causes rapid pressure changes through the rapid formation, expansion, and forceful collapse of vapor bubbles.
Recently, laser-activated irrigation (LAI) using various laser systems has gained much attention for its efficient cleaning of the root canal system. 14 –19 LAI with an Er,Cr:YSGG laser is the first that has been reported to generate cavitation when artificial root canals containing irrigant are irradiated, and its high potential efficacy in root canal irrigation has been described. 14 LAI is also reported to generate high fluid flow rates and shockwaves inside the root canal. 15,16 Due to these phenomena, LAI using Er,Cr:YSGG or Er:YAG lasers has been reported as similarly or significantly more effective than PUI and SI at removing apical smear layers. 15,16 Moreover, LAI is reported to eliminate dentin debris from complex canal areas 2.6 times more effectively than SI. 19
Sodium hypochlorite is routinely used worldwide as the root canal irrigant of choice because of its effective antimicrobial and organic tissue-dissolving capabilities. 20 –24 However, sodium hypochlorite can cause severe complications when it comes into contact with soft tissue 25 ; numerous studies have shown that the sodium hypochlorite irrigant used in SI may extrude beyond the apical foramen, causing chemical damage to the periapical tissue that can result in severe pain and swelling. 26 –28 This has led to a number of studies on irrigant extrusion outside the apical foramen, such as those measuring the level of irrigant extrusion and the pressure generated by SI and various other root canal irrigation techniques. 18,29 –36
We have previously measured the pressure generated outside the apical foramen during root canal irrigation and reported that various irrigation techniques, including LAI, induce pressure increases. 35,37 Apical extrusion of root canal irrigants has also been reported for LAI. 18,34 These findings suggest that LAI needs further evaluation regarding irrigant extrusion before safe clinical application. However, the apical pressure generated by LAI using an Er:YAG laser has not been investigated in detail. Thus, in the present study, we aimed to examine the influence of laser energy and tip insertion depth on the pressure generated outside the apical foramen during LAI.
Materials and Methods
Root canal irrigation techniques
Plastic pipette tips (no. 204; 10 μL short type; 0.40 mm in inner diameter of the tip and 6% taper; Fukaekasei, Hyogo, Japan) were used as root canal models with a canal length of 20 mm. To protect test equipment, distilled water was used as the irrigant instead of sodium hypochlorite.
An Er:YAG laser unit (Erwin AdvErl Unit; Morita Manufacturing, Kyoto, Japan) was used for LAI. The unit's specifications were as follows: wavelength, 2.94 μm; pulse oscillation; energy output, 30–350 mJ/pulse; repeat pulse frequency settings, 1, 3.3, 5, 10, 20, and 25 pps; and optical fiber transmission cable, laser beam delivered through contact tip. The R200T contact tip (Ø = 200 μm; Morita Manufacturing) was used for laser irradiation into the root canal model. Laser irradiation was conducted at 30, 50, and 70 mJ, 10 pps. After filling the root canal with distilled water, the laser tip was positioned at 2, 5, or 10 mm from the apical foramen, and the laser beam was irradiated for a period of 20 sec. The laser tip position was maintained throughout the irradiation period.
In the PUI group, the Piezon Master 400 (EMS, Switzerland) with a #20 U-file (Shofu, Kyoto, Japan) was used as the ultrasonic device. The unit produces a maximum frequency of 32 kHz. After filling the root canal with distilled water, the file tip was positioned at 2, 5, or 10 mm from the apical foramen, and the tip was activated at the highest power setting for a period of 20 sec.
A syringe (Nipro Syringe; Nipro, Osaka, Japan) and a 27-gauge (ø 0.40 mm) irrigation needle (Nipro Blunt Needle; Nipro) commonly used in endodontic practice were used for SI. After filling the root canal with distilled water, the needle tip was positioned at 2, 5, or 10 mm from the apical foramen, and 1 mL of the irrigant was delivered manually for a period of 20 sec.
In Experiment 1, which aimed to assess the effect of laser output energy, root canal models (n = 50) were assigned into the following groups: LAI groups (30, 50, or 70 mJ, 10 pps), PUI group, and SI group (n = 10 in each group). The tip of the laser device, the ultrasonic file, and the irrigation needle were positioned at 2 mm from the apical foramen, and each irrigation was performed repeatedly 10 times for 20 sec.
In Experiment 2, which aimed to assess the effect of tip insertion depth, root canal models (n = 90) were assigned into nine groups (n = 10 in each group) according to the combination of the method of irrigation (LAI, PUI, or SI) and the insertion depth of the tip (2, 5, or 10 mm from the apical foramen; referred to as −2, −5, or −10 mm, respectively). Each irrigation was performed repeatedly 10 times for 20 sec. The power setting of the laser system was set at 70 mJ, 10 pps.
Measurement of pressure outside the apical foramen
The apex of the root canal model was connected to a pressure sensor (AP-12S; Keyence, Osaka, Japan) using a vinyl tube filled with distilled water. The pressure generated outside the apical foramen was measured by connecting the pressure sensor to an amplifier (AP-81A; Keyence) and a recording device (NR-1000; Keyence). The mean maximum pressure (kPa) was measured (Fig. 1).
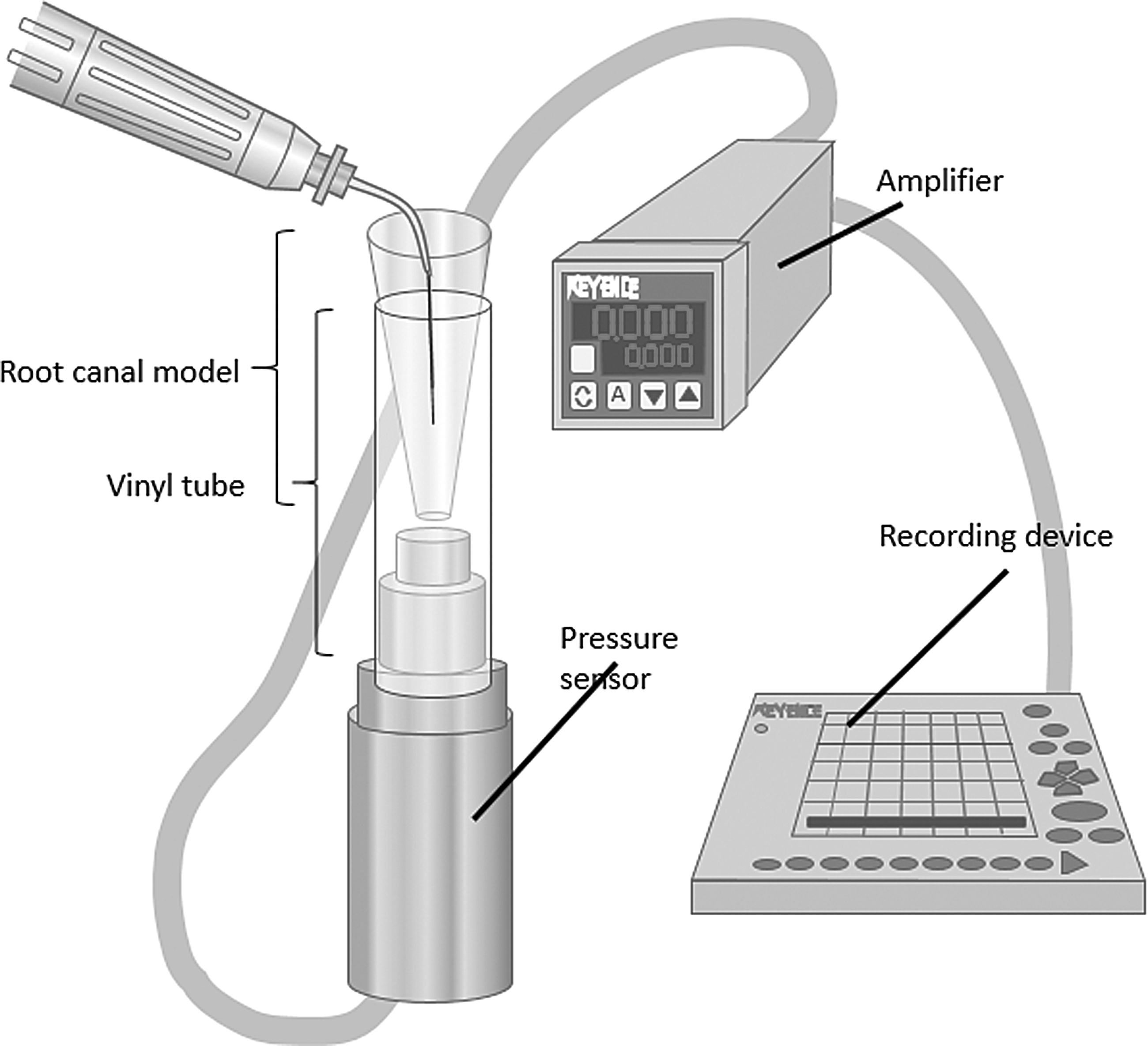
Schematic diagram of the experimental setup. The pressure caused by the irrigation was measured by a pressure sensor connected to the root canal model using a vinyl tube filled with distilled water.
Statistical analysis
Statistical analysis of the test results was performed using one-way analysis of variance (ANOVA) and the Tukey–Kramer test. A significance level of 5% was adopted for all analyses.
Results
Experiment 1: effect of laser output energy
As shown in Fig. 2, the mean maximum pressure generated in the three LAI groups increased according to the increase of the output energy, and there was a significant difference between LAI (30 mJ) and LAI (70 mJ) groups (p < 0.05). The three LAI groups showed significantly lower apical pressure compared with the SI group (p < 0.05). Compared with the PUI group, LAI (30 and 50 mJ) groups showed no significant differences, but the LAI (70 mJ) group generated significantly higher apical pressure (p < 0.05).
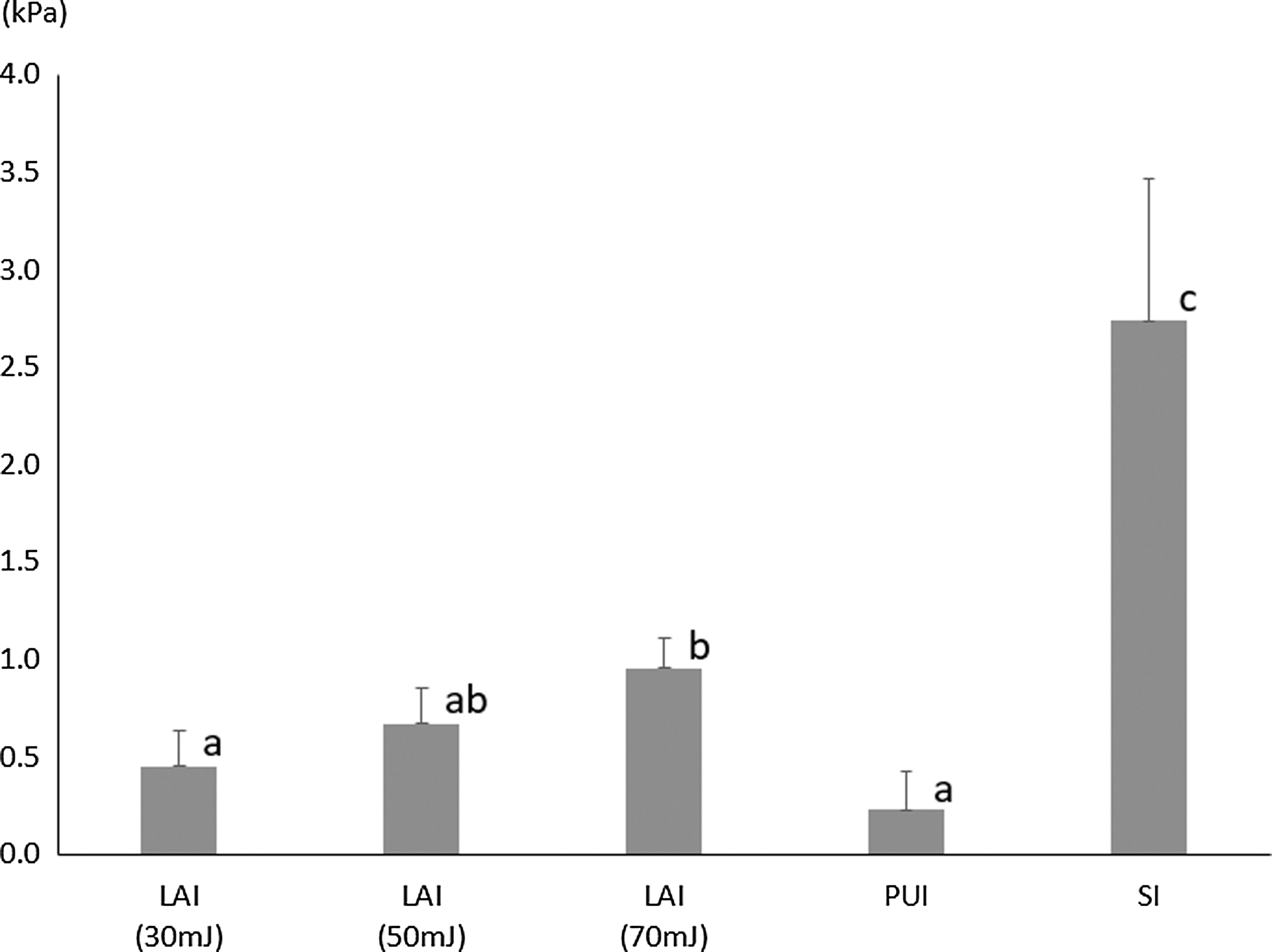
Comparison of maximum pressures generated outside the apical foramen during Er:YAG LAI, SI, and PUI (Experiment 1). Laser irradiation was conducted at 30, 50, or 70 mJ, 10 pps. Values represent the mean and SD (n = 10). Different superscript letters indicate statistically significant differences (One-way ANOVA and Tukey–Kramer test, p < 0.05). ANOVA, analysis of variance; LAI, laser-activated irrigation; PUI, passive ultrasonic irrigation; SD, standard deviation; SI, syringe irrigation.
Experiment 2: effect of tip insertion depth
As shown in Fig. 3, the mean maximum pressure generated in the LAI, SI, and PUI groups tended to decrease according to the decrease of the tip insertion depth, whereas there was no significant difference among the three LAI groups (p < 0.05). When the insertion depth was −2 mm from the apical foramen, the mean maximum pressure was SI > LAI > PUI (p < 0.05 among the groups). When the insertion depth was −5 and −10 mm from the apical foramen, the mean maximum pressure was SI = LAI > PUI (p < 0.05 between PUI and other groups).
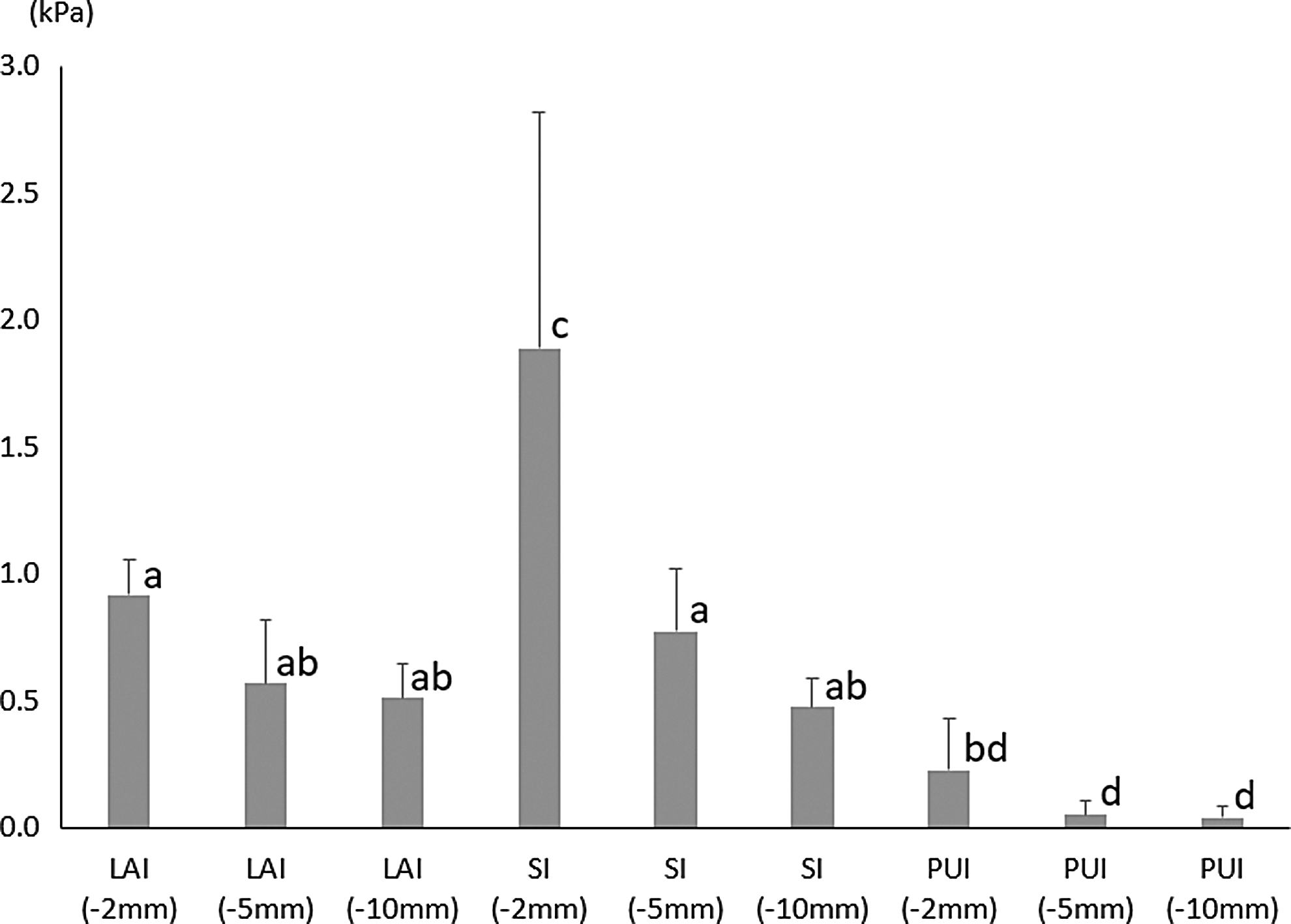
Comparison of maximum pressures generated outside the apical foramen during Er:YAG LAI, SI, and PUI (Experiment 2). The insertion depth of the tip was set at 2, 5, or 10 mm short of the apical foramen. Values represent the mean and SD (n = 10). Different superscript letters indicate statistically significant differences (One-way ANOVA and Tukey–Kramer test, p < 0.05).
Discussion
LAI is a potentially effective irrigation method, given that it generates cavitation, causing the high fluid flow rates and shockwaves inside the root canal. 14 Previous studies have reported that, compared to SI or PUI, LAI is similarly or significantly more effective at removing debris from inside the root canal 15,16 and that it decreases the amount of bacteria within the dentinal tubules. 36 However, concern exists regarding potentially harmful effects of the fluid flow generated by LAI, such as irrigant extrusion beyond the apical foramen due to apically-directed pressure generation. In the present study, we therefore examined the pressure generated outside the apical foramen with changing laser output energy and tip insertion depth and compared the findings with those of SI and PUI.
Based on a considerable amount of literature on the extrusion of irrigant solution beyond the apical foramen, 18,29 –34,37 –40 several methods have been used to evaluate the amount of extrusion, such as measurement of (1) the surface area of stained gelatin bleached by sodium hypochlorite; 30,34,37 (2) the volume of extruded irrigant using pipette tips; 29 (3) the concentration of extruded irrigant; 32 (4) the image area of a dye solution extruded into an aqueous solution; 38 and (5) the weight of extruded irrigant. 39,40 Previous studies on LAI have reported that the level of irrigant extrusion does not significantly differ from that with SI. 18,34 However, each measurement technique has limitations that should be taken into account when interpreting each finding. For example, two-dimensional evaluation of the surface area 30,34,37,38 may not be very accurate. In addition, the use of an aqueous solution or gelatin as the apical extrusion medium 18,30 –34,37 may cause permeation of the residual irrigant inside the root canal to the medium over time. In addition, measurement of the extrusion volume 29 may have been affected by the evaporation of extruded irrigant over time.
By measuring the pressure generated beyond the apical foramen, it is possible to monitor the force of extruded irrigant directly during the root canal irrigation procedure in real time without being affected by the abovementioned types of potential measurement errors. However, this method also has some limitations such as the fact that it does not directly measure the amount of extruded irrigant itself. Moreover, the amount of irrigants that are extruded from a root canal model is reportedly less than that from extracted teeth. 37 Further, the wall of the canal model is made of polymethyl methacrylate, and thus, the frictional resistance of the irrigant could be different compared to a dentinal root canal wall.
In Experiment 1, the pressure outside the apical foramen was significantly higher in the SI group than in the LAI and PUI groups. The higher pressure measured in the SI group was attributed to the positive pressure that this technique generates inside the root canal when the irrigant is expelled from the needle tip. In the LAI groups, the pressure outside the apical foramen tended to be energy dependent and there was a significant difference between LAI (30 mJ) and LAI (70 mJ) groups. This is not contradictory to the finding that LAI at 10 mJ showed slightly lower extrusion than LAI at 20 mJ 34 and suggests that there is an increasing concern of irrigant extrusion with increasing output energies.
Cavitation is a common phenomenon in both the LAI and PUI. In the LAI, cavitation is caused by microexplosions surrounding the end of the laser tip, in contrast to the PUI where cavitation is predominantly generated by ultrasonic vibration. 29 In both the LAI and PUI groups, negative pressure may have been generated in the area surrounding the tip as a result of the cavitation-induced reduction in pressure. In the LAI group, the microexplosions and pulse irradiation may have created flows toward the laser tip, which in turn caused apical extrusion of the irrigant and pressure beyond the apical foramen. Larger flow is generated with increasing laser energies. 17 Taken together, a large fluid flow generated by a high laser power setting (70 mJ) may be attributed to the significantly higher pressure compared to that generated by PUI.
In Experiment 2, the pressure outside the apical foramen tended to decrease with decreasing tip insertion depths in all of the irrigation methods (LAI, SI, and PUI). This is likely due to the decrease of fluid flow in the apical region when the irradiation site is set away from the apical foramen. 17 In contrast, it has been reported that LAI with the tip at 5 mm from the apical foramen removes dentin debris plugs as efficiently as PUI with the tip at 1 mm, 15 indicating that LAI may clean the root canal over a longer distance from the tip compared with PUI. It seems reasonable to assume that, during LAI, shallower insertion depths may be sufficient and can be recommended from the viewpoint of safety. This view is supported by an in vivo study showing that LAI using Er,Cr:YSGG laser caused no apical irrigant extrusion when the laser tip was kept above the orifice in the cervical region. 41
The central venous pressure (0.79 kPa = 5.88 mmHg in humans) 42,43 has been used as a hypothesized standard corresponding to naturally occurring pressure in the periapical tissue, and this pressure is believed to counteract the pressure generated during root canal irrigation. 44 Under the test conditions of the present study, the pressure generated in the SI (−2 mm, −5 mm) and LAI (−2 mm, 70 mJ) groups exceeded the abovementioned level, suggesting that LAI with a high power setting, together with SI, increases the concern of irrigant extrusion. SI at a flow rate of 2–3 mL/min has been reported to generate a pressure of 1.89 ± 0.13 to 3.61 ± 0.27 kPa (14.15 ± 0.99 to 27.1 ± 2.02 mmHg), 44 which is consistent with our findings. In the PUI group, however, none of the recorded pressure levels exceeded the central venous pressure and the pressure fluctuation behavior was predominantly of negative pressure beyond the apical foramen. This is in agreement with the finding that PUI generates less apical extrusion of an irrigant solution than SI. 29
The findings of the present study showed that changing the laser output and the tip insertion depth alters the pressure generated outside the apical foramen during LAI. This suggests that, under appropriate power settings and insertion depth, it is possible to generate cavitation effectively without causing irrigant extrusion beyond the apical foramen. Although it is not clear how much extrusion is problematic in clinical settings, it is preferable to reduce irrigant pressure beyond the foramen as much as possible to leverage the advantages of LAI. The present findings suggest that a lower power setting and a shallower tip position are recommended for LAI, particularly compared with PUI. Nevertheless, LAI generated a smaller or similar apical pressure increase compared with SI, suggesting that LAI is as safe or safer than SI as long as the potential for irrigant extrusion is considered.
Conclusions
Under the present experimental condition, LAI generated lower or similar pressure outside the apical foramen compared with SI, irrespective of the laser energy and tip insertion depth examined. However, LAI generated higher pressure compared with PUI.
Footnotes
Acknowledgments
This work was supported, in part, by a Grant-in-Aid for Young Scientists B from the Japan Society for the Promotion of Science (No. 25870195 to W.S. and No. 15K20398 to S.K.). The authors are grateful to Professor Emeritus Hideaki Suda, Tokyo Medical and Dental University for helpful discussion.
Author Disclosure Statement
No competing financial interests exist.