
Abstract
Introduction
P
De Freitas and Hamblin 2 state that LLLT refers to the use of light in the red or near-infrared region (NIR) with wavelength usually in the range from 600 to 700 nm and from 780 to 1100 nm. A wavelength range between 700 and 780 nm has been found to be ineffective as it coincides with a trough in the absorption spectrum of cytochrome c oxidase. 3 Moreover, red/NIR wavelengths are chosen because the penetration through tissue is maximal in this range, due to lower scattering and absorption by tissue chromophores.
The laser or light emitting diode (LED) used for this application typically has an irradiance or power density between 5 and 50 mW/cm2. Continuous wave or gated energy has been used at a relatively low energy density (0.04 − 50 J/cm2), and output power can vary widely from 1 to 500 mW. 2
In PBM, energy density or irradiance is lower than in other laser uses such as ablation and thermal coagulation. 4
Application of incorrect parameters of fluence (J/cm2), irradiance (mW/cm2), and delivery time or repetition rate can lead to ineffective treatment. A biphasic dose response or hormesis phenomenon follows the Arndt-Schultz Law, which states that weak stimuli slightly accelerate vital activity; stronger stimuli raise it further until a peak is reached; and even stronger stimuli suppress it until a negative response is achieved. 5 Studies suggest that the biological effects of laser energy and LED energy are the same when the wavelength is properly chosen. 6
Phototherapy at the cellular level can be classified into primary, secondary, and tertiary light-induced effects. 7,8
-A primary effect is restricted to photon absorption. Photons emitted from the laser reach the mitochondria of cells, are absorbed by chromophores (cytochrome, porphyrins, and flavoproteins), and are finally converted into chemical energy in the cells. A cascade of signals between mitochondria, nucleus, and oxidative metabolism leads to an increase in adenosine triphosphate (ATP) production, causing pain relief and wound healing. 9
– A secondary effect is the result of photonic stimulation, amplifying the primary effect and increasing calcium production.
– A tertiary effect is systemic and occurs at a distance from the stimulus. 8 Thus, laser energy applied to one lesion can stimulate the healing of both the treated lesion and other lesions at a distant location.
There is no agreement for a mechanism of action of PBM. However, a molecular mechanism of PBM proposed by De Freitas and Hamblin in 2016 is attractive. 2
Molecular mechanism of PBM
Cytochrome c oxidase (Complex IV of the mitochondrial membrane) is the first photo-acceptor for red and NIR wavelengths. 1 The absorption spectra for light that produce a biological response are very similar to the absorption spectra of cytochrome c oxidase. 3 COX is the terminal enzyme of the electron transport chain mediating the electron transfer from cytochrome c to molecular oxygen. Ox acts as a photo-acceptor and transducer of photo signals in the red and NIR regions of the light spectrum. 2 PBM increases the mitochondrial membrane potential, increases the level of adenosine triphosphate, c-AMP (cyclic adenosine monophosphate), and ROS (reactive oxygen species). In addition, PBM increases the availability of electrons for the reduction of molecular oxygen in the catalytic center of COX.
This suggests that light is absorbed by the chromophore (cytochrome c oxidase), followed by a photo-dissociation of NO (nitric oxide) from COX. As a consequence, the activity of the mitochondria is inhibited and reversed due to the excessive NO binding (NO photodissociates from the heme iron and copper center of COX). 2
The mitochondrial alteration function allows the oxygen to come to the site and, because there is communication between mitochondria and nucleus, this will cause an increase in enzymatic activity, electron transport, and ATP production due to alteration of mitochondrial activity. 2
Numerous signaling effects occur due to the change in mitochondria, including: an increase in ATP, an alteration in CA concentration, and an increase in c-AMP as a direct consequence of the rise in ROS that leads to the activation of NF-κB. (NF-κB has an important function in the nucleus as it combines with the DNA and the production of NO.)
Activation of transcription factors
(1) NF-κB is a protein complex that is responsible for DNA transcription. An increase in NF-κB leads to enhanced cell transcription that leads to cell proliferation and reduced cell death. 2
(2) RANKL (receptor activator of nuclear factor Kappa-B ligand) is a transmembrane protein that is involved in bone regeneration and remodeling, and it also acts as a ligand for osteoprotegerin (OPG). OPG is a secretory soluble receptor and an inhibitor of the RANK receptor.
The RANKL/OPG ratio is an important factor that is used for studying or determining whether bone is removed or formed. During the remodeling process, there is an increase in RANKL production by osteoblasts, which bind to RANK receptors and cause osteoclast progenitor expansion, activation, and fusion into multinucleated osteoclasts.
(3) Hypoxia-inducible factor (HIF-1α): This type of protein is involved in cellular adaptation to hypoxia. It is oxygen dependent and, during PBM, this protein is rapidly activated through two mechanisms. First, it is possible that this protein is mediated by MarK (mitogen-activated protein kinase) and PI3K (phosphatidyinositol 3 kinase). Second, light activation of CX causes oxygen depletion followed by a rapid activation of HIF-1α.
(4) AKt/GSK3β/β: Protein Kinase is activated by PBM, causing a decrease in the activity of GsK 3 (glycogen synthase kinase 3) and inhibiting Bax translocation and the pro-survival action of β catenin.
Other transcription factors that are activated by LLLT are as follows:
(5) AKt/m TOR/cycling pathways F-ERK/FOXM1G-PPaR: H-RUNX2
The effect of LLLT on bone regeneration during osseointegration and bone graft is still not clear. Despite many positive reports of in vitro and in vivo studies and more than 50 randomized clinical trials claiming a positive effect of PBM, many reports found no significant laser effect.
The aim of this study was to evaluate studies correlating PBM and bone regeneration during either osseointegration or bone graft and to assess parameters that produce positive results based on dose and output power used.
Materials and Methods
The present systematic review was conducted by following PRISM (Preferred Reporting Items of Systematic reviews and Meta-analysis).
Research strategy for article identification
Research was conducted on the following electronic databases: Springer, PubMed, Google Scholar, and Cochrane Databases.
Keywords used: LLLT and bone regeneration, LLLT, PBM, LLLT and osseointegration, LLLT and bone graft, and LLLT and cells.
After collecting the data, the titles, abstract, and conclusion were read and unrelated and obviously biased articles were excluded. Also, all case reports and literature reviews were excluded. Only studies dating from 2007 to 2016 were included. Reasons for exclusion are shown in Table 3.
Evaluations of articles were performed by two reviewers independently. Fig. 1 shows how the final group of 19 studies was selected.
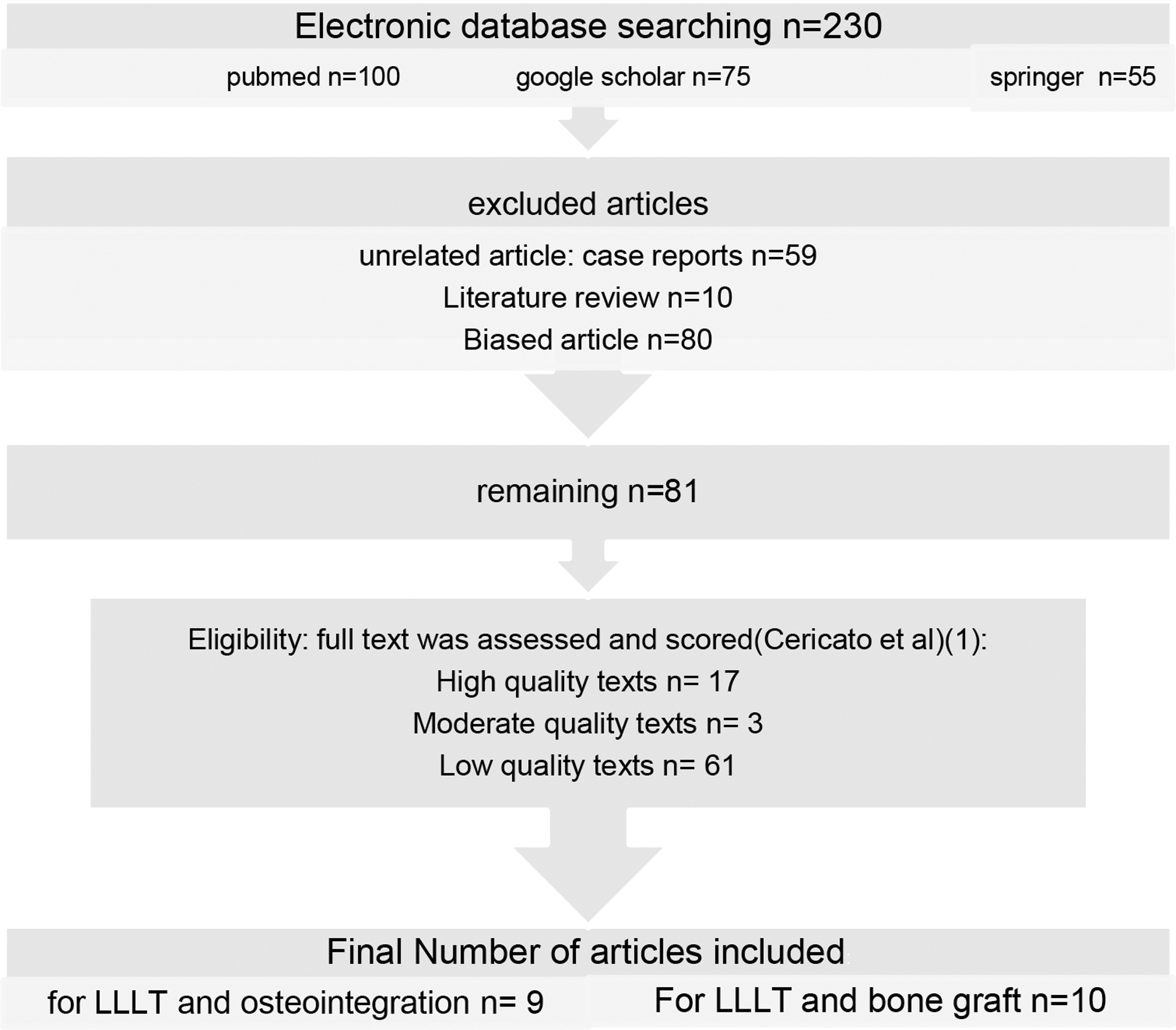
Flowchart of article selection.
Assessment of the studies
After obtaining the full texts, all articles were evaluated and scored by following the checklist described in Table 1. Articles with scores from 0 to 5 points were considered to be of a low quality and were excluded; those with scores from 6 to 8 were considered to be of a moderate quality; and those with scores from 9 to 11 were considered to be of a high quality. Main characteristics of included studies are shown in Table 2.
Introduction to LLLT and Osseointegration
Osseointegration is a direct structural and functional contact between a loaded implant surface and bone at the light microscopic level. 10 An implant is osseointegrated when there is an absence of progressive movement between the bone and the implant. 11 Early failure of the implant occurs before placement of the restoration. Possible reasons are improper wound healing, infection, or mobility. Late failure occurs after prosthetic treatment and may be due to overloading or infection. 12
The effect of LLLT on osseointegration is still controversial. Some studies assert a positive contribution of laser energy on bone, whereas others claim no effect. All the studies were divided into four groups: High dose/low power, low dose/high power, high dose/high power, and low dose/low power. More than 16 J/cm2 per session is considered high dose, whereas more than 35 mW is considered high power.
Each study will be described in some detail since parameters and research protocols varied widely. Knowledge of these differences is vital to understanding the summary tables.
Review of LLLT and osseointegration
Lopes et al. 13 assessed through Raman spectroscopy the effect of diode laser 830 nm on the osseointegration of implants in 14 rabbits: All received titanium implants with 6 acting as controls, whereas 8 were irradiated with laser energy by using the following parameters: 10 mW, 21.5 J/cm2 per point, 86 J per session, spot area 0.0028 cm2, and seven sessions at 48 h intervals. The animals were sacrificed at 15, 30, and 45 days and were prepared for Raman spectroscopy and scanning electron microscopy (SEM). Results showed a significant difference in the concentration of calcium hydroxyapatite CHAin irradiated and the control group (p = 0.001). It was concluded that infrared laser irradiation improves bone healing.
De Almeida et al. 14 performed an in vitro study in rats to evaluate the influence of LLLT on osseointegration. Titanium implants were placed in the tibia of 60 rats. Of these, 30 underwent laser treatment before implant placement by using a GaAlAs (Gallium-Aluminum-Arsenide) laser: 660 nm, 35 mW, CW, and energy density of 4.9 J/cm2, for 4 sec. Ten animals from each group were euthanized after 15, 30, and 60 days. Histological and immunohistochemical analysis was performed by using optical microscopy. Histological and quantitative analysis shows an increased amount of multinucleated tartrate-resistant acid phosphatase-positive cells in the lased group (p < 0.05). It was concluded that LLLT accelerated the osseointegration via stimulation of both osteoblastic and osteoclastic activity.
Gomes et al. 15 evaluated the effect of LLLT on peri-implant healing. A total of 32 rabbits received immediate dental implantation after mandibular incisor extraction. The animals were divided into four groups: a control group or one of three LLLT groups at different doses: 5, 10, and 20 J/cm2 by using a semiconductor GaAlAs 830 nm, 50 mW every 48 h for 13 days for a total of five sessions. Resonance frequency analysis (RFA) and SEM showed that the bone implant contact (BIC) was significantly higher in the 20 J/cm2 group, with significant improvement in implant stability quotient (ISQ). Bone area values were better in the group receiving 10 J/cm2 (p = 0.036) and 20 J/cm2 (p = 0.0016).
Mandic et al., 16 using a split-mouth design, placed self-tapping implants in 12 patients to investigate the influence of LLLT osseointegration on self-tapping implants placed into low-density bone. For each patient, one jaw randomly received LLLT and the other side of the same patient was treated as a placebo. The laser used was a 637 nm GaAlAs, with an output power of 40 mW, CW, and a total irradiation of 6.26 J/cm2 per implant. Laser treatment was performed immediately after implant placement and repeated every day for 7 days. The outcome was assessed for implant stability, early implant success, and ALP (alkaline phosphatase) weekly from the first to the sixth week. Throughout this period, irradiated implants achieved higher stability than nonirradiated ones. However, the difference was not significant until the fifth postoperative week.
Maluf et al. 17 randomly divided mice into control and laser groups. In the laser group, the bone-implant interface was subjected to LLLT by using a semiconductor laser 795 nm, CW, power of 120 mW, 8 J/cm2 per point, six laser applications with an interval of 2 days, and a total dose of 48 J/cm2. The result suggested faster and better bone-implant integration than the control.
Menezes et al. 18 assessed the PBM action of LLLT on peri-implant bone healing of dental implants in the tibia of dogs. Ten dogs served as controls and received implants only in the tibia, with the other 10 dogs receiving implants with laser therapy: GaAlAs 830 nm, power of 40 mW, irradiation interval of 48 h for 2 weeks, 4 J/cm2 at five points, CW, Thera laser, which applied 20 J/cm2 per session distributed at 5 points of 4 J/cm2, and for a total dose of 140 J/cm2. After 15 and 30 days, all the specimens were removed and submitted to EDXRF tests (energy-dispersive X-ray fluorescence) to assess the concentration of calcium. At 30 days, the lased group showed a significant increase in calcium concentration compared with the control group (p < 0.05).
Marques et al. 19 proposed and compared a new protocol of LLLT for bone regeneration on 45 rats. After creating a bone defect of 8 mm in the skull, they divided the animals into three groups of 15 rats. Group I was treated with LLLT: transcutaneous applications into four points around the defect, fluence 16 J/cm2, power of 50 mW, duration of application 9 sec, and 1 mm distance, applied every 48 h for 15 days. Group II received LLLT by using three applications—during the surgery before closing with sutures, directly into the defect in four points (same points as Group I), and directly to the skin. The parameters used were as follows: fluence 3.7 J/cm2, power 50 mW, and time of application 3 sec; then, two other applications were made after 48 and 96 h transcutaneously. Group III was the control group and was not submitted to laser irradiation. Histomorphometric analysis, an immunohistochemistry study, and microscopic evaluation showed significant differences between the treated and untreated groups. It was concluded that laser irradiation supports bone regeneration, and that LLLT works better in the early stages of bone formation.
Garcia et al. 20 performed a randomized clinical study to assess the LLLT effect on implant stability by means of RFA. Thirty implants were distributed bilaterally in the mandible of eight patients. In each patient, one side acted as a control group not receiving laser irradiation. The other group received GaAlAs 830 nm (Thera laser), 86 mW, 0.25 J, 92 J/cm2, energy of 0.25 J per point, contact mode, total energy of irradiation 5 J, 3 sec/point at 20 points, and spot size of 0.0028 cm2. Irradiation was initiated immediately after implant placement and repeated every 48 h for 14 days. RFA was used to determine the stability of dental implants. After 10 days, the increase in ISQ value in the irradiated group was not significantly different than the control. It was concluded that the laser has little impact macroscopically and that LLLT did not have any effect on the stability of implants.
Kim et al. 21 investigated the LLLT effect on healing and attachment of titanium implant in the bone. Thirteen rabbits received femur implantation and were divided into control and LLLT groups by using GaAlAs 808 nm, with 100 mW output power, 830 mW/cm2, and 60 sec, applied to the tissue surrounding the implants daily for 1 week. Rabbits were sacrificed in the 6th (six rabbits) and 12th weeks. Histopathologic results showed that the LLLT group, after 12 weeks, had more bone matrix and collagen around implants. Histomorphometric analysis showed that there was no significant difference in BIC between the groups, although the laser group showed higher average values. Torque tests showed significantly higher removal torque values for the lased group compared with the control (p ≤ 0.05), but only after 12 weeks. Likewise, ISQ values were significantly different between the two groups only after 12 weeks. All tests showed no statistically significant differences after 6 weeks. It was concluded that LLLT might promote implant osseointegration, but there was no statistically significant difference.
Results
Out of nine articles, using diode laser, eight found positive results with significant difference (p < 0.05). This review found, in Table 4, that when high fluence (greater than16 J/cm2) was combined with low power (less than 35 mW) and when high power (greater than 35 mW) was combined with low fluence (less than 16 J/cm2) per session, all studies showed positive results. However, when high fluence (greater than16 J/cm2) was combined with high power (greater than 35 mW), the results showed no significant difference between the irradiated and control groups. 14,15
BIC, bone implant contact; EDXRF, energy-dispersive X-ray fluorescence; ISQ, implant stability quotient; TRAP, tartrate-resistant acid phosphatase.
Altan et al. 22 concluded that when using 50 mW, 20 J/cm2 on osseous expansion, treatment was not effective whereas when using 50 mW, 5 or 6.4 J/cm2 the results showed a significant effect.
It must be noted that, using the exclusion criteria of Cericato et al., 6 there are no studies of either high or moderate quality that explore the low power (<35 mW) low fluence (<16 J/cm2) scenario. This shortcoming prevents drawing conclusions under these conditions.
Other studies that did not meet inclusion criteria provide further insight into the possible effects of very divergent parameters.
Schwartz-Filho et al. 23 did not find effective results when using 35 mW/cm2 power density and 25, 77, and 135 J/cm2 fluence. Very low energy density (less than 1 J/cm2) combined with high power density was also not effective. 24
Mayer et al. 25 as well as Massoti et al. 26 found that 20 J/cm2, 50 mW showed better results compared with 5 and 10 J/cm2, which contradicts the conclusion of this article. However, their spot area of 0.0028 cm2 was much different than other studies, which could affect results.
It is suggested that LLLT increases the cellular metabolism. Photonic energy is transmitted to the nucleus, resulting in DNA and RNA synthesis, which causes protein synthesis. This could lead to bone neo-formation and resorption, which increase osseointegration.
Introduction to LLLT and Bone Graft
Bone loss is a major problem in medical and dental specialties and may be caused by physiologic, pathologic, or iatrogenic conditions. Although bone has a regenerative capacity, this capacity is limited if there is mechanical instability, deficient blood supply, or competition with highly proliferative tissue. As a consequence, a bone defect may be created that makes prosthetic rehabilitation impossible. 27
There are different methods to overcome this problem, including the use of a graft. This may be autologous bone, a xenograft, or the combination of graft material with an overlying membrane in guided bone regeneration. 28
An investigation of the influence of PBM on the success of bone grafting procedures was performed. As earlier, all studies were divided into four groups: high dose/low power, high power/low dose, high dose/high power, and low dose/low power. More than 16 J/cm2 per session is considered high dose, whereas more than 35 mW is considered high power.
Again, each study will be described in some detail since parameters and research protocols varied widely. Knowledge of these differences is vital to understanding the summary tables.
Review of LLLT and bone graft
Rasouli Ghahroudi et al. 29 conducted a double-blind experiment studying the effect of LLLT and Bio-Oss graft material on the osteogenesis process in rabbit calvarium. They prepared 10 mm identical cranio-caudal incisions and then created four identical circular defects on each rabbit. One defect was used as an untreated control, a second was filled with Bio-Oss, a third was treated with laser irradiation only using diode laser 810 nm, 300 mW, CW, and 4 J/cm2, and a fourth was treated with Bio-Oss and laser by using the same laser parameters.
In histological and histomorphometrical evaluation, after 4 weeks, the control group and the “Bio-Oss only” group showed the most inflammation. The “laser only” group showed the least inflammation, and the combination of “laser with Bio-Oss” ranked between the previous groups. After 8 weeks, the control group demonstrated the greatest inflammation and the laser with Bio-Oss was next in order.
The “laser plus Bio-Oss” group showed greater new bone formation than the “laser only” group or the “Bio-Oss only” group.
Pinheriro et al. 30 conducted an in vitro study on 24 rats that were divided into three groups. After exposing the femur, they created 3 mm2 cavities in the bone. For group I, the periosteum was repositioned and sutured. In groups II and III, the cavities were filled with inorganic bovine bone and sutured. Group III was submitted to seven sessions of LLLT at 48 h intervals (wavelength 830 nm, 40 mW, CW). A dose of 4 J/cm2 was applied, giving a total dose of 16 J/cm2 to four points around the cavities. Animals were killed after 15, 20, and 30 days; samples were taken, decalcified with nitric acid, and stained with heat shock factor (HSF). Results of the study showed that new bone formation was seen after 21 days in groups II and III and collagen fiber was seen in group III after 30 days.
In this study, the major finding was the increased amount of collagen fiber in the lased group, which indicated a positive effect of LLLT on bone healing.
Soares et al. 31 conducted a study on rabbits to assess the influence of LLLT on BIC and bone volume around implants inserted in a block of bovine xenograft or autologous bone graft. They used 780 nm, 4 J/cm2 per point, 0.5 cm2, repeated every other day for 2 weeks. The result showed a higher percentage of new bone formation in the autograft-irradiated groups in comparison to irradiated xenograft without a significant difference (p > 0.05). A comparison of the irradiated and nonirradiated grafts showed that the irradiated group increased the formation of bone on both types of graft, with a significant difference (p = 0.05).
de Vasconcellos et al. 32 assessed the effect of the bone repair process with titanium scaffold on rat femur. Fifty-six rats were divided as follows: Group1-SHAM (simulated ovariectomy) animals received the titanium scaffold; Group2-SHAM animals received scaffold and were subjected to LLLT; Group3-ovariectomized animals received scaffold; and Group4-ovariectomized animals received scaffold and LLLT (the ovariectomized rats showed bone characteristics similar to those found in postmenopausal woman). The LLLT source was GaAlAs 780 nm, CW, through an optic fiber, 40 mW, duration of 100 sec, immediately after surgery was repeated every 48 h for 6 weeks, spot diameter of 0.69 cm, and 4 J/cm2 applied to four points for a total of 16 J/cm2 per session. Results showed that statistically greater new bone formation occurred in the irradiated group. It was concluded that LLLT improves bone repair within a titanium scaffold in both ovariectomized and healthy rats.
Carneiro et al. 33 assessed the effect of using an AlGaAs 830 nm laser on the repair of surgical defects created in the femur of rats. Forty-eight rats were divided into four groups of 12 each: In the control group, the periosteum was repositioned and sutured in place with no other treatment. The other three groups had this same initial treatment. The second group had laser only applied, the third group received hydroxyapatite+ membrane, and the fourth group received HA+ membrane+ laser treatment. Both laser groups had energy applied at 40 mW, CW, 16 J/cm2 per session, four points of 4 J/cm2, and spot diameter of 0.6 mm. Laser irradiation was repeated seven times every 48 h. Rats were sacrificed after 15, 21, and 30 days. It was found that, after 15 and 21 days, defects submitted to laser therapy healed more quickly, but at 30 days, the level of repair was similar. Laser therapy associated with hydroxyapatite and a biological membrane increased the biomodulation effect on the bone.
Marquez-Martinez et al. 34 assessed the effect of PBM on the repair of surgical defects in the femur of rats. Twenty-four rats were divided into three groups of eight each. The first was used as a control, the second received only bovine bone graft, and the third received graft with PBM by using GaAlAs 830 nm, 40 mW, CW, 4 J/cm2 applied to four points for a total of 16 J/cm2 per session, and spot diameter of 0.6 mm for four sessions. Animals were killed on days 15, 21, and 30. A histological exam showed an increased amount of collagen fiber, osteoblastic activity, and bone trabeculae formation on the 30th day in the lased group. It was concluded that there was a positive effect on bone healing with the use of PBM.
Gerbi et al. 35 assessed the effect of laser PBM on the repair of surgical defects; 48 rats were divided into four groups of 12 each: The first one was used as a control, the second group received LLLT, the third group received bone morphogenic proteins (BMPs)+organic bovine bone graft, and the fourth group received BMPs+organic bovine bone+LLLT. The laser used was 830 nm, 40 mW, CW, 0.6 mm fiber diameter, 16 J/cm2 per session divided over four points, and seven irradiations every 48 h. The results, assessed histologically after 15, 21, and 30 days, showed an increased deposition of collagen fiber (at 15 and 21 days) and an increased amount of organized bone trabeculae at 30 days in the irradiated groups. It was concluded that combining LLLT with BMPs and bovine bone increased the biomodulating effect of the laser.
Pinheiro et al. 36 histologically studied the effect of LLLT on the repair of defects created surgically on 54 rat femurs. Rats were divided into four groups: The first group served as the control, the second group received LLLT, the third group received HA, guided bone regeneration, and the fourth group received HA, GBR, and LLLT.
The irradiated group was subject to GaAlAs, 830 nm, 40 mW, CW, and spot diameter 0.6 mm, immediately after placing the suture; 4 J/cm2 per point; session dose was 16 J/cm2; and total treatment dose 112 J/cm2 was applied every other day for 15 days. A histological study on day 15 showed that, in the control group, the defect was filled with medullary tissue without osteoblastic activity. At the end of the experiment, the cortical plate was still thinner than the area not being operated. The irradiated group LLLT at day 15 was filled with medullary tissue, but it progressed faster from day 15 until day 21 when new bone formation was seen. When HA and GBR were used, cortical repair, spongy bone, and giant cells were seen at day 15; in group 4 (HA, GBR, and LLLT), cortical repair and a thin plate at the wounded site with spongy bone, osteoblastic activity, and giant cells were seen. At the end of the experiment, for the entire treated group, the cortical plate was similar to the area not being operated. It was concluded that LLLT could be effective in early wound healing.
Fekrazad et al. 37 evaluated the effect of LLLT and mesenchymal stem cells on bone regeneration. Fifty-eight rabbits were included and divided into four groups: C = control, L = LLLT, Sc = filled with mesenchymal cells, and SCL = LLLT+mesenchymal cells. The laser application was initiated the day of the surgery and continued every other day for 3 weeks by using GaAlAs 810 nm, CW, 200 mW, 4 J/cm2, 0.2 W/cm2, spot size of 1 cm2, a distance of 0.5 cm, and 20 sec of treatment. All animals were sacrificed and subjected to histological and histomorphometric analysis at 21 days. Results showed a statistically significant increase (p < 0.05) of new bone formation in the group treated with LLLT compared with the two other experimental groups. When comparing the other three groups (C, SC, and SCL), no significant difference between them (p > 0.05) was found. Histological evaluation showed that groups SC and SCL demonstrated a significantly higher level of inflammation compared with the other groups. It was concluded that combining LLLT with mesenchymal cells does not have a synergistic effect on bone formation.
Kim et al. 38 investigated the effect of high-power pulsed laser on bone repair, by using an NdYAG Q-switched pulsed laser. Using 14 rats and 14 rabbits, bilateral defects (5 m rats) and (8 mm rabbits) were created along the sagittal suture. All the rabbits were implanted by using a collagen scaffold and divided into two groups: One group was subjected to 0.75 W output power; the other was subjected to 3 W, by using the same fluence (344 J/cm2). For the 14 rats, bilateral defects were either left empty (n = 7) or implanted by using a collagen scaffold (n = 7). All were irradiated at the same fluence (344 J/cm2) and 0.75 W output power. The Q-switched pulsed NdYAG was applied with high peak power, 320 μm diameter, nonfocused at a distance of 1–2 cm, and with a repetition rate of 100 pulses per second every 2 days for 2 weeks. The spot diameter matched defect size (rats = 5 mm, rabbits = 8 mm). Histomorphometric analysis after 4 weeks showed that the NdYAG laser, using high-intensity pulse, high-power laser irradiation was effective in bone formation in rats when the defects were left empty or filled. In rabbits, both 0.75 and 3 W enhanced bone formation, with no significant difference between the two power levels.
Results
Table 5 summarizes the effect of laser irradiation on bone grafting. Most of these studies used 4 J/cm2 per point into four points and found a positive response. One study using higher dose and irradiance did not find a significant effect between the control and laser groups. Finally, one study used Nd: YAG rather than diode laser irradiation.
LLLT, low-level laser therapy.
Studies showed that when combining LLLT with bone graft, the results were much better than when using graft alone or irradiation alone but the improved healing was more effective at the early stage of the healing process.
Discussion
The parameters of most importance in PBM are power density (irradiance) measured in watts/cm2 and energy density (fluence) measured in J/cm2. Most of the studies discussed here and, indeed, most seen in research literature are based on the misleading parameter of laser output in watts. Depending on the area irradiated by this beam of photons, the power density and the cellular effect produced will be very different.
As an example, one watt delivered through a 400 μm diameter optical fiber will produce a power density of 796 W/cm2 whereas the same one watt delivered through a 8 mm diameter therapy handpiece will produce a power density of only 2 W/cm2.
Energy density is often reported in research literature, but the spot area at the tissue is routinely omitted. This error makes it impossible to verify the given findings or to see how the vital energy density information was calculated. Inconsistency in reporting these parameters is a major source of contradictory research outcomes, and it has done much to slow the understanding of any PBM effect.
It must be noted that, using the established exclusion criteria of Cericato et al., there are no studies of either high or moderate quality that explore some application scenarios. Neither low power (<35 mW)/low fluence (<16 J/cm2) nor low power (<35 mW)/high fluence (>16 J/cm2) studies were found. This shortcoming prevents drawing any strong conclusions.
Conclusions
On reviewing the studies evaluated here, it is apparent that each study has subtle or major differences in experimental protocol that could have a significant effect on outcome. The complete reading of any study is vital to evaluating its significance since summary tables can be misleading.
According to this review, we can conclude that: • LLLT increases cellular metabolism. • Photonic energy is transmitted to the nucleus, resulting in DNA and RNA synthesis, which causes protein synthesis. This will lead to bone neo-formation and resorption, which increase osseointegration. • There is no fixed value of dose that produces positive PBM response and bone regeneration. • A higher dose combined with low power or a low dose combined with high power appears to produce a positive result of PBM. • Higher dose combined with high power may have an inhibitory effect on PBM. • Proper reporting of vital laser parameters is essential to understanding the effects of PBM on both soft tissue and bone.
Footnotes
Acknowledgments
This article has received no financial assistance or grants from any organization or individual.
Author Disclosure Statement
No competing financial interests exist.