
Abstract
Introduction
L
Light energy must penetrate the skin barrier with a sufficient amount of energy to modulate pathophysiological processes in tendinopathies. The light scatters in collagen structures in the skin, and hemoglobin, water, melanin, and lipids absorb light energy. 8 Hence, the skin barrier is regarded a major obstacle to overcome in LLLT treatment of a deeply situated pathology.
Class 3b lasers used in tendinopathy treatment typically have a wavelength ranging from 632 to 904 nm and deliver energy either continuously or in the pulsed mode. 9 Lasers in the infrared spectrum (780–1000 nm) penetrate skin with less energy attenuation than red wavelength lasers (600–700 nm). 10 Consequently conditions such as tendinopathy are commonly treated with infrared gallium–aluminum arsenide 810–830 nm or a gallium–arsenide 904 nm laser, 6 whereas more superficial tissues such as the oral mucosa can be effectively treated with red wavelength lasers. 11
Interestingly, comparison of an 810 nm continuous wave (CW) laser and a 904 nm superpulsed wave (SPW) laser has shown significantly different penetration profiles in rat skin. In a previous study, the SPW 904 nm laser demonstrated superior skin penetration at the start of irradiation, and significantly less energy was absorbed by the skin during 150 sec of irradiation compared with the 810 nm CW laser. 12 Similarly, Enwemeka 13 found that less energy was attenuated in rabbit calf muscle for the 904 nm wavelength than for the 632.8 nm wavelength. This partly explains the difference in optimal energy doses reflected in WALT guidelines, that is, less energy is needed to produce the same clinical effects with a superpulsed 904 nm laser as for the continuous 810 nm laser.
Acute tendon disorders and other soft tissue injuries are also commonly treated with cryotherapy. However, clinical effects on soft tissue lesions, treatment parameters, and therapeutic mechanisms are not well supported by scientific evidence. 14 The effect of cryotherapy on acute musculoskeletal injury is primarily attributed to cold-induced vasoconstriction, which decreases edema, secondary hypoxic tissue damage, and the release of inflammatory mediators. 15
In a recent study on acute Achilles tendinopathy in rats, we found superior tendon biomechanics and histology when cryotherapy was followed by LLLT, compared with LLLT or cryotherapy alone as monotherapies or in a reversed order (laser first followed by cryotherapy). 16 This has made us speculate that perhaps skin and tendon optics can be altered by cryotherapy, which, in turn, may influence LLLT treatment outcome.
Therefore, the aim of this study was to investigate the penetration of a CW 810 nm laser and a SPW 904 nm laser through skin and Achilles tendon in healthy humans, before and after 20 min of cryotherapy.
Methods
Subjects
The study sample consisted 54 healthy human Achilles tendons. Twenty-seven students from Bergen University College (20 women and 7 men) with light skin color, ranging in age from 20 to 30 years (M = 22.5 years, SD = 2.0 years) volunteered to participate in the study. In this in situ study, both right and left Achilles tendon of the participants received the same experimental task (Table 1).
The values are mean with SD.
Indicates that there was no significant difference between left and right Achilles.
SD, standard deviation.
Instruments
Skin temperature was measured by a thermographic camera (Flir System, ThermaCam S65HS) and ancillary software (ThermaCAM Researcher Pro 2.8 SR-1). This software includes tools for quantifying the recorded temperature. The camera measures temperature with a precision of 50 mK at 30°C and has an accuracy of ±2% (Manufacturer's specifications). Two commercially available infrared class 3B lasers were used for irradiation of the Achilles (Table 2). The 810 nm wavelength laser (Thor LX2, Thor UK) operates in CW with 200 mW mean output power (MOP), spot size 0.0314 cm2 and power density of 6.37 W/cm2 (Manufacturer's specifications). The 904 nm wavelength laser (MID-laser, Irradia, Sweden) operates in a SPW with peak power 20 W, pulse train frequency 6 kHz and pulses 100 nsec (10–9 sec), width ( = 30.000 pulses/sec), 60 mW MOP, spot size 0.0364 cm2, and power density of 1.67 W/cm2 (Manufacturer's specifications). The laser MOP was measured using an optical power meter (OPM) system (Thorlabs Instruments, NJ, USA). The OPM system consists of a PM100 display unit with sample rate of 6 Hz and accuracy of ±1%, and a S121B silicon sensor. The S121B sensor has an aperture diameter of Θ = 9.5 mm with an optical power range from 500 nW to 500 mW and an accuracy of ±5% (Manufacturer's specifications). The real-timed ultrasonography (RTUS) was a Logiq-S8 (GE Healthcare, Minneapolis, USA). The unit has a 19" LCD screen display and operates in B-mode with high-definition speckle reduction imaging (SRI-HD), CrossXBeam resolution, and coded harmonic imaging. The linear matrix transducer (ML16-15-D) was tuned to frequency 12 MHz. The RTUS instrument has a caliper (Somet INOX CHROM, Czech Republic) with measurement precision scaled in millimeter. Domestic ice cube bags containing 28 ice cubes per bag were produced in a freezer at −10°C and used for cooling the tendons.
GaAs, gallium–arsenide.
Experimental procedure
Room temperature was recorded before each experiment started. The participants were placed in prone lying position on a bench with both ankles positioned outside the end of the bench, leaving the ankle joint in neutral position. Further, the experiment was carried out in eight steps. The MOP of each laser device was recorded for 3 sec before and after each irradiation. The order of application of 810 and 904 nm wavelength lasers was changed every second time (Fig. 1):
1. A pen mark was made on both Achilles tendons 2.5 cm proximal to the superior ridge of the Os calcaneus.
2. The Achilles area was ultrasonographically scanned in both the longitudinal and transverse planes, and one image in each plane was saved for further processing. The longitudinal image covered the superior tip of the Os calcaneus and distal third of the Achilles tendon. The transverse image was obtained with the probe covering the predrawn pen mark on the Achilles.
3. A thermographic camera was placed ∼50 cm above the subject's ankles covering both Achilles tendons, and one image was recorded.
4. Laser irradiation was performed with the subject positioned side lying and the calcaneus placed on a mobilization wedge (Fig. 2). The laser probe was placed on a tripod and pressed firmly to the medial side of the Achilles tendon (2.5 cm proximal for Os calcaneus). The handheld OPM was pressed firmly against the lateral side of the Achilles at the same level. The amount of energy penetrating through skin and tendinous tissue was recorded after 1, 30, 60, 90, and 120 sec irradiation by the 904 nm laser and after 1, 30, and 60 sec irradiation by the 810 nm laser.
5. Subjects were in prone lying position during 20 min of tissue cooling. An ice bag containing 28 ice cubes was applied directly above each Achilles area, covering the targeted distal third of the tendon. Every subject was in prone lying position with ice covering the Achilles area for 20 min. Subjects were not allowed to change body position to ensure an equal and comparable cooling effect.
6. The ice bags were removed after 20 min, and postcooling thermographic image was recorded (ad step 3).
7. The subject was positioned side lying and postcooling LLLT procedure was performed (ad step 4). While measuring laser energy penetration on one Achilles, the other Achilles was kept cooled.
8. The Achilles areas were scanned with RTUS (ad step 2). While scanning one Achilles, the other Achilles was kept cooled.
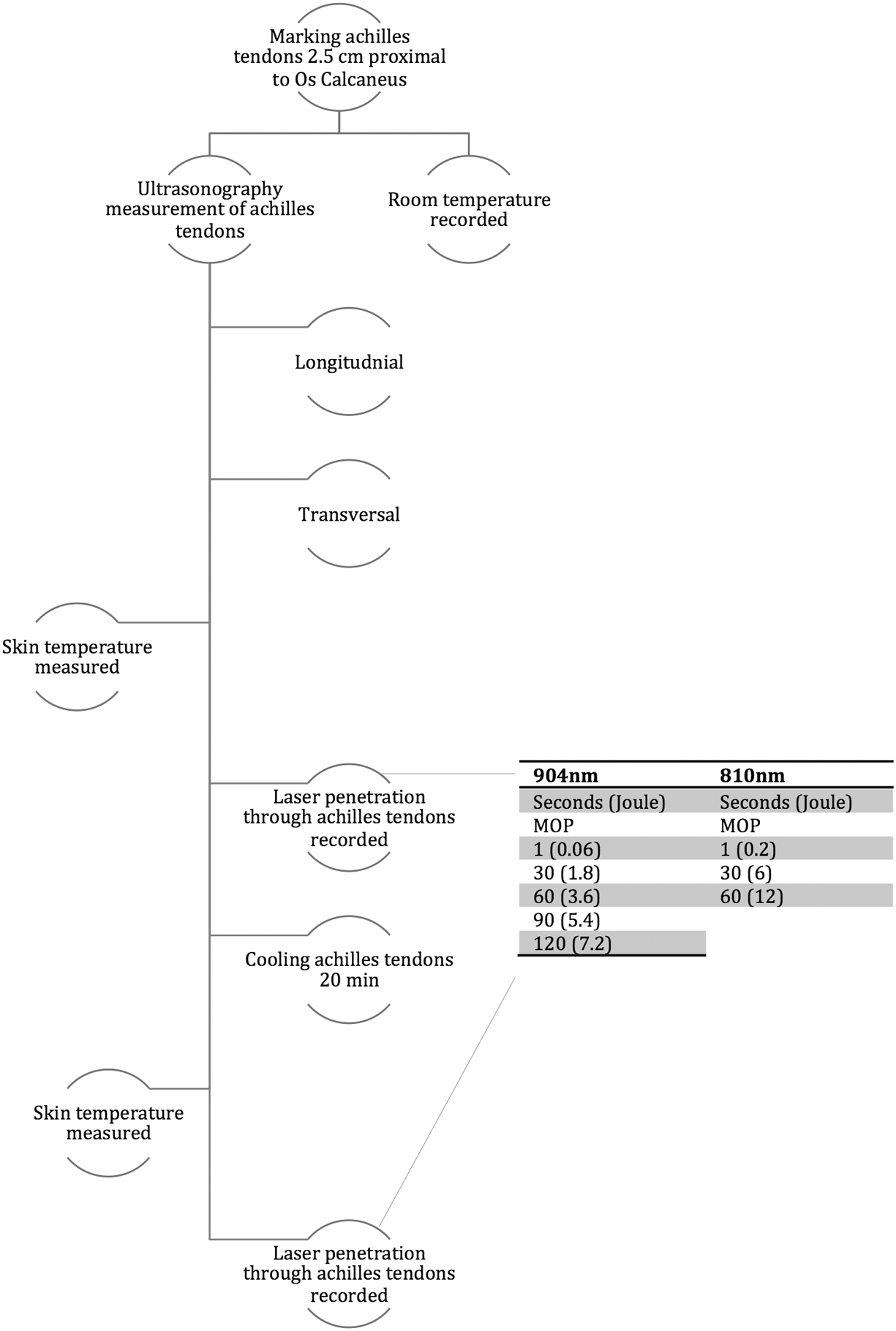
Flowchart of experimental procedure. Measurements were performed on right and left Achilles tendons of each subject. Tendons were irradiated for a total of 60 sec with the 810 nm laser and 120 sec with the 904 nm laser.

Laboratory setup for measuring laser energy penetration through Achilles tendon. Subject in side-lying position with left calcaneus resting on a mobilization wedge. The laser probe is fixed on a holder with firm skin contact to medial side of the Achilles tendon. The operator fixed the power meter manually to the lateral side of the Achilles tendon.
RTUS score
A built-in caliper was used to measure amount of tissue. In the longitudinal images, tendon thickness in an anterior–posterior direction was measured at 2.5 cm proximal from the tip of the Os calcaneus. In transversal images, tissue was measured 0.4 cm from the dorsal skin surface overlaying the Achilles. Tendon thickness was measured as the distance within the lateral–medial border of the peritenon. The total amount of tissue the laser irradiation should penetrate was measured as skin-to-skin distance.
Except for some transient feeling of stiffness in the Achilles tendons after cooling, none of the 27 enrolled subjects experienced any adverse events such as skin burns/freezing, nerve palsies, or parasthesia.
Main outcome measure
The amount of laser energy penetrating through the Achilles area before and after 20 min of cooling was calculated for each irradiation time and each laser.
Statistical analysis
Microsoft Excel (Microsoft Office Excel 2011) was used for statistical analysis and graphics. The mean (±SEM) amount of laser energy (mW) penetrating the Achilles area was calculated precooling and postcooling. The difference in energy penetration pre/postcooling is illustrated as the mean increase in mW and percentage of MOP when measured directly into the OPM. The mean (±SEM) tendon and skin thickness precooling and postcooling is displayed in centimeters. Energy loss per centimeter tissue was calculated as MOP (mW, no obstacle) – MOP (mW, through tissue)/skin-to-skin tissue thickness in centimeters. Student's pairwise t test was used for precooling/postcooling comparisons of energy penetration, tendon/skin thickness, and energy loss with statistical significance level set at p < 0.05.
Ethical approval
LLLT is considered harmless when applied to healthy tissue. 17 Owing to the consistent absence of adverse events and the lack of treatment intentions in this study, no special ethical approval was necessary.
Results
All study subjects (n = 54) completed the experimental procedure according to protocol (Fig. 1). The baseline room temperature was 21.9°C (SD ±0.7). Thermography recordings before cooling showed Achilles mean skin temperature at 28.2°C (SD ±1.8). Skin temperature dropped to a mean value of 4.8°C (SD ±3.6) after 20 min of cooling.
Mean output power (no obstacle)
The 904 nm laser was stable and not significantly different (p = 0.22) during the 120 sec precooled and postcooled irradiations at 54.5 mW (SD ±2.41) and 55.2 mW (SD ±3.05) (p = 0.22), respectively. The 810 nm laser was stable during the 60 sec exposure period at 202.7 mW (SD 3.75) before ice application and at 204.3 mW (SD 2.99) after ice application. The MOP increased by 1.6 mW in the after ice application measurement, which was found to be a statistically significant increase (p < 0.05).
904 nm laser penetration
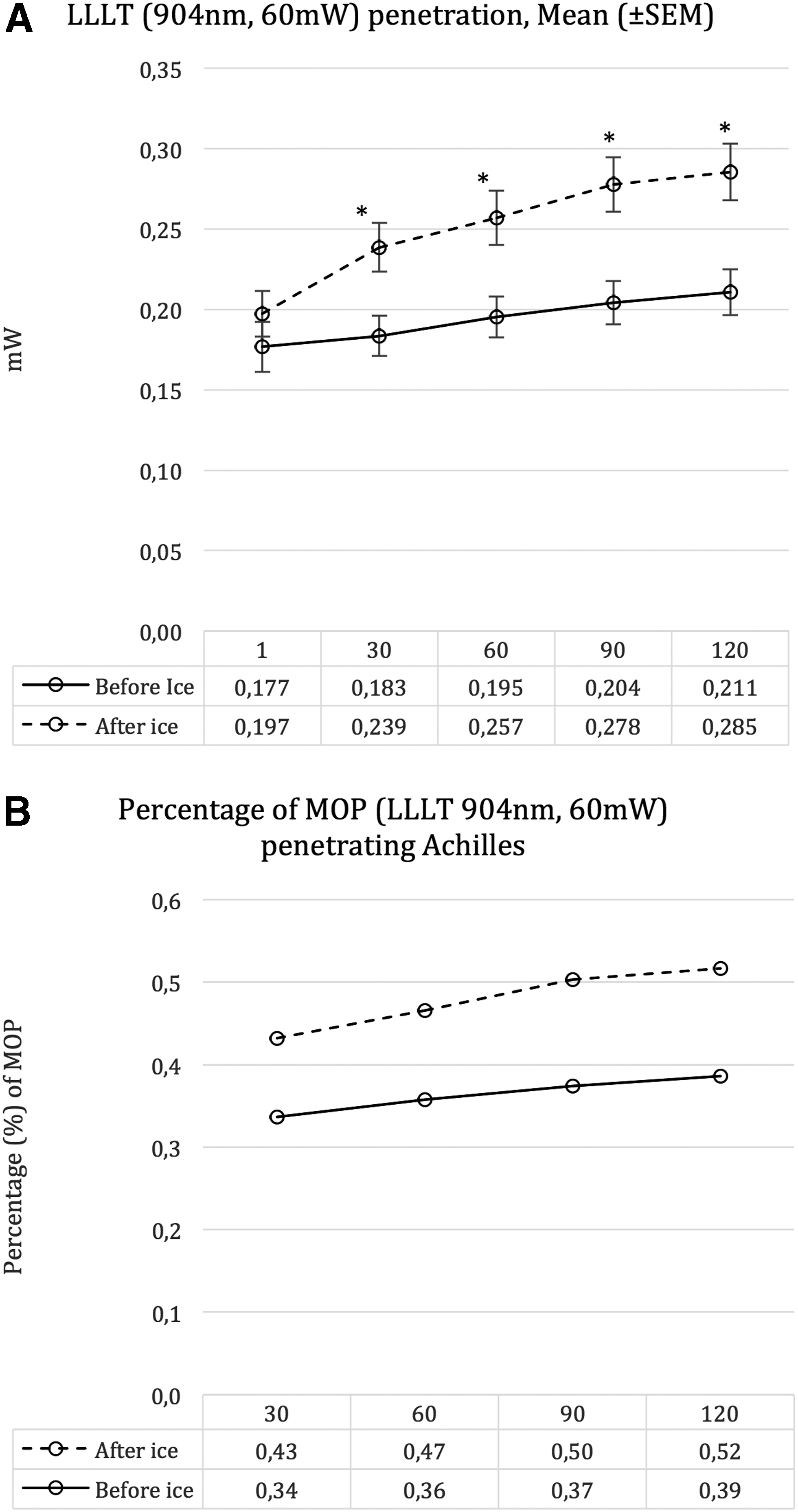
Irradiation with the 904 nm laser showed a linear increase in tissue penetration with time (30–120 sec), and during this laser exposure period, penetration increased by 0.03 mW (19%) before and by 0.09 mW (45%) after cooling. Energy penetration after ice application was significantly increased (p < 0.01) at all time intervals (30, 90, and 120 sec) compared with that before ice application at all time intervals (Fig. 3A and Table 3). The percentage of energy penetrating the Achilles area during the exposure period was 0.34–0.39% of MOP before cooling, that is, a relative increase of 15%. The percentage of energy penetrating the same area was 0.43–0.52% of MOP after cooling, that is, a relative increase of 21% during the laser exposure period (Fig. 3B). Laser energy loss per centimeter of tissue was significantly (p < 0.05) higher at all time intervals after ice application (Fig. 4A).
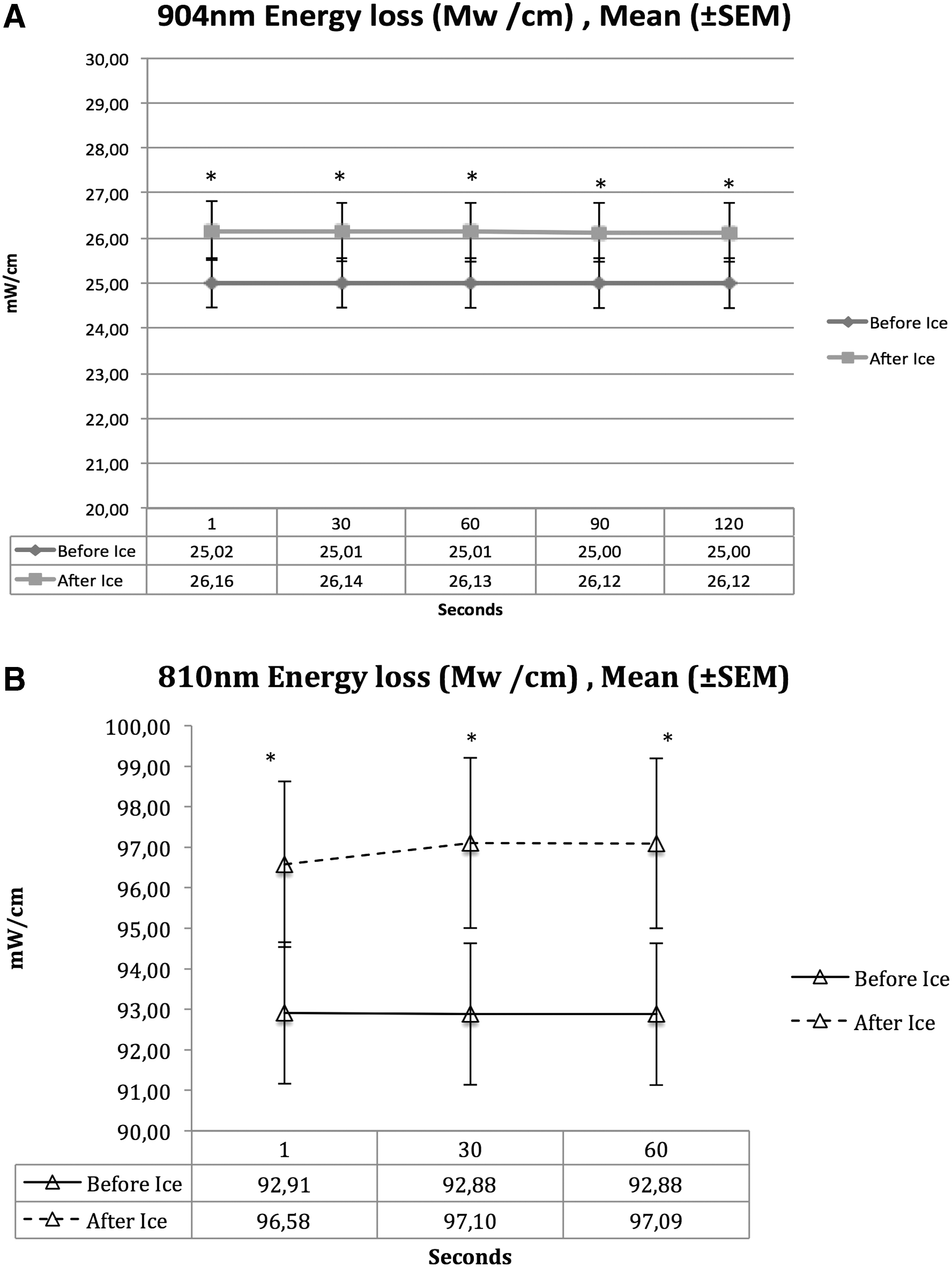
Energy loss refers to degree of attenuation of light energy in the irradiated tissue. Increase in energy loss per centimeter tissue equals less energy attenuated in the tissue.
SEM, standard error of the mean.
810 nm laser penetration
Irradiation with the 810 nm laser showed a stable energy penetration during the 60 sec of exposure. Laser energy penetration at the interval 30–60 sec increased 0.012 mW (2%) in noncooled Achilles and 0.02 mW (3%) in cooled Achilles. The amount of energy in mW penetrating the Achilles area after ice application was significantly increased (p < 0.01) at all time intervals compared to before ice application (Fig. 5A and Table 3). The energy penetrating the Achilles area before and after ice application was 0.24–0.25% and 0.30–0.31% of MOP, respectively (Fig. 5B). Hence, there was a relative energy increase of 4% before cooling and 3% after cooling during the laser exposure period. Laser energy loss per centimeter of tissue was significantly (p < 0.05) higher at all time intervals after ice application (Fig. 4B).

RTUS: Skin-to-skin distance and Achilles tendon thickness
The mean thicknesses of the Achilles tendons before ice application were 0.51 cm (SD ±0.07) in the longitudinal and 1.83 cm (SD ±0.40) in the transversal images. The total thickness of tissue the laser should penetrate before ice application, that is, skin-to-skin distance, was 2.20 cm (SD ±0.30). The mean Achilles tendon thickness in logitudinal images was 0.51 cm (SD ± 0.07) both before and after ice, and was not significantly different (p = 0.49). The mean transversal Achilles tendon thickness after ice application was 1.77 cm (SD ±0.38) and was significantly reduced (p = 0.03) compared with that before ice application. The skin-to-skin distance after ice application was significantly reduced (p = 0.05) compared with that before ice application, at 2.14 cm (SD ±0.34) (Fig. 6).
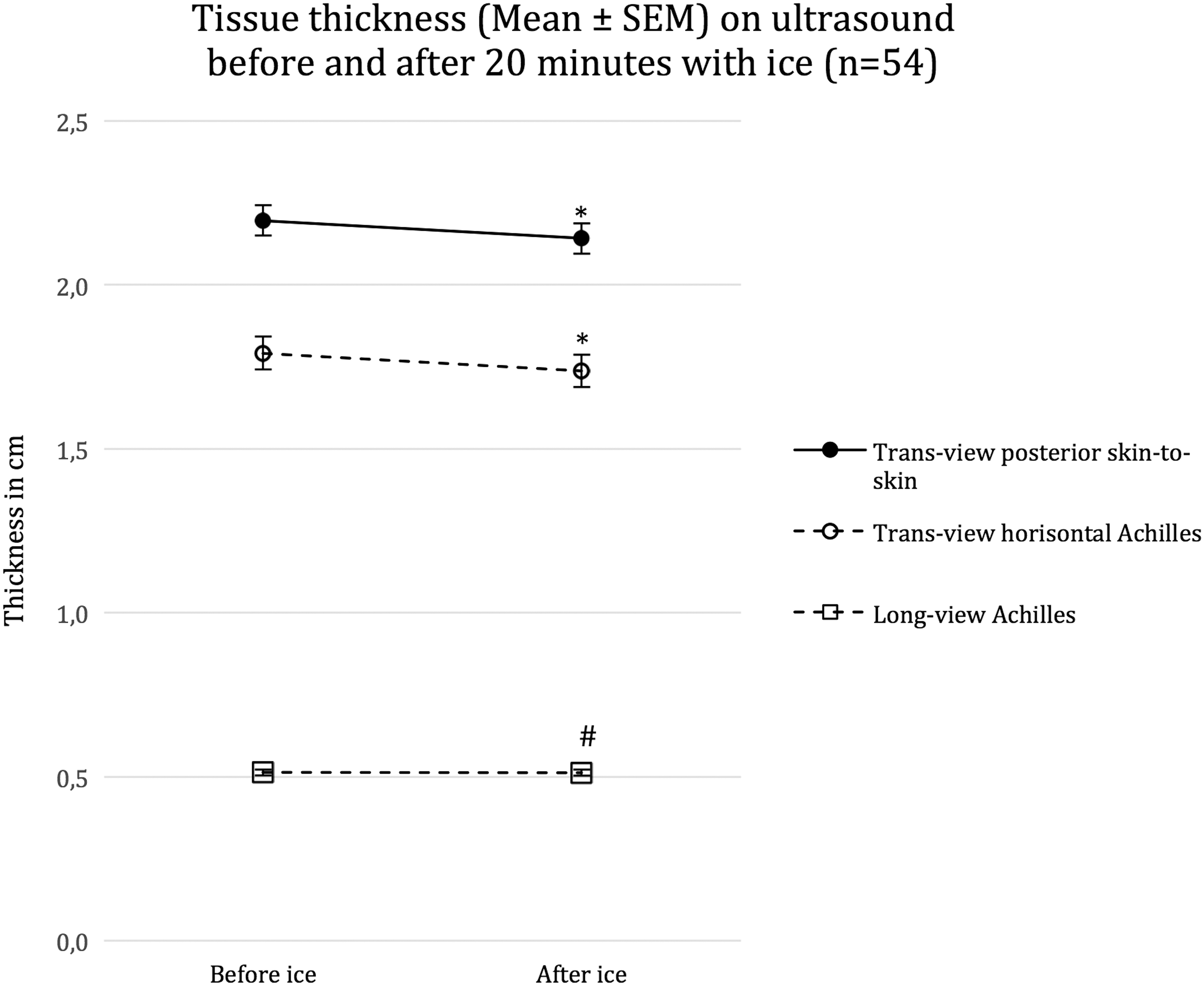
Mean (±SEM) Achilles tendon thickness and skin-to-skin thickness before and after 20 min of cooling. *Indicates significant difference (p < 0.05) in tissue thickness before and after ice application. #Indicates no significant difference (p > 0.05) in tissue thickness before and after ice application.
Discussion
To our knowledge, this is the first study to investigate the effect of cryotherapy on LLLT penetration profile in human Achilles. We found that applying ice above the Achilles area for 20 min significantly increased penetration of energy for both lasers tested when compared with penetration of noncooled tendons. RTUS measurements showed that Achilles tendon thickness and the total amount of tissue the lasers should penetrate, that is, skin-to-skin distance, were significantly reduced after ice application.
Increased tissue penetration, as described throughout this article, simply refers to less attenuation of energy in the irradiated tissue. The degree of attenuation refers to the amount of energy being absorbed and scattered in the tissue, thereby preventing the laser beam from continuing penetration in the direction toward the OPM placed on the opposite side of the irradiation point. Consequently, no conclusions regarding the exact amount of energy absorption and scattering, or changes in interrelationship between these two characteristics, can be drawn from our study. However, we have demonstrated a significantly higher laser energy loss per centimeter of tissue after cooling the Achilles area, which indicates that less laser energy is attenuated in the tissue.
This finding may have some interesting implications for researchers and clinicians targeting deeply situated tissues such as the hamstrings tendon and hip or sacroiliac joint. We found no published LLLT studies targeting pathologies in deeply situated tendons such as the proximal hamstrings or iliopsoas. Currently, evidence supporting LLLT for tendinopathies is limited to the Achilles, lateral elbow extensors, and rotator cuff tendons. 4 –6 The depths from the skin surface to the Achilles, lateral elbow extensors, and supraspinatus tendon were all measured and found to be less than 10 mm in an RTUS study. 18 Conversely, the psoas muscle origin at the lumbar transverses, and the proximal tendinous hamstring attachment at the ischial tuberosity is situated ∼4–5 cm from the skin surface. 19,20 Therefore, our findings of reduced attenuation of laser energy after cooling may have some interesting implications for future researchers and clinicians targeting deeply situated tissue, or superficial tendons covered by adipose subcutaneous thickness.
It has been argued that differences in adipose thickness across individuals or anatomical locations should affect clinical outcomes, and that cooling durations should be guided by skinfold thickness covering the injured area. 21 A near twofold increase in cooling time has been demonstrated to lower intramuscular temperature by 7°C in humans with 20 mm compared with 10 mm subcutaneous skinfolds. 22 As subcutaneous adipose tissue consists of lipids, connective tissue, neural, and vascular tissue, 23 increased attenuation of laser energy should also be expected. The relationship between different body compositions, LLLT treatment parameters, and clinical outcomes is an unexplored area in LLLT research. In this perspective, our findings of less attenuation of laser energy in cooled tissue may influence both clinical practice and future research.
In our study, 20 min of cooling reduced superficial skin temperature from 27.6°C to 4.8°C. Intermittent cooling in 3 × 10 min sessions significantly decreased deep Achilles capillary blood flow by 71% in healthy humans. 24 Reduced blood volume and hemoglobin levels have also been demonstrated in human leg skin and ankle dorsiflexors during 30 min of cooling. 25 Our measurements of less laser energy attenuation, that is, increased penetration, in cooled tissue may be explained by reduced skin and tendinous microcirculation and amount of laser energy absorbing hemoglobins. However, cooling soft tissue also reduces cell metabolism. 21 It is possible that reduced attenuation of laser energy simply reflects the reduced metabolic state of the tissue.
Interestingly, we also found that cryotherapy decreased skin and tendon thickness, which should influence the penetrative abilities of the laser energy. Cold sensitive receptors in the skin are triggered by cryotherapy, which stimulates the sympathetic activation of cutaneous vasoconstrictor nerves on smooth vessel walls. 26 This reduction in size of blood vessels because of a vasoconstrictor response also makes them a smaller target for the laser irradiation. Hence, this may also contribute to the increased penetration of laser energy through tissue subjected to cryotherapy. As blood vessels are space occupying structures in the skin and tendons, 27 our measurements of decreased tissue thickness after cooling could also be explained by the vasomotor response.
In line with previous studies, we also observed that energy penetration through tissue increased with longer wavelengths. 12,13 The 904 nm laser penetrated tissue with a percentage of MOP 10–16% higher than the 810 nm laser, for 60 sec of irradiation. This finding corresponds well to previous in vitro examinations of laser penetration in human and animal skin flaps. 12,28 Although the 810 nm laser displays a stable and flat penetration curve during the exposure period of 60 sec, the 904 nm laser penetration increased linearly with time. This finding has previously been hypothesized to arise from possible photobleaching of the skin by the 904 nm laser. 12 Interestingly, this linear increase occurred even more rapidly in cooled tissue. The reduced attenuation of laser energy in cooled tissue suggests that tissue temperature affects the optical properties of skin and tendon tissue. Future studies are needed to elucidate this phenomenon.
The use of a laser tripod and a hand-held OPM has its limitations. The exact amount of pressure exerted on the Achilles tendon from these devices was not measured. Although our experimental setup was identical for each measurement, we cannot exclude that small variations in Achilles squeezing occurred and influenced the outcome. The operator holding the OPM was blinded to all measurement recordings, but could not be blinded to whether the tendon was cooled or not. We also observed a difference in MOP (no obstacle measurements) before and after ice application for the 810 nm CW laser. The increase in MOP after ice application was very small (1.6%), but it was still significantly (p < 0.01) higher than the MOP recorded before ice application. However, a higher percentage of MOP penetrating cooled Achilles was also found for the 810 nm CW laser, indicating that the increased penetration after ice application cannot be explained by higher MOP from the laser device alone. It should also be emphasized that our results originate from a homogeneous population consisting of healthy young adults with light skin tone. Dermal and tendinous tissues degenerate with increasing age, 29,30 and can be influenced by both disease and activity levels. 31 –34 Careful consideration should be given before extrapolating the results of this study to a heterogeneous general population with pathology.
Conclusions and Summary
The penetration of laser energy through the Achilles area increased significantly after 20 min of cryotherapy in healthy young adults. Our findings indicate that attenuation of laser energy is reduced in cooled tissue. These findings occurred in the presence of a significant reduction in cooled skin and tendon thickness.
Footnotes
Author Disclosure Statement
No competing financial interests exist.