
Abstract
Introduction
E
The successful prognosis of an endodontically treated tooth depends greatly on its remaining structural integrity. 10 Therefore, minimally invasive endodontics (MIE) has been emphasized in recent years. 11 MIE aims at removing or reversing disease by causing the minimum loss of dental tissues, conserving the maximum structural integrity, and, as a result, preserving the longevity of the endodontically treated tooth. Under the condition of the same or similar disinfection efficacy, a smaller ATWW should be used during the root canal treatment, based on the principle of the MIE.
Erbium:Yttrium Aluminum Garnet (Er:YAG) laser has conventionally been used for removal of carious dentin, preparation of cavity, and treatment of dentine hypersensitivity. 12,13 It was also used for the removal of smear layers from canals. 14 Recently, the Er:YAG laser was introduced for endodontic treatment due to its excellent antibacterial effect. 15,16 Bactericidal potential of Er:YAG laser might be related to the evaporation effect of cellular water, which could expand quickly during the laser pulse and lead to the disintegration of bacterial cell wall. 17 However, carbonization, cracks, and craters may happen to dentin treated with laser radiations without a coolant. 18,19 Previously, we found that Er:YAG laser irradiation dramatically enhanced the bactericidal effect of NaOCl irrigation by facilitating its penetration. 20,21 This can be attributed to the physical mechanism, the cavitation phenomenon, of laser-activated irrigation (LAI). 22 When the Er:YAG laser is activated for root canal disinfection, its optical fiber is placed at the orifice of the root canal, instead of inserting it inside, suggesting a smaller ATWW may be needed when the Er:YAG laser is combined with NaOCl for endodontic treatment.
In this study, we tested the disinfection efficacy and potential of Er:YAG laser-activated NaOCl irrigation (Er:YAG + NaOCl) for MIE. Three parameters (ATWW, output power of the Er:YAG laser, and radiation time of the Er:YAG laser) were examined, and the results were compared with the NaOCl-alone group. We hypothesized that the disinfection efficacy of the Er:YAG + NaOCl would be influenced by the output power and radiation time of the Er:YAG laser, and the Er:YAG + NaOCl might achieve a similar disinfection efficacy at a smaller ATWW compared with NaOCl alone.
Materials and Methods
Tooth collection and preparation
Three hundred thirty-five permanent human teeth with straight root canals and mature apical roots were selected radiologically from the School of Stomatology, Fourth Military Medical University, China. These teeth were caries free, intact, single rooted, and freshly extracted for orthodontic treatment. Teeth with previous coronal restorations or root canal treatment were excluded. The experimental protocol was approved by the ethics committee of the institutional review board of the university, and written informed consents were obtained from all the donors. The procedures of tooth preparation were similar to that of our previous studies. 20,21 In brief, after stored and sterilized in NaOCl (0.5%; Sigma-Aldrich Co.) for 24 h, the selected teeth were decoronated to a standard 12 mm root segment. The root canals were first negotiated and instrumented to a 10# K-file (Dentsply Maillefer). The #10 K-file was inserted into the root canals until it was visible at the apical foramen, and the distance from the orifice to the apical foramen was measured (M mm). The working length was equal to (M − 1) mm. Next, they were prepared with K3 nickel-titanium rotary instruments (SybronEndo) using a crown-down technique, and all the canals were enlarged to an apical working width of 15#/0.04. After treated with NaOCl (5.25%, 5 mL, 4 min), ethylenediaminetetraacetic acid (EDTA, 17%, 5 mL, pH = 7.2, 4 min), and autoclaving (121°C, 15 min), five canals were randomly selected to ensure that the smear layer and microorganisms had been eliminated by examining them under scanning electron microscopy (SEM); another five canals were selected to further confirm the elimination of the microorganisms by incubating them in brain–heart infusion (BHI; Difco) broth for 48 h at 37°C.
Culture of Enterococcus faecalis and specimen inoculation
The protocols were similar to that of our previous studies. 20,21 In brief, Enterococcus faecalis (ATCC 29212), thawed from frozen stock, was streaked onto a BHI agar plate and incubated anaerobically at 37°C for 24 h. Single colonies were inoculated into BHI broth and cultured at 37°C for 24 h. Before inoculation, the root surfaces were sealed with nail polish. The root canals were then incubated individually in 1.5 mL E. faecalis suspension [∼108 colony forming units (CFUs)/mL] at 37°C for 4 weeks. Five randomly selected specimens were examined by SEM to ensure the formation of E. faecalis biofilm, and the medium was refreshed every 3 days. Each time, samples of the replaced media were selected randomly and identified using 16S rRNA gene sequencing to ensure purity.
Irrigation instruments and irrigants
Syringe with a 27G side-vented needle (Patterson Dental Supply) and an Er:YAG laser (Fotona) emitting a wavelength of 2940 nm with a photon-induced photoacoustic streaming (PIPS) tip (diameter = 300 μm; Fotona) were used in this study. NaOCl (0.5% and 5.25%) was diluted from a 10.0% NaOCl solution (Sigma) in deionized water and used immediately after preparation. Normal saline (NS, 0.9%, Kelun Pharmaceutical Co.) was used directly after purchase.
Grouping and treatments
The specimens were randomly divided into 16 groups after incubation and are listed in Table 1. The treatment for each group is described as follows: (A) Untreated group: 20 canals were left untreated. (B) 15#/NS group (negative control): 20 canals were treated with NS (5 mL, 60 sec) irrigation. (C) NaOCl-only groups (a total of five groups): 20 canals in each group were prepared individually to an ATWW of 15#/0.04 (positive control, no further preparation), 20#/0.04, 25#/0.04, 30#/0.04, and 40#/0.04 using K3 instruments. Next, the specimens were treated with 5.25% NaOCl (5 mL, 60 sec) irrigation, followed by 5 mL of sodium thiosulfate (Sigma) and NS for 60 sec sequentially to deactivate any residual NaOCl. For groups B and C, the irrigants were delivered using a syringe with a 27G side-vented needle (Patterson Dental Supply). The needle was moved back and forth. (D) Er:YAG + NaOCl groups (a total of five groups): first, 20 canals in each group were individually prepared to an ATWW of 15#/0.04, 20#/0.04, 25#/0.04, 30#/0.04, and 40#/0.04. For each group, the root canals were first filled with 5.25% NaOCl (5 mL) and radiated with Er:YAG laser at an output power of 0.3 W for 20 sec. Next, the root canals were filled with sodium thiosulfate (5 mL) and NS (5 mL), and radiated with Er:YAG laser at 0.3 W for 20 sec. The optical tip (PIPS) was placed and activated at 1 mm below the orifice of the canals with 15 sec intervals. (E) Er:YAG + NaOCl groups of different output powers and radiation times (a total of four groups): 20 canals with an ATWW of 15#/0.04 in each group were individually treated with Er:YAG + NaOCl at an output power of 0.3 W for 40 and 60 sec, or at 0.5 and 1.0 W for 20 sec. They were then treated with sodium thiosulfate and NS as described above.
ATWW, apical terminal working widths; NS, normal saline; NaOCl, 5.25% NaOCl; SSP, super-short pulse with 50 μsec; Er:YAG, Erbium:Yttrium Aluminum Garnet.
SEM evaluation
The protocols were similar to that of our previous studies. 20,21 In brief, longitudinal grooves were carved onto the root surfaces with high-speed diamond burs (Brasseler) without entering the inner parts of the root canals. They were split with an acuminate chisel and hammer. Next, the specimens were fixed in 2.5% glutaraldehyde for 24 h, dehydrated in an ascending acetonitrile series (50%, 70%, 80%, 90%, and 100% twice for 20 min each), dried in a lyophilizer (ES-2030; Hitachi), sputter-coated with platinum (Ion Sputter E-1045; Hitachi), and observed by SEM (S-4800; Hitachi). For image acquisition, one microscopic field was selected every 1 mm, starting from coronal to apical sites of the specimen (n = 5, 12 mm in length); a total of 60 fields were selected for the evaluation.
Estimation of CFUs and evaluation of bacterial reduction
The protocols were similar to that of our previous studies. 20,21 In brief, the untreated and treated root canals in each group (n = 20 for each group) were used to measure the number of viable bacteria before and after treatments, respectively. The samples on root canal walls were collected using three sterile paper points per canal, with the paper points saturated with NS and kept in the canals for 60 sec. Dentin shaving samples were obtained by over-preparing the root canals to 5 mm greater than the working length using the master point K3 instruments in each group, removing ∼0.1 mm of dentin around the canal. The paper points and powder dentin samples from the same canal were transferred together to 1 mL NS and vortexed for 10 sec. Bacterial suspensions were diluted in 10-fold steps. One hundred microliters of each dilution was spread onto BHI agar plates, which were incubated at 37°C for 48 h, and then the CFUs were recorded. The numbers of CFUs in the untreated group multiplied by the corresponding dilution ratios represented a close estimate of viable bacteria before treatments (M). The number of viable bacteria after treatments was denoted as N, and the bacterial reduction = (M − N)/M × 100%.
Statistical analysis
The bacterial reductions after treatments were expressed as the mean ± standard deviation and analyzed using a one-way analysis of variance followed by the Tukey test using the SPSS statistics package for Windows (version 13.0; SPSS, Inc.). The statistical significance level was set at α = 0.05.
Results
Root canal preparation and inoculation
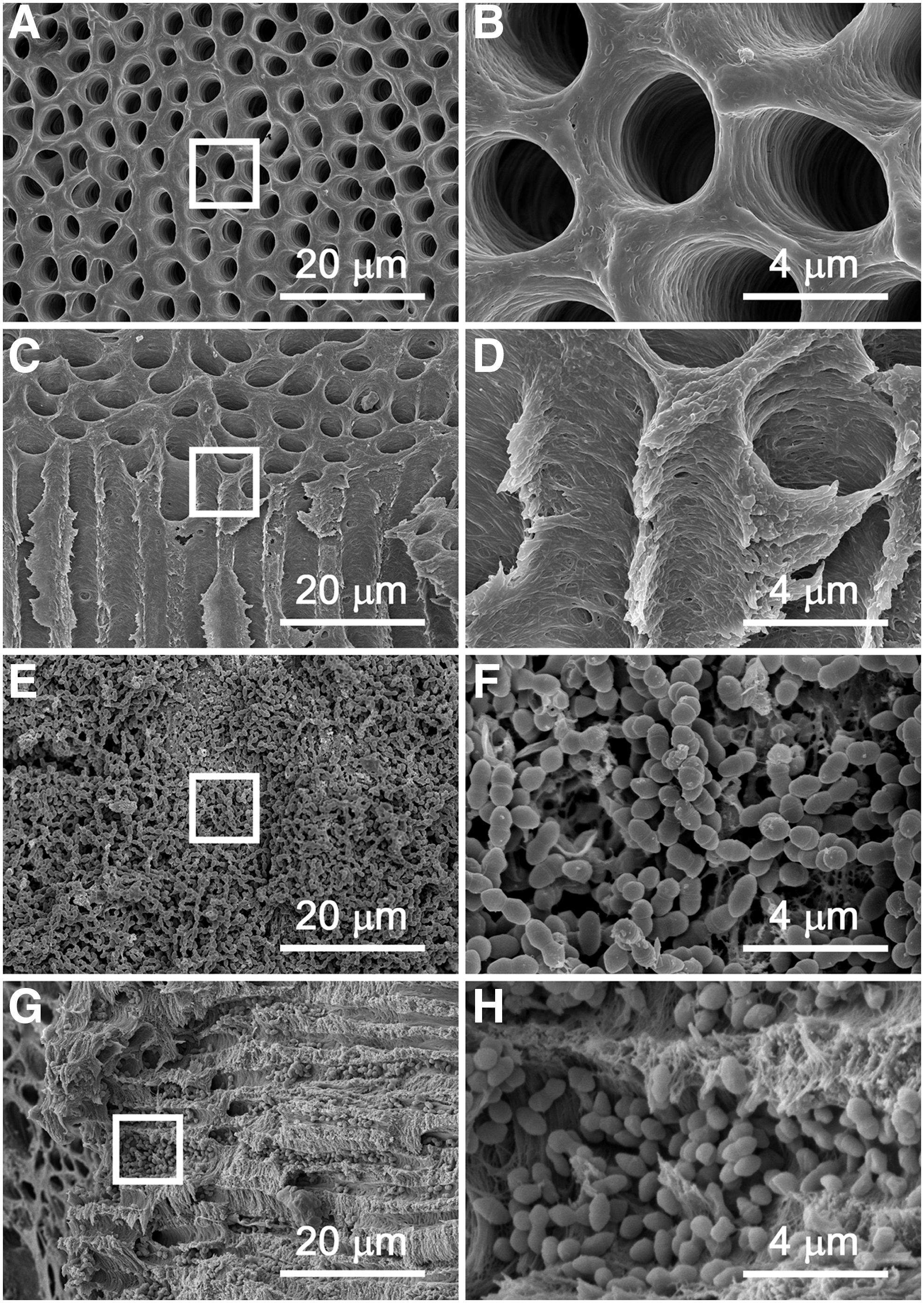
As shown in Fig. 1, they were representative SEM images taken from the conjunction site of the middle and apical thirds of the canals. Smear layer and microorganisms inside the tooth root were undetectable after sequential treatments with NaOCl, EDTA, and autoclave (Fig. 1A–D). The orifices of the dentinal tubules were completely opened (Fig. 1A, B), and the dentinal tubules were clear and unimpeded (Fig. 1C, D). In addition, the BHI medium remained clear after culturing the specimens for 48 h, further confirming that the microorganisms had been eliminated. These root canals were used for the following bacterial inoculation experiments.
Root canals before
After a 4-week bacterial incubation, biofilm-like structures were detected on the root canal walls (Fig. 1E, F). A longitudinal cross-sectional image clearly showed that E. faecalis invaded into the dentinal tubules (Fig. 1G, H) and the bacterial cells exhibited a smooth, uniform, and bright surface (Fig. 1F, H).
Bacterial reductions after treatments
As shown in Fig. 2, the bacterial reduction percentage increased as the ATWW were enlarged from 15# to 40# in both the NaOCl and Er:YAG + NaOCl groups, which were all significantly greater (p < 0.001) than that in the negative control group (40.3%, not shown in the figure). The maximum bacterial reduction was 99.9% for the 40#/Er:YAG + NaOCl group and 93.6% for the 40#/NaOCl group. The Er:YAG laser significantly enhanced the disinfection efficacy of NaOCl at each ATWW (p < 0.001). In addition, under the condition of the similar disinfection efficacy, the Er:YAG + NaOCl group allowed a smaller ATWW compared to the NaOCl group. The disinfection efficiency of the 15#/Er:YAG + NaOCl group was similar to that of the 40#/NaOCl group (p > 0.05).
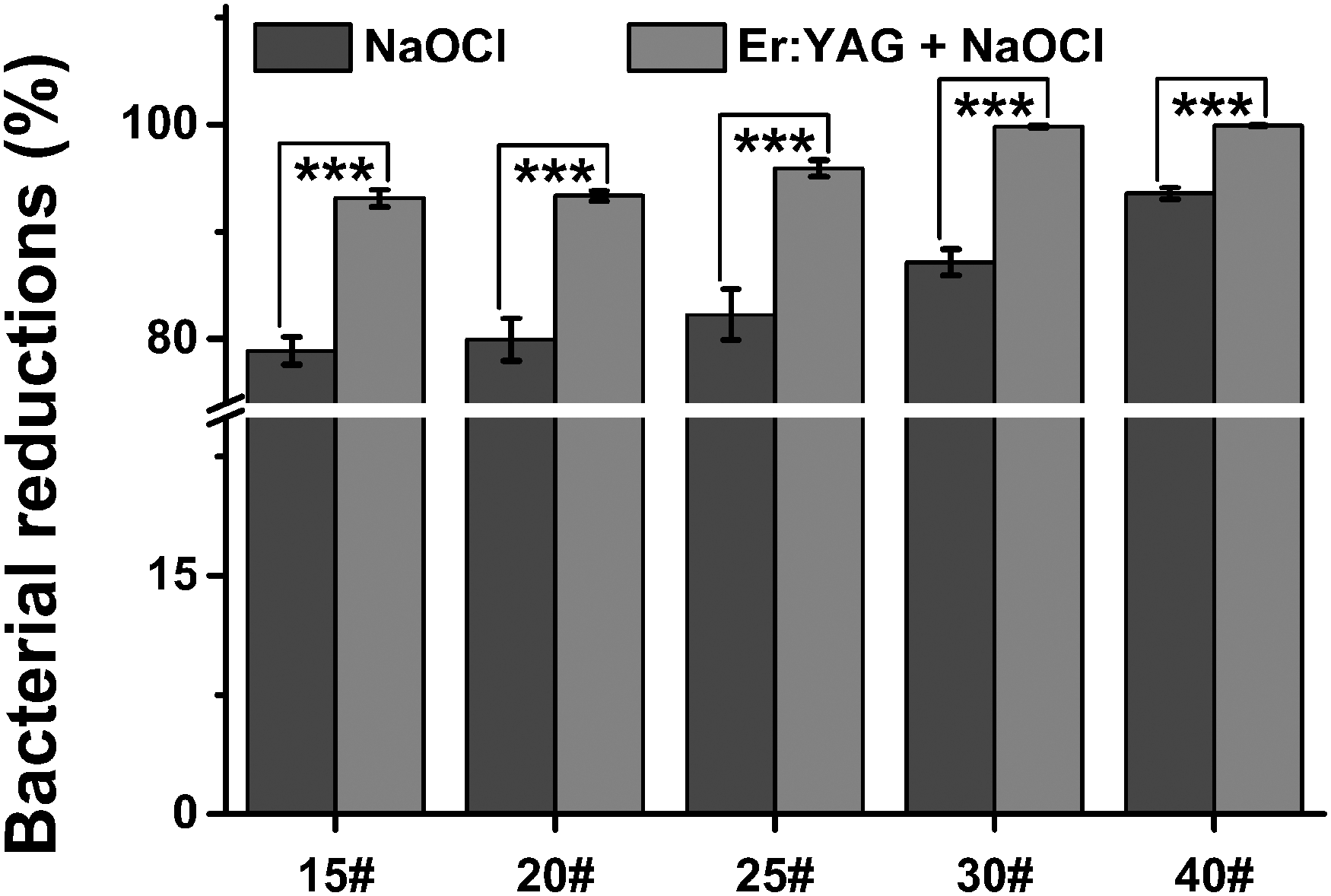
Bacterial reductions after treatments of Er:YAG + NaOCl or NaOCl alone at different apical terminal working widths. ***p < 0.001. Er:YAG, Erbium:Yttrium Aluminum Garnet; NaOCl, sodium hypochlorite.
Under the condition of the same ATWW and the output power of the Er:YAG laser, the disinfection efficacy of the Er:YAG + NaOCl increased with radiation time (Fig. 3A). The maximum bacterial reduction was 96.1% when the Er:YAG laser was activated for 60 sec.
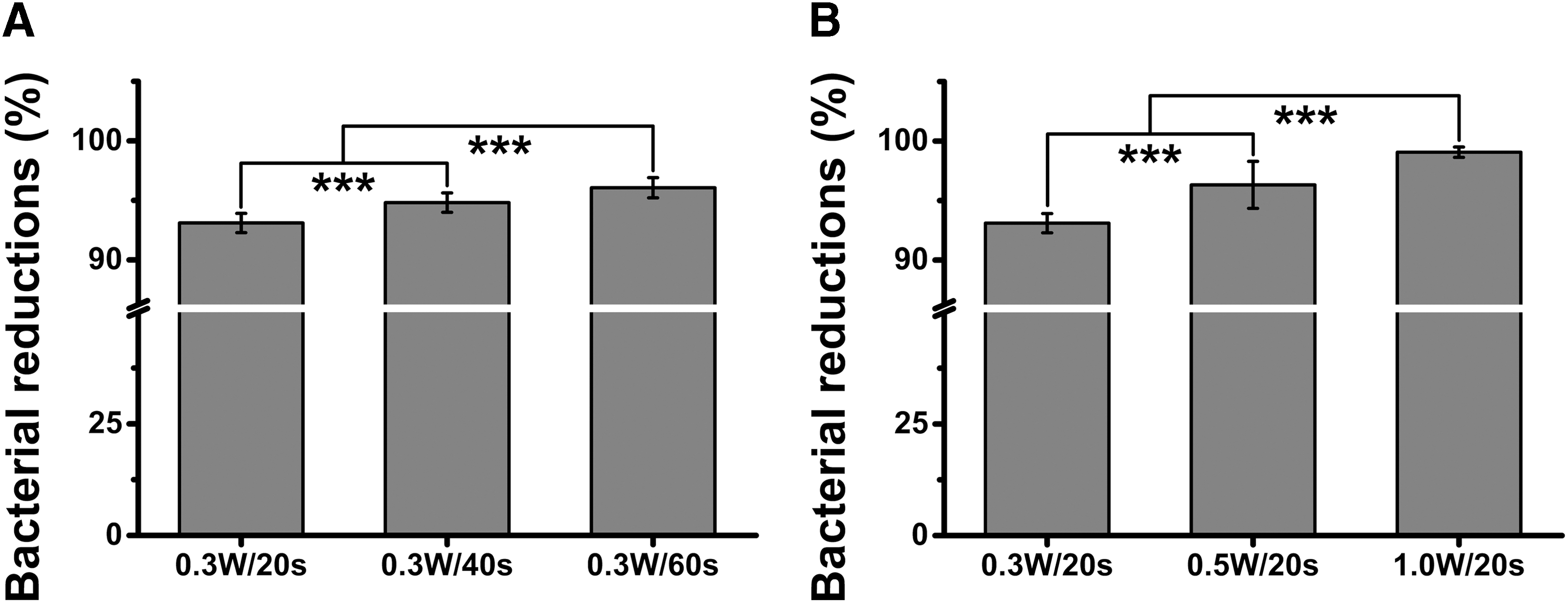
Bacterial reductions after treatments of Er:YAG + NaOCl at different output powers and radiation times of the Er:YAG laser. ***p < 0.001.
The disinfection efficacy of Er:YAG + NaOCl also increased with the output power of the Er:YAG laser. When the ATWW and radiation time were fixed at #15 and 20 sec, the maximum bacterial reduction was 99.2% at an output power of 1.0 W (Fig. 3B).
Discussion
In this study, we evaluated the potential of the Er:YAG + NaOCl for MIE. Our results indicated that the Er:YAG laser significantly enhanced the disinfection efficacy of NaOCl irrigation. To achieve a similar disinfection efficacy, the Er:YAG + NaOCl allowed a smaller ATWW than the NaOCl alone did. In addition, the disinfection efficacy of the Er:YAG + NaOCl could be improved by increasing the output power and radiation time of the Er:YAG laser. This confirmed our hypotheses.
MIE was recently developed to conserve the maximum structural integrity of dental tissues and therefore preserving the longevity of an endodontically treated tooth. 11 Based on the concept of MIE, root canals should be prepared as minimally as possible to preserve healthy tooth structure. However, according to current techniques, the root canals are usually prepared to large ATWW of 45–70# and even 80# to achieve an effective disinfection effect. 8,23,24 The treatment of large ATWW increased the risk of root fracture due to the loss of dental tissues. 9,10,25
Lasers have been proposed as an alternative to the conventional approach of cleaning and disinfecting, or as an adjuvant to the conventional chemomechanical treatment to enhance debridement and disinfection. 26 It was reported that the Er:YAG laser significantly enhanced the disinfection efficacy of NaOCl for endodontic treatment. 20,21,27 The mechanism of the Er:YAG laser for the root canal treatment is attributed to vapor bubble expansion and the implosion with secondary cavitation effects that induce high-speed fluid motion in and out of the canal. 22,28 The collapsed shock waves and acoustic streaming of the fluid produced during the process of laser-assisted irrigation put a large shear stress on the root canal wall. 29,30 The shear stress facilitates the penetration of NaOCl into the deeper dentin layers to perform its bactericidal effect.
It has been well documented that the Er:YAG laser irradiation using PIPS significantly improved the disinfection efficacy of NaOCl irrigation. Irrigation with NaOCl (5%) and EDTA (17%) activated by the Er:YAG laser was effective in eradicating E. faecalis from extracted canals, 31 and the Er:YAG + NaOCl using PIPS was effective in removing both E. faecalis and smear layer from canals. 32,33 In this study, as shown in Fig. 2, only 78.9% of the bacteria were eliminated in the 15#/NaOCl group, while 93.1% of the bacteria were eliminated in the 15#/NaOCl + Er:YAG group. In fact, the disinfection efficacy of the15#/NaOCl + Er:YAG group was similar to that of the 40#/NaOCl group (p > 0.05). In other words, under the condition of the same disinfection efficacy, the addition of Er:YAG laser to NaOCl allowed the use of much smaller ATWW than the NaOCl alone. When fixing the ATWW at #15, the disinfection efficacy of Er:YAG + NaOCl increased with the output power and radiation time of the Er:YAG laser. Increasing the output power was more effective than the radiation time in improving the disinfection efficacy. A maximum bacterial reduction of 99.2% was reached when the Er:YAG laser was activated at 1.0 W for 20 sec. All these results indicated that the Er:YAG + NaOCl allowed a less apical preparation to reach an effective disinfection effect, which may prevent the excess loss of dental tissues, conserve the structural integrity of endodontically treated teeth, and therefore be a promising procedure for MIE.
A major concern of LAI is the thermal injury to dentin and periodontal tissues. To reduce the risk of thermal damage to those tissues, a super-short pulse working mode was used, and a coolant (i.e., NS) and irrigant (i.e., NaOCl) were included to suppress the temperature increase during the Er:YAG laser treatment. In addition, a short treatment time (e.g., 20 sec) was used to reduce thermal stress to the radicular dentin and the periodontium. According to previous studies, the emission protocols of the Er:YAG laser tested in this study were safe to periodontal tissues. 15,34 In case of damage to periapical tissues, the apical extrusion of endodontic irrigants should be taken into consideration when choosing a system for activated irrigation. It has been reported that LAI with the Er:YAG laser demonstrated significantly more potential for apical extrusion than the EndoVac system, although the size of canal preparation showed no effect on the extent of apical extrusion. 35 More investigations of the apical extrusion of LAI with the Er:YAG laser need to be explored.
In this study, single-rooted teeth with straight root canals were selected so that standard quantification analyses could be performed. To further understand the clinical disinfection efficacy of Er:YAG + NaOCl, future work will include the evaluation of multiple-rooted teeth and curved root canals. In addition, taper 0.04 was tested in this study, which is the smallest taper among the most popular tapers (0.04, 0.06, and 0.08) currently used in the clinic. Evaluations of the disinfection efficacy of Er:YAG + NaOCl in root canals prepared with newly developed instruments of taper 0.02 will also be explored in our future work.
Conclusions
Under the conditions of this study, the Er:YAG + NaOCl reached an effective disinfection result at a small ATWW. The 15#/Er:YAG + NaOCl with Er:YAG laser irradiation at 1.0 W for 20 sec reached an effective bacterial reduction of 99.2% and may be considered a promising procedure for MIE.
Highlights
• Disinfection efficacy of NaOCl irrigation increased as the ATWW was increased.
• Disinfection efficacy of Er:YAG laser-activated NaOCl irrigation (Er:YAG + NaOCl) increased as the ATWW was increased.
• Er:YAG laser enhanced significantly the disinfection efficacy of NaOCl irrigation.
• Er:YAG + NaOCl showed a similar disinfection effect to NaOCl alone at a smaller ATWW.
• The use of Er:YAG laser could reduce the apical preparation.
• Er:YAG + NaOCl is a promising procedure for minimally invasive endodontics.
Footnotes
Acknowledgments
This research was supported by grants from the National Natural Science Foundation of China (No. 81670975) and the Innovation Team of the Ministry of Education (No. IRT13051).
Author Disclosure Statement
No competing financial interests exist.