
Abstract
Introduction
G
As a type of periodontal disease, it is a consequence of an imbalance between a wide range of microorganisms, the host response, and modifying factors. 2,3 The microbial biofilm is an important protagonist in the etiology and evolution of GAgP. 4 Given the important role played by the biofilm, periodontal therapy should be aimed at preventing the inflammatory response by decreasing and eliminating these microbial active factors. 5
Nonsurgical periodontal treatment, one of the first suggested treatments for the management of periodontal disease, is characterized by the elimination of the pathogenic biofilm using hand and ultrasonic instruments. 6 Although systematic and critical reviews have shown an improvement in clinical periodontal parameters, 7,8 it was shown that conventional therapy through scaling and root planing (SRP) does not completely remove periodontopathogens, particularly in mild and deep periodontal tissues, 9,10 and can therefore stimulate infective events. 11
For many years, diode laser therapy has been recommended as an additional or supplementary protocol to treat periodontal disease. 12 In subjects with GAgP, the additional use of the diode laser has been more effective compared to SRP alone, both for clinical and microbiological parameters. 13,14 However, despite these encouraging results, several studies have reported that the diode laser presented comparable results to SRP alone. 15,16 Moreover, a recent systematic review by Slot et al. 17 reported that a diode laser as an adjunct to SRP offers only moderate effects during the nonsurgical approach to periodontal disease; thus, its clinical relevance remains a matter of debate.
Considering these findings, the aim of this study was to further evaluate the effects of SRP+diode laser for the treatment of GAgP by analyzing clinical, microbiological, and immunological parameters. The null hypothesis was that, after a 1-year follow-up, there would be no variations between SRP+diode laser and SRP alone.
Materials and Methods
The local Ethics Committee of the University of Messina approved the study protocol (No. 12/16). Each patient was informed about the possible risks of the study and written informed consent was acquired by all patients in accordance with the Declaration of the World Medical Association 1975 in Helsinki, revised in 2000. Only subjects with a diagnosis of GAgP were enrolled in this prospective, split-mouth, double-blinded, randomized clinical trial (see Supplementary Table S1 at
The diagnosis of GAgP was performed following the criteria of the American Academy of Periodontology workshop. 18 The inclusion criteria were as follows: (1) good general health, (2) radiographic evidence of interproximal bone loss exceeding ≥50% of the root length, (3) a probing depth (PD) >5 mm at more than eight sites per quadrant, (4) ≥30 years old or <40 years old with a rapid bone loss as shown by radiographs, (5) a minimum of six teeth per quadrant, respectively, and (6) a concentration of more than 104 colony-forming units/mL of Actinobacillus actinomycetemcomitans. 19
The exclusion criteria were as follows: (1) periodontal therapy during the last 12 months, (2) use of antibiotics during the last 3 months, (3) pregnancy, (4) any systemic condition that might affect the study, (5) previous or current radiation or immunosuppressive therapy, (6) use of mouthwash containing antimicrobials during the previous 3 months, (7) use of hormonal contraceptives, (8) medication by anti-inflammatory and immunosuppressive drugs, (9) history of excessive drinking, (10) smoking, and (11) class II and III tooth mobility.
During the first phase of the study, 155 patients were initially enrolled from those referred to the School of Dentistry of the University of Messina (Messina, Italy). However, after screening, 124 patients were excluded because they did not meet the inclusion and exclusion criteria (n = 108), declined to participate (n = 14), or were lost during the first visit (n = 2). Thus, the final number of patients assessed for eligibility was 31 (Fig. 1).
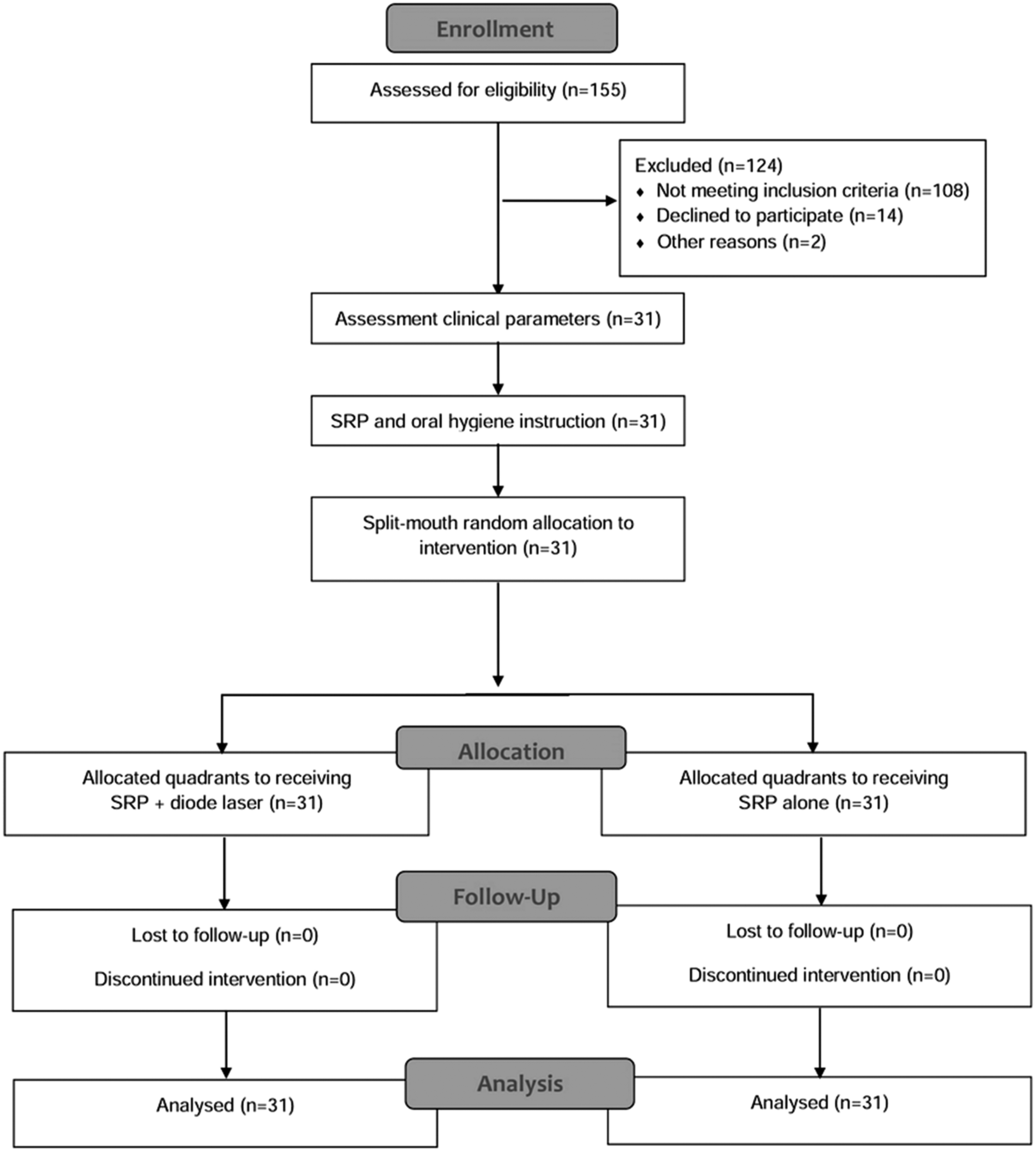
Flowchart of the randomized clinical split-mouth study design.
Clinical examination
Thirty-one patients, 14 men and 17 women, mean age 34.9 ± 1.2, were assessed for eligibility at the School of Dentistry at the University of Messina (Fig. 1). This trial was conducted from May 2012 to September 2016 in agreement with the CONSORT guidelines.
A full-mouth periodontal evaluation was performed in all subjects. The examiner collected probing measurements on six sites per tooth. Bleeding on probing (BOP) was recorded during the PD assessment by evaluating the possible presence of bleeding up to 30 sec after probing with a periodontal probe (UNC-15; Hu-Friedy, Chicago, IL).
Following completion of the clinical assessments, during the calibration sessions, intraexaminer repeatability and the reproducibility of clinical attachment level (CAL) were evaluated to obtain duplicate measurements of the clinical parameters from randomly selected patients.
Intraexaminer agreement was calculated by Cohen's k coefficient, which predicted a good degree of reliability (0.841) and a good reliability (ICC = 0.766) was found for all examinations. The kappa coefficients were calculated for the measurements obtained at each different examination.
The sample size was established considering an effect size of 0.40 with α = 0.050 and a power level of 0.80 for CAL, which was the primary outcome variable. A minimum sample of 24 quadrants per group would be needed. Thirty-one patients were enrolled, so that the primary variable, CAL, achieved a power value of 0.92.
Randomization and allocation to treatment
A clinician not involved in the trial generated a random quadrant allocation sequence by a ratio of 1:1 using a permuted block design by a computer random-number generator. In every subject, the upper maxillary quadrants were allocated to receive SRP+diode laser (A) or SRP alone (B) treatment.
The allocation concealment to the therapist was performed through serially numbered sealed envelopes and the details of the sequence were unidentified to the patients and clinicians participating in the study. Before every treatment, an investigator not involved in the recording and processing of data performed the assignment of the sealed envelopes marked with the initials of the name and date of birth of the patient and containing treatment methods for the treating clinician for each quadrant.
The examiners and patients were not informed about the type of treatment, thus avoiding bias in the evaluation of the experimental data. Shortly before each treatment session, another clinician opened the envelope with the assigned number by which the quadrant would subsequently be identified. The operator was informed and performed one of the two types of treatment. The same operator performed all the procedures and was blinded to previously recorded data and did not participate in any measurements or analysis.
Treatment
After admission to the study, each patient was instructed in oral hygiene and appropriate motivation, repeated at every appointment, and underwent supragingival prophylaxis by ultrasound and hand instrumentation.
At 7 days after treatment phase I, clinical data, which included PD, CAL, BOP, and full-mouth plaque score (FMPS), were recorded in all subjects (Table 1). Both quadrants included maxillary teeth 11–16 and 21–26. The evaluations were performed at baseline and at day 15, 30, 60, 180, and 365 (last follow-up).
p < 0.003. p value, ANOVA for repeated measure for variation of clinical parameters over time.
ANOVA, analysis of variance; BOP, bleeding on probing; CAL, clinical attachment level; DL, diode laser; FMPS, full-mouth plaque score; PD, probing depth; SRP, scaling and root planing.
All parameters were recorded by a calibrated examiner not involved in the treatment.
Each subject, after recording periodontal parameters, underwent one of the two following treatments: one maxillary quadrant was treated with SRP+diode laser, while the contralateral quadrant was treated with SRP alone. All the patients received treatment under local anesthesia. In the side assigned to diode laser+SRP, diode laser treatment was performed in a single session after instrumentation by ultrasonic instruments using an 810-nm laser (Wiser Laser Doctor Smile; Lambda, Vicenza, Italy) set at 1 W in pulsating mode at 50 Hz, toff = 100 msec, ton = 100 msec, and an energy density of 24.84 J/cm2, with a 300-μm fiber optic delivery system. The fiber tip was moved parallel to the root surface and the fiber was gently moved with a slow movement from apical to coronal into the periodontal pocket. The treatment was performed buccal-palatally and mesiodistally for 20 sec for each tooth of the quadrant included in the study. All sites were irrigated with saline solution after each session of irradiation to avoid any thermal damage. The laser treatment was performed in contact mode with the laser tip shifted with a constant speed of 2.5 mm/sec to reduce periodontal injury.
The contralateral quadrant was treated only with SRP. In this group, a placebo gel solution was used for 20 sec for each tooth to blind the patients to the application of product with respect to the test side. For the treatments, safety glasses were worn by the patient, surgeon, and dental assistant to prevent potential eye damage due to laser irradiation. Both quadrants in the mandible underwent the treatment but were not included in the results of this study.
At the end of both treatments, patients were advised to discontinue tooth brushing on the day of the treatment period. Subsequently, an oral hygiene protocol was prescribed.
Microbiological and inflammatory evaluation
In all subjects, subgingival plaque was acquired from eight interproximal sites at baseline and at 15, 30, 60, 180, and 365 days after therapy.
To permit specimen analysis, all sites chosen were isolated using cotton rolls. Subsequently, a sterilized paper point was introduced into the base of the selected site for 30 sec and a subgingival plaque sample was collected. The samples were stored in sterile Eppendorf vials with 0.15 mL of a solution of sterilized phosphate-buffered saline (PBS) and then stored at −80°C. In all samples, 40 microbial species were counted and investigated using the checkerboard DNA–DNA hybridization technique as described by Socransky et al. 20 Subsequently, whole genomic DNA probes to 40 subgingival species were digoxigenin labeled and hybridized in separate lanes of the miniblotter. Following hybridization, the membranes were rinsed and the DNA probes were identified by an antibody conjugated with digoxigenin and with alkaline phosphatase and chemiluminescence exposure, transformed to absolute counts comparing the regression line that resulted from the values on the same membrane as previously described by Novaes et al. 21 If the signal was not perceived, it was documented as 0. For each run, two lanes comprised standards at concentrations of 105 and 106 cells of all the microbial species analyzed. The test sensitivity was corrected to allow for the recognition of 104 cells for each microbial type by correcting the concentration of all DNA probes.
Gingival crevicular fluid (GCF) was obtained from eight other different noncontiguous interproximal sites using filter paper strips (PerioPaper; Oraflow) as previously described. 22 The levels of interleukin (IL)-1β, IL-10, and tumor necrosis factor (TNF)-α were measured by enzyme-linked immunosorbent assay using an equation with software.
Statistical analyses
For the analysis of clinical parameters, all test units were obtained from the average of six measurements per treated tooth and at a minimum of six teeth per treated quadrant. The clinical parameters were evaluated by Student's t-test for paired data. The patient's maxillary quadrant was set as a test unit for statistical analysis and evaluation.
Microbial data are presented as the mean counts ( × 105) of each microbial species and the significant differences in each group for mean counts of all microbial species were detected by the Wilcoxon test. Values are expressed as the mean ± standard error of the mean (SEM) and analyses were performed after corrections for multiple assessments as previously described. 23
Total protein values were converted to picograms per milliliter. The final cytokine levels analyzed were obtained by the values initially resulting from the multiplexing system from the total amount of protein in GCF (picograms per milliliter) and the IL-1β/IL-10 ratio was estimated per quadrant group by the Friedman test. 24 Differences between quadrants during all experimental periods and among quadrants for the mean concentrations of IL-1β, IL-10, and TNF-α were calculated by two-way analysis of variance (ANOVA) and a post hoc Bonferroni test. All statistical analyses were executed using SPSS 17.0 for Windows, and p < 0.05 was considered to be statistically significant.
Results
All enrolled patients successfully completed the study. Mean values (±standard deviation, SD) of the periodontal parameters, such as PD, CAL, BOP, and FMPS, are reported in Table 1.
At baseline, no significant differences were present between groups for all parameters.
Comparison over time shows that in the SRP+diode laser group, significant differences existed at 60 days for PD and CAL values (p < 0.003) (Table 1). At 15, 30, and 180 days, there was no significant difference between the two treatments for PD, CAL, BOP, and plaque score values. At 1 year, both treatments produced a reduction of every periodontal parameter compared to the values recorded at baseline, and this difference was statistically significant in the SRP+diode laser group (p < 0.05) (Table 2). However, at 1 year, a comparison between the two treatments showed that SRP+diode laser therapy significantly reduced (p < 0.001) PD (2.56 ± 0.44 mm compared to 3.36 ± 0.51 mm in the SRP-alone treatment) and CAL (3.47 ± 0.25 mm compared to 4.11 ± 0.26 mm in the SRP-alone treatment), while BOP was reduced but without statistical significance (26.16% ± 2.4% compared to 32.26% ± 3.1% in the SRP-alone treatment) (Table 1).
p < 0.001; ** p < 0.05.
IL, interleukin; TNF, tumor necrosis factor.
The changes in the proportions of periodontopathogens at baseline and at day 15, 30, 60, 180, and 365 in the SRP+diode laser and SRP-alone group are shown in Fig. 2. Of the 40 microbial species evaluated at each time point, the SRP+diode laser group showed significant reductions in four species of the orange complex at 30 and 60 days compared to the SRP-alone group (Fig. 2). Further, there was no significant decrease in the number of the red complex species (Porphyromonas gingivalis, Tannerella forsythia, and Treponema denticola) between the two groups during the different follow-up sessions (p > 0.05).
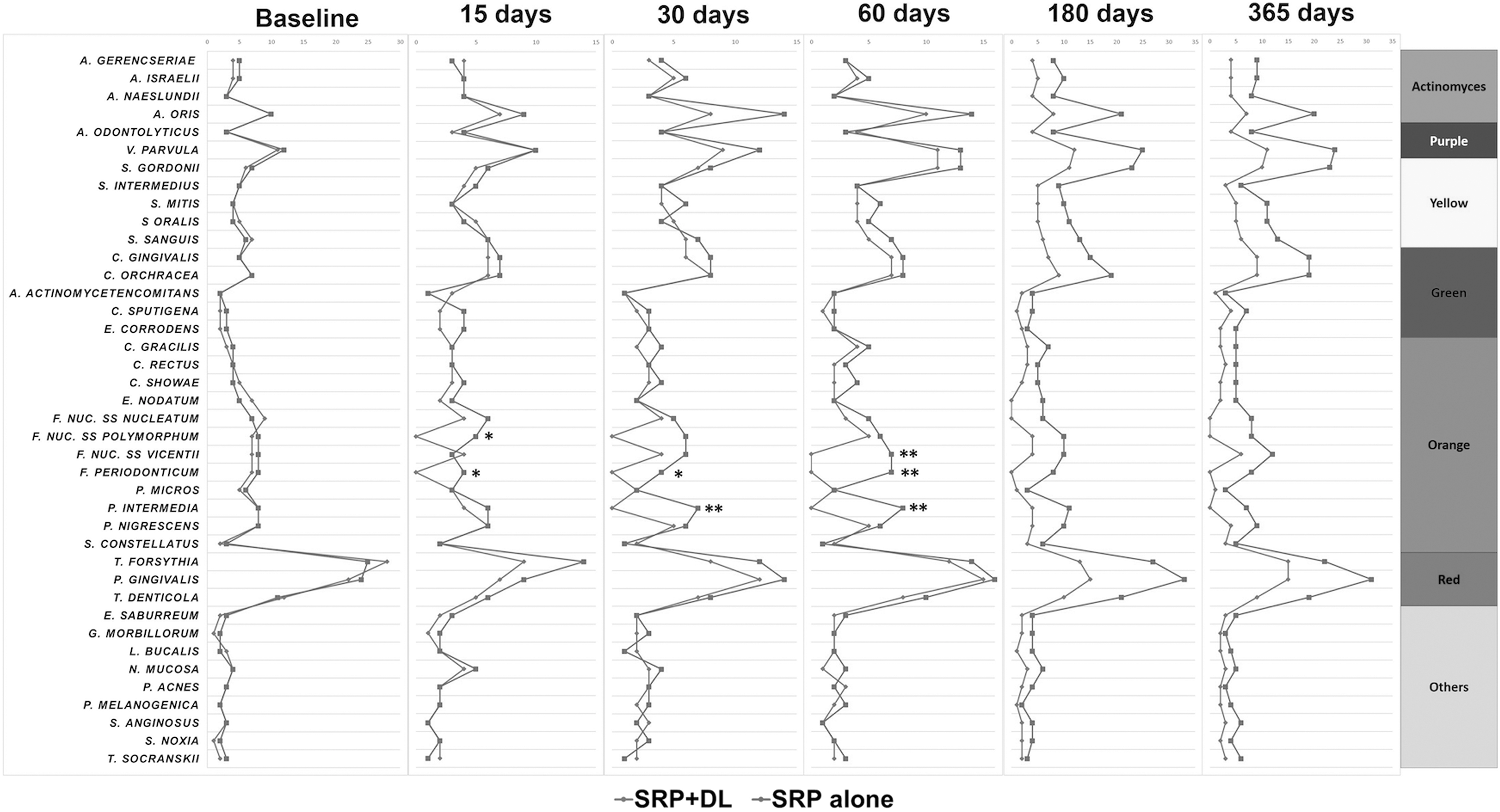
Mean counts ( × 105) of 40 bacterial species in the SRP+DL and SRP-alone groups at baseline and 15, 30, 60, 180, and 365 days and the results of intergroup comparisons. The species were ordered according to the microbial complexes described by Socransky et al. 20 *p < 0.05; **p < 0.001. DL, diode laser; SRP, scaling and root planing.
The entire distribution of the mean values of GCF cytokines is represented in Fig. 3. There was a statistically significant reduction of the mean GCF values due to the treatment response in both groups from baseline to the last follow-up. However, the SRP+diode laser determined a significant reduction in the mean level of IL-1β at 15 and 30 days compared to the SRP-alone group (p < 0.05). There was a significant difference in the mean levels of IL-10 that was higher in the SRP+diode laser group at 30 and 60 days compared to the SRP-alone group (p < 0.05) (Fig. 3). There were no statistically significant differences in the mean TNF-α level between the two groups during the different follow-up sessions, while the IL-1β/IL-10 ratio was significantly lower at 15 and 30 days in the SRP+diode laser group compared to SRP alone (p < 0.05).
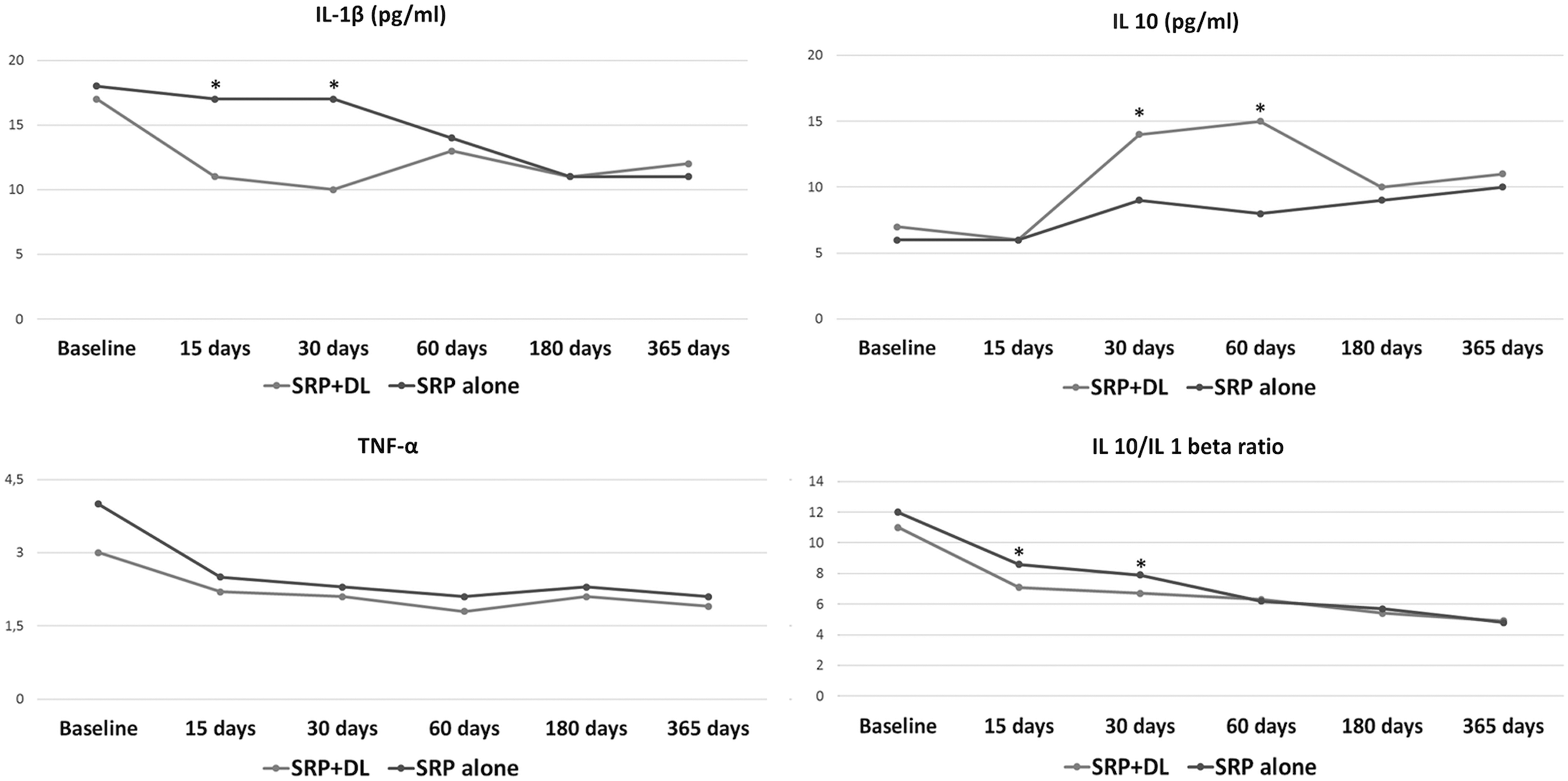
Mean levels (picograms per milliliter) of IL-1β, IL-10, and TNF-α and IL-1β/IL-10 ratios at baseline and at 15, 30, 60, 180, and 365 days in the SRP+DL group and SRP-alone group. *p < 0.05 between groups in the same period of analysis, Wilcoxon test. IL, interleukin; TNF, tumor necrosis factor.
Discussion
This randomized, double-blind, split-mouth, clinical trial compared the effect of SRP alone versus SRP plus diode laser using clinical, microbiological, and inflammatory analyses in patients with GAgP.
Both treatments improved the clinical, microbiological, and inflammatory outcomes. However, after a single treatment, SRP plus diode laser yielded a statistically significant improvement in PD and CAL at 12 months compared to the SRP alone. However, it did not significantly reduce the percent of bleeding sites compared to SRP treatment alone.
One of the key points of nonsurgical periodontal therapy in GAgP patients is to reduce or eliminate the subgingival bacterial burden, 13,25 which increases the risk of periodontal disease recurrence 26 and long-term tooth loss. 27
For this reason, for several decades, SRP has frequently been enhanced by the use of many adjuncts. Systemic or local delivery of antimicrobial agents was used in addition to SRP with good results. 28 However, several studies have indicated slightly favorable clinical long-term results and bacterial resistance due to the use of the antibiotics. 29 Thus, greater efforts are being made to identify new treatment strategies that do not rely on antibiotics.
Our research focused on diode laser therapy as an adjunct to SRP for the nonsurgical treatment of GAgP.
Several studies have shown that the diode laser, as an adjunct to SRP, significantly reduced the bleeding sites in patients with periodontal disease affected by type 2 diabetes 30 and Fanconi anemia. 31 Many controlled clinical trials that have evaluated the treatment of moderate and deep pockets have demonstrated that the diode laser, as an adjunct to SRP, improved periodontal treatment during GAgP. 13,32,33 De Micheli et al. 34 also showed that diode laser therapy was able to enhance the PD and CAL values after 6 weeks of nonsurgical treatment of active periodontal disease, probably due to the effect exerted by the diode laser on the reduction of PD through the de-epithelialization of the periodontal pocket. 35,36 Novaes et al. 21 showed that when the diode laser was used into the periodontal pocket as an adjunct to SRP, there was a decrease in inflammation and reduction of the bacterial load at 90-day follow-up in patients with GAgP.
Based on the pilot observation by Novaes et al., 21 we designed the current study to compare the clinical, microbiological, and inflammatory effects of SRP+diode laser or SRP alone in a 1-year study. Our study demonstrated that, at 1-year follow-up, when the diode laser was combined with SRP, there was a significant decrease in the main periodontal clinical parameters (PD and CAL), while microbiological and inflammatory measures were significantly reduced only at the first follow-up sessions compared to SRP alone.
A strong reduction in the periodontal pathogens, especially the orange and red complex bacteria, is one of the key factors in the clinical success of nonsurgical periodontal therapy. In fact, previous reports highlighted that gram-negative bacteria in periodontal pockets are difficult to eliminate. 37,38
Our results are consistent with recently published reports showing that the diode laser possesses clinical, microbiological, and immunological benefits during the first phase after the treatment of periodontal pockets in patients with GAgP. 13
Our study also indicated that at 15 and 30 days, SRP+diode laser can significantly reduce GCF levels of the IL-1β/IL-10 ratio compared to SRP alone (p > 0.001). A previous report showed that a discrepancy in this ratio in GCF is related to the development and course of periodontal disease. 39 Further investigators have suggested that a higher IL-1β/IL-10 ratio may be correlated with elevated proportions of periodontal pathogens of the orange and red complex. 40 The reduced composition of periodontal pathogens found in the SRP+diode laser group may influence the GCF level reductions of proinflammatory cytokines.
Conclusions
The effects of several diode laser protocols and photodynamic therapies as adjuncts to SRP on GAgP have been studied. This study indicated that after 1 year of treatment, both treatments produced an improvement in the clinical, microbial, and inflammatory parameters in patients with GAgP. However, a single session of diode laser as an adjunct to SRP was more effective and promoted significant clinical effects at 1 year in pocket depth and CAL values, while microbial and inflammatory parameters were comparable to SRP alone.
Footnotes
Acknowledgment
The authors thank Dr. Rita Aveni of the University of Messina for her help in searching for literature.
Author Disclosure Statement
This work has been performed with departmental funding only. The authors declare that they have no conflict of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.