
Abstract
Introduction
B
Breast-conserving surgery followed by radiotherapy has been a standard treatment for small-sized breast cancer. 2 However, to avoid invasive treatment, several less invasive treatment options, including laser ablation, radiofrequency ablation (RFA), or cryotherapy, have been developed for early breast cancer. 3 –8 Although these techniques are promising for early breast cancer, a major disadvantage is that it is impossible to obtain the negative margins of breast cancer because of nonvisualized surgical field. Also, without accurate obtaining of negative margin, the patient with breast cancer would experience local recurrence, which needs additional surgery or chemotherapy. 9,10
The most important factor to control of local recurrence is obtaining negative margins of breast cancer in surgery. The use of frozen sections intraoperatively is a favorable method to evaluate the surgical margin. 11 Even if the absence of tumor in the margin has been confirmed intraoperatively, tumor cells are occasionally identified at surgical margins in the final pathological report. When tumor cells are detected in the surgical margin, physicians usually choose additional excision or adjuvant radiotherapy. 12 To reduce the difficulties associated with this and minimize the local recurrence of breast cancer, many cancer centers are performing intraoperative radiotherapy. 13,14
Laser ablation or photodynamic therapy (PDT) has been applied solely for treatment of human disease. 15,16 However, the combination technique with laser ablation and PDT is rarely reported, especially for breast cancer. 17 –19 In this study, the authors compared laser ablation and PDT to assess their therapeutic efficacy for breast cancer. And we also evaluated the pathologic margin status after combination treatment with laser ablation and PDT.
Materials and Methods
Ethical approval
Animal care and experiments were carried out in accordance with the Institutional Animal Care and Use Committees of Korea Institute of Science and Technology (KIST) (No. 2014-038).
Breast cancer cell line
The breast cancer cell line, MDA-MB-231 (basal-type, triple negative breast cancer), was purchased from the American Type Culture Collection (ATCC). MDA-MB-231 was maintained in Dulbecco's modified Eagle's medium (Gibco, Grand Island, NY) containing 10% fetal bovine serum (Gibco), 100 U/mL penicillin, and 100 μg/mL streptomycin (Gibco) in a 5% CO2 humidified incubator.
Tumor xenograft model
Animals were maintained on a 12-h light–12-h darkness cycle at 22°C to 25°C under specific pathogen-free conditions and fed with standard xenograft mice chow and water ad libitum.
BALB/c nude mice (5-week-old female, CAnN.Cg-Foxn1nu/CrljOri, n = 12) weighing 20–22 g each were purchased from Orient Bio, Inc. (Seongnam, Republic of Korea). Breast cancers were induced by the subcutaneous inoculation of MDA-MB-231 cells (1 × 107 cells suspended in 60 μL of culture medium) into the subcutaneous layer of the left thigh and grown for 5 weeks. During the transplantation of tumor cells, the mice were anesthetized with intraperitoneal injection of the solution (300 μL) of tiletamine hydrochloride (1 mg/mL), zolazepam hydrochloride (1 mg/mL), and xylazine hydrochloride (0.2 mg/mL) in saline. No anti-inflammatory or analgesic agent was administrated.
After the breast cancer tumors had grown larger than 5–10 mm in diameter and 50–100 mm2 in volume, they were isolated from the mice and the proliferation of breast cancer was confirmed by a pathological examination. The tumor burden was measured using its diameter and volume. The diameter was measured with a digital caliper and the volume was calculated based on the following formula on each of nine days: width × length × height × 0.5.
After confirmation of the successful development of the xenograft mice tumor models, the mice were treated with four different procedures: control (without any treatment, group I, n = 3), treated only with laser ablation (group II, n = 3), treated only with PDT (group III, n = 3), and treated with the combination of laser ablation followed by PDT (group IV, n = 3).
Pilot study
To evaluate the laser effect to breast cancer, laser ablation was performed on six other xenograft mice. Also, to confirm the maximum effect of PDT, we performed a preliminary study with different numbers of PDT sessions on breast tumors of seven mice models.
Laser ablation
The laser ablation was performed under in vivo conditions with a diode laser ablator (DINONA, Inc., Seoul, Republic of Korea). The mice were anesthetized with intraperitoneal injection of the solution (300 μL) of tiletamine hydrochloride (1 mg/mL), zolazepam hydrochloride (1 mg/mL) and xylazine hydrochloride (0.2 mg/mL) in saline. The distal tip of the multidirectional bundle-type laser fiber was localized at the center of the tumor and then, the MDA-MB-231 tumor xenograft mice underwent laser ablation (diameter, 600 μm; wavelength, 980 nm; output power, 5 W; exposure time, 5 min).
Photodynamic therapy
For preparation of nanoparticle type of methylene blue, the methylene blue trihydrate (20 mg, 0.05 mmol; Sigma-Aldrich Co., Munich, Germany) and sodium oleate (30 mg, 0.10 mmol; Sigma-Aldrich Co., Munich, Germany) were added into tetrahydrofuran (THF). Furthermore, for the ternary complexation, methylene blue–oleic acid binary complex and Pluronic F-68 (20 mg; Sigma-Aldrich Co., Munich, Germany) were mixed with THF (1.2 mL).
For the procedure of PDT, a total of 60 μL per mouse of 10.05 mg/mL biocompatible nanocomplex formulation of methylene blue (nanoMB) dispersion was injected into three different points of the peritumoral site, the protocol for which is described in our previous report. 20 One hour after the injection, 655-nm laser excitation was performed for 10 min by irradiating the collimated laser beam through the induced breast tumor. Singlet oxygen generation was evaluated in vitro by monitoring a decrease in the absorbance of the p-nitrosodimethylaniline (RNO) at 440 nm under an excitation of 655 nm laser (0.2 J/cm2·s; Changchun New Industries Optoelectronics Tech. Co., Ltd., China). The mixture solution was prepared in deionized water by mixing 0.21 mL of NanoMB (10.05 mg/mL) or free MB solution of an equivalent absorption at 655 nm with 0.11 mL of RNO stock solution (0.12 mM), 0.7 mL of histidine (0.03 M), and 0.18 mL water. Laser excitation at 655 nm was performed by irradiating the collimated laser beam through the sample. The relative quantum yields of 1 O2 generation were estimated by using an aqueous solution of free MB as a reference and comparing the derived slopes of RNO absorbance plots (−ln A440) as a function of laser irradiation time. This procedure was repeated every 2 days, a total of five times, for all mice.
Combination of laser ablation and PDT
The combination technique involved the use of both laser ablation and PDT as described above. First, laser ablation was performed on the xenograft mice with a multidirectional bundle-type laser fiber under in vivo conditions. The next day, the nanoMB was locally injected into three points at the peritumoral site. One hour later, irradiation with a 655-mn laser for PDT was performed for 10 min. This irradiation process was repeated five times every 2 days (Fig. 1). The changes of tumor volume were calculated and compared with those in the mice models that received treatment with only laser ablation or PDT for 15 days.
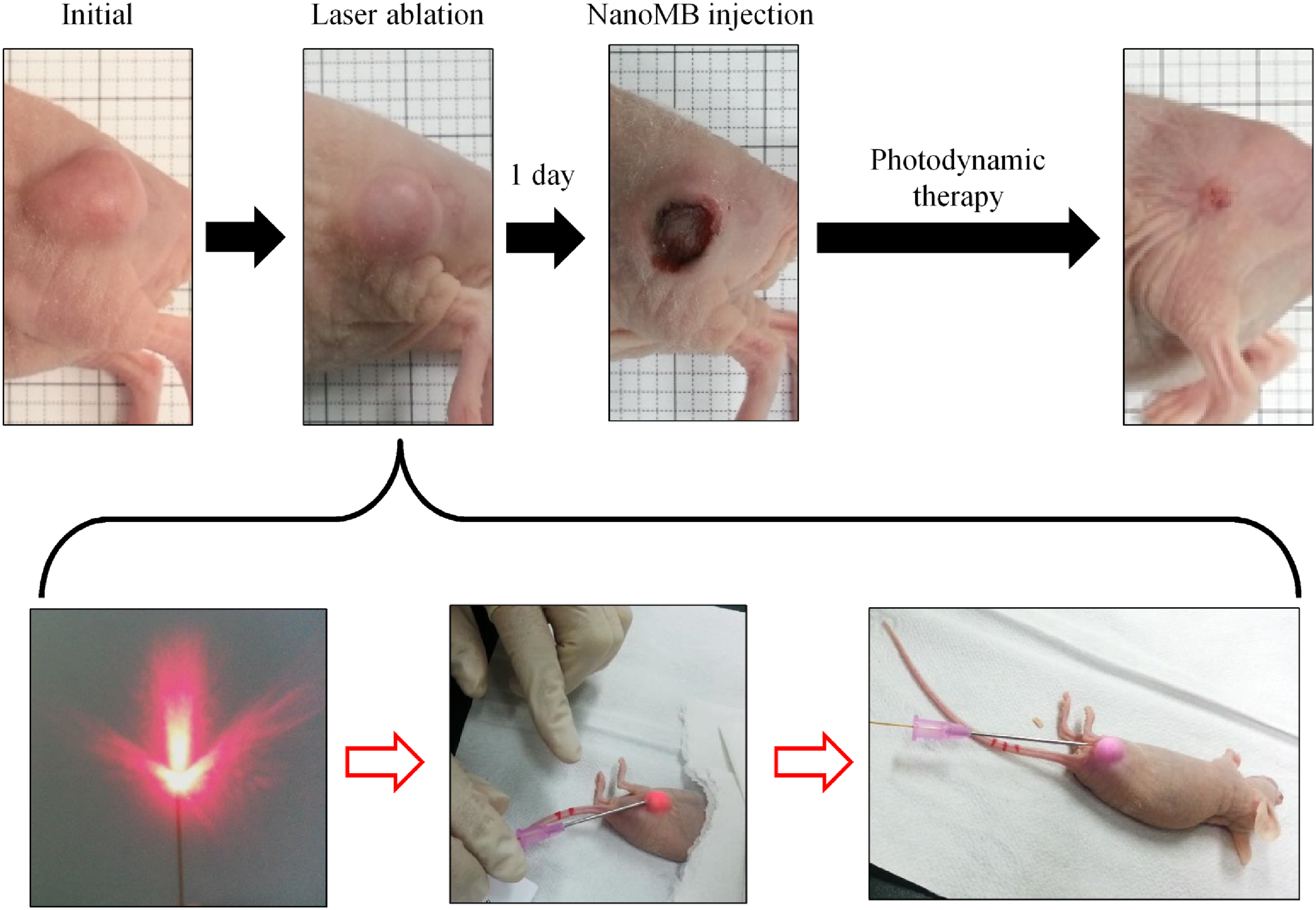
Combination of laser ablation and PDT to treat MDA-MB-231 tumor xenograft mice. Laser ablation was conducted on xenografted mice under in vivo conditions and the nanoMB solution was injected into the peritumoral site 1 day later. Irradiation with a 655-mn laser for PDT was then applied 1 h later for 10 min. PDT, photodynamic therapy.
Pathological examination
For histological analyses of the treated tumors, the specimens were sent for pathological analysis unfixed immediately after the treatment procedures. The specimens were transected as serial sections with 2-mm intervals and photographed to record gross anatomical tissue changes. Hematoxylin and eosin (H&E) staining was carried out after embedding the tissue in paraffin. Microscopic findings were also captured with a series of objective lenses (20 × , 40 × ). After laser ablation, the zones of breast tissue could be distinguished as three areas as follows: a carbonized zone (zone 1), a coagulation zone (zone 2), and a normal breast tissue zone (zone 3).
Statistical analysis
Based on the power calculation (using GPOWER software), approximately 10 mice per group were required for accurate comparison. However, we conducted the pilot studies to assess the treatment effects of laser ablation and PDT with six and seven mice. Therefore, we calculated the sample size as three mice per group to compare each treatment effect or combination effect.
Data were expressed as the mean ± standard error (SE). Repeated measures ANOVA test was used to assess the comparisons of extent of tumor diameter and volume. p-value ≤0.05 was considered statistically significant. And the analysis was performed with SAS.
Results
Pilot study
In preliminary study with laser ablation, thermal transformation due to laser ablation resulted in three clearly distinct zones in xenograft mice breast tumors. H&E staining clearly demarcated the three zones. Zone 1, which was directly affected by laser ablation, featured the complete destruction of breast tissue, while zone 2 showed only a coagulation effect (Fig. 2).
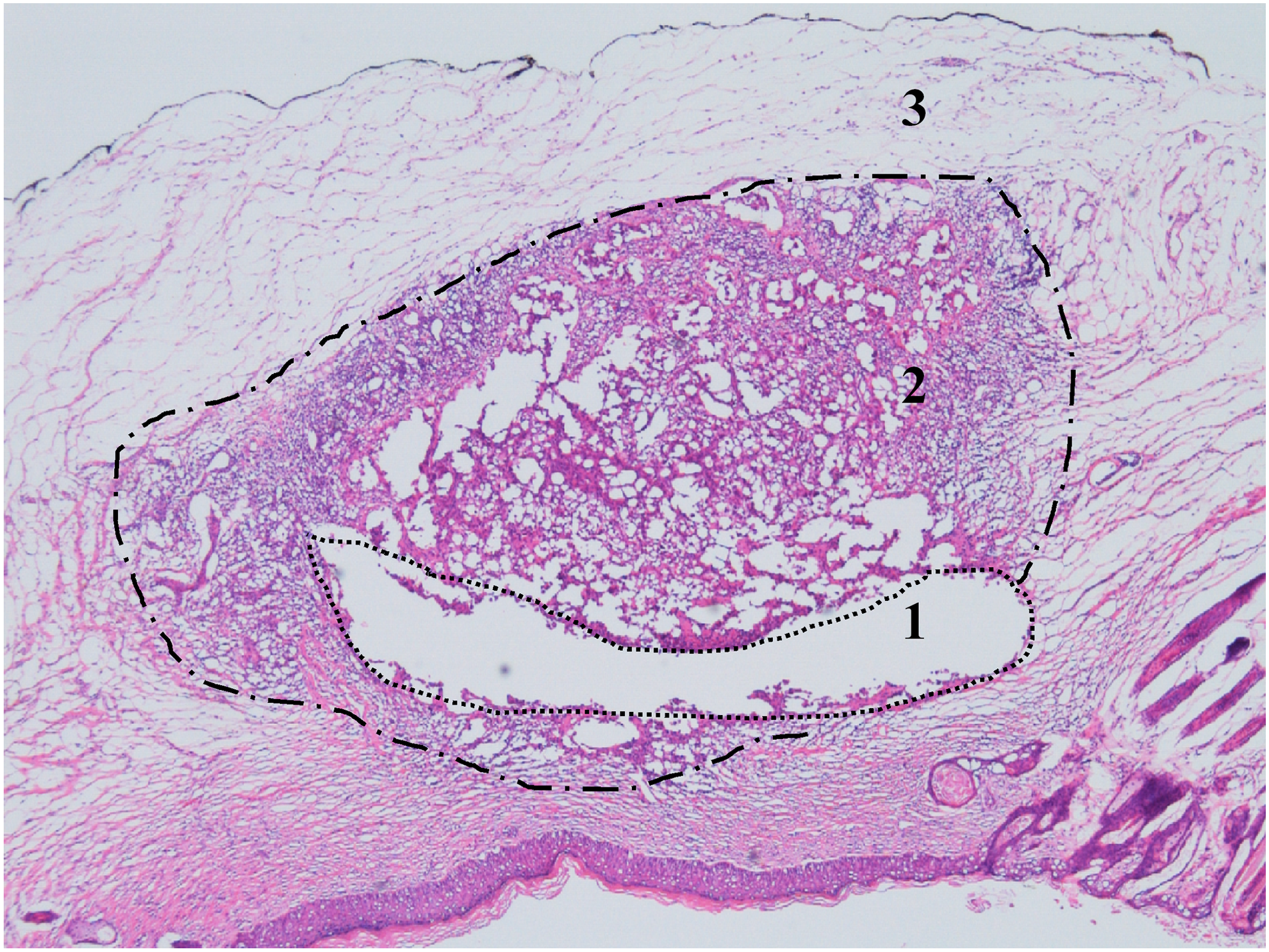
Microscopic findings (40 × ) with H&E staining of MDA-MB-231 tumor in xenograft mice ablated with a laser using multidirectional firing fibers. The zones were clearly demarcated as follows: carbonization with necrosis (zone 1), coagulation with thermal transformation and tissue damage (zone 2), and undamaged (zone 3), based on H&E staining. H&E, hematoxylin and eosin.
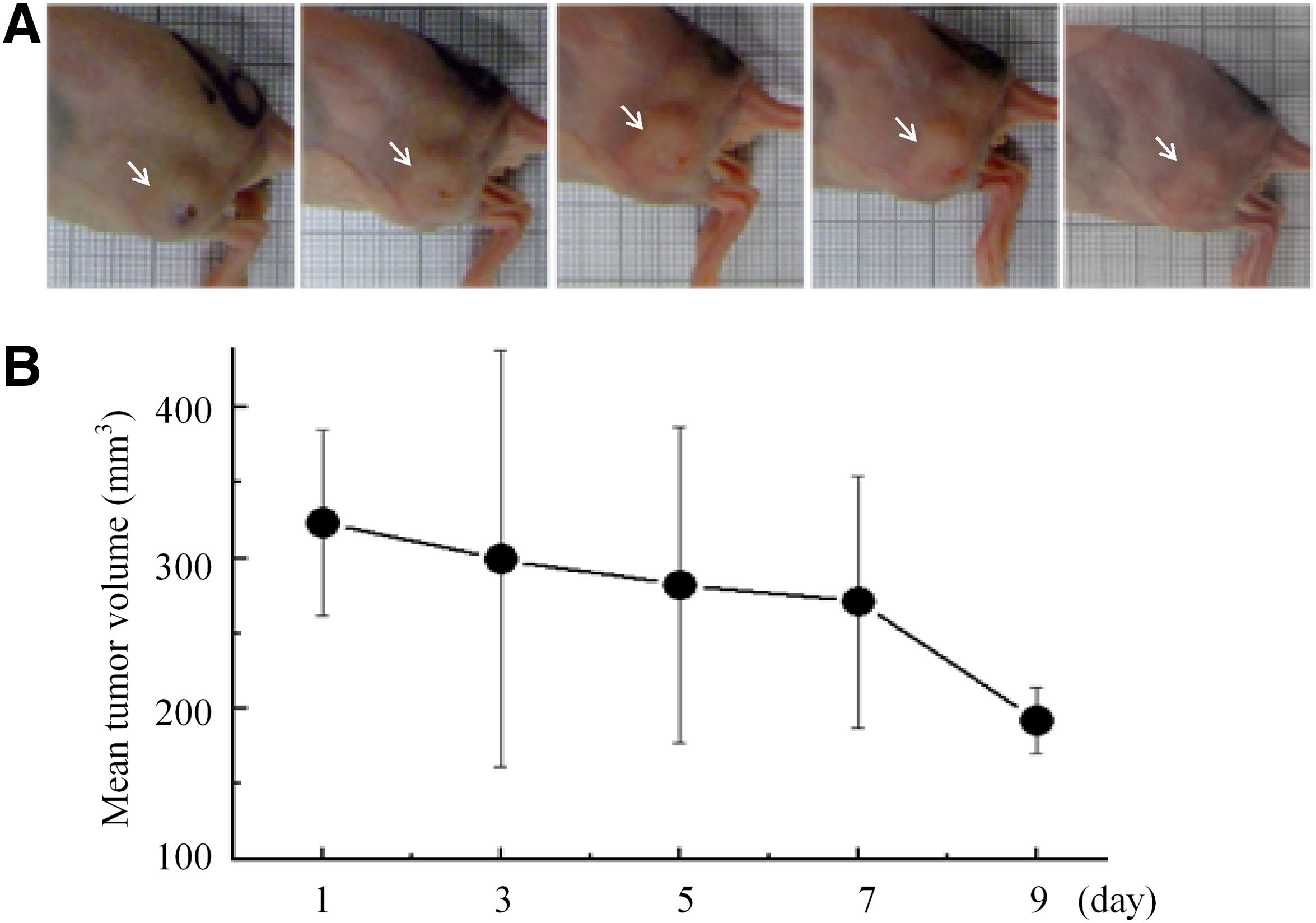
In preliminary study with PDT, the ulceration of the superficial layer of the breast tumor occurred when one to two sessions of PDT were conducted on breast tumors. However, as the number of PDT sessions increased, the ulceration on the breast tumor, instead, transitioned to healing (Fig. 3A). When more than four sessions of PDT were performed serially every two days, the residual tumor size decreased to less than 2 mm in diameter. The breast tumor completely disappeared in one case in which PDT was performed five times (Fig. 3B, C). After four consecutive sessions of PDT, the tumor burden of xenograft mice was rapidly decreased. However, that did not change much after the fifth. Upon treatment of breast tumors with a maximum of five sessions of PDT, the tumor burden was estimated using the tumor volume. Although the tumor burden slightly decreased during the first three sessions of PDT, it significantly decreased 7 days after the initial treatment. The tumor was largely decreased in size as well as healed without ulceration (Fig. 4). The effect of PDT on xenograft mice breast tumor was confirmed by histological examination. The histological findings showed that the breast tumor burden decreased depending on the number of PDT sessions, and the tumor was completely replaced with fibrosis and inflammation after five sessions of PDT (Fig. 5).
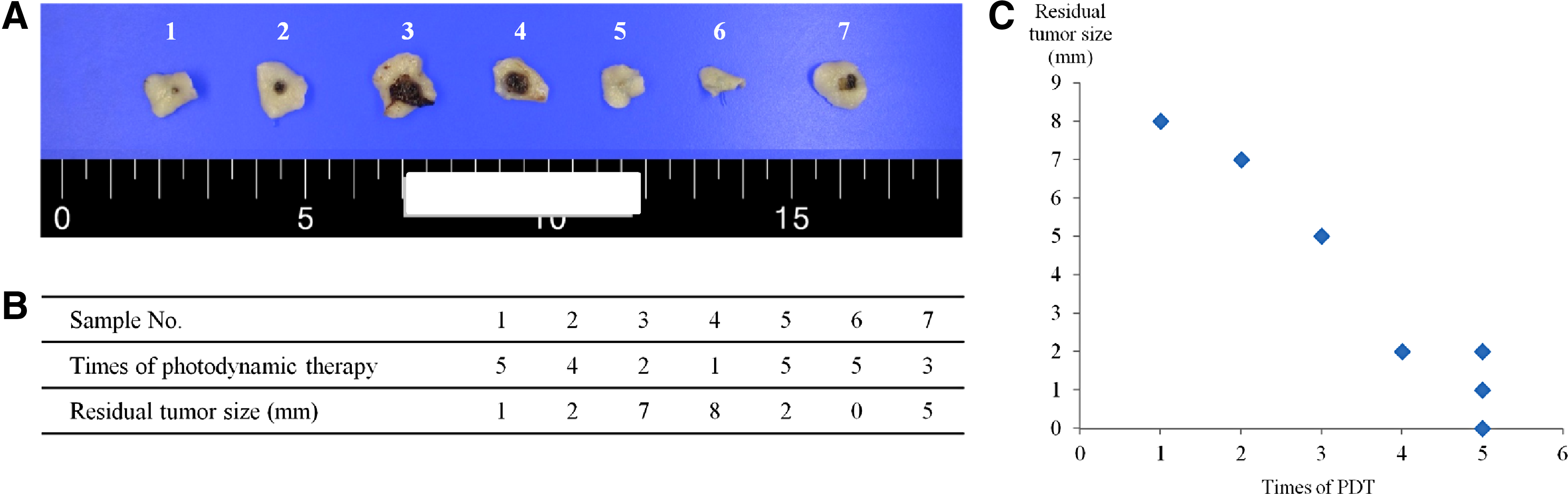
Seven cases of mice model with breast tumor treated with PDT.
The change of tumor shape and burden during five sessions of PDT.
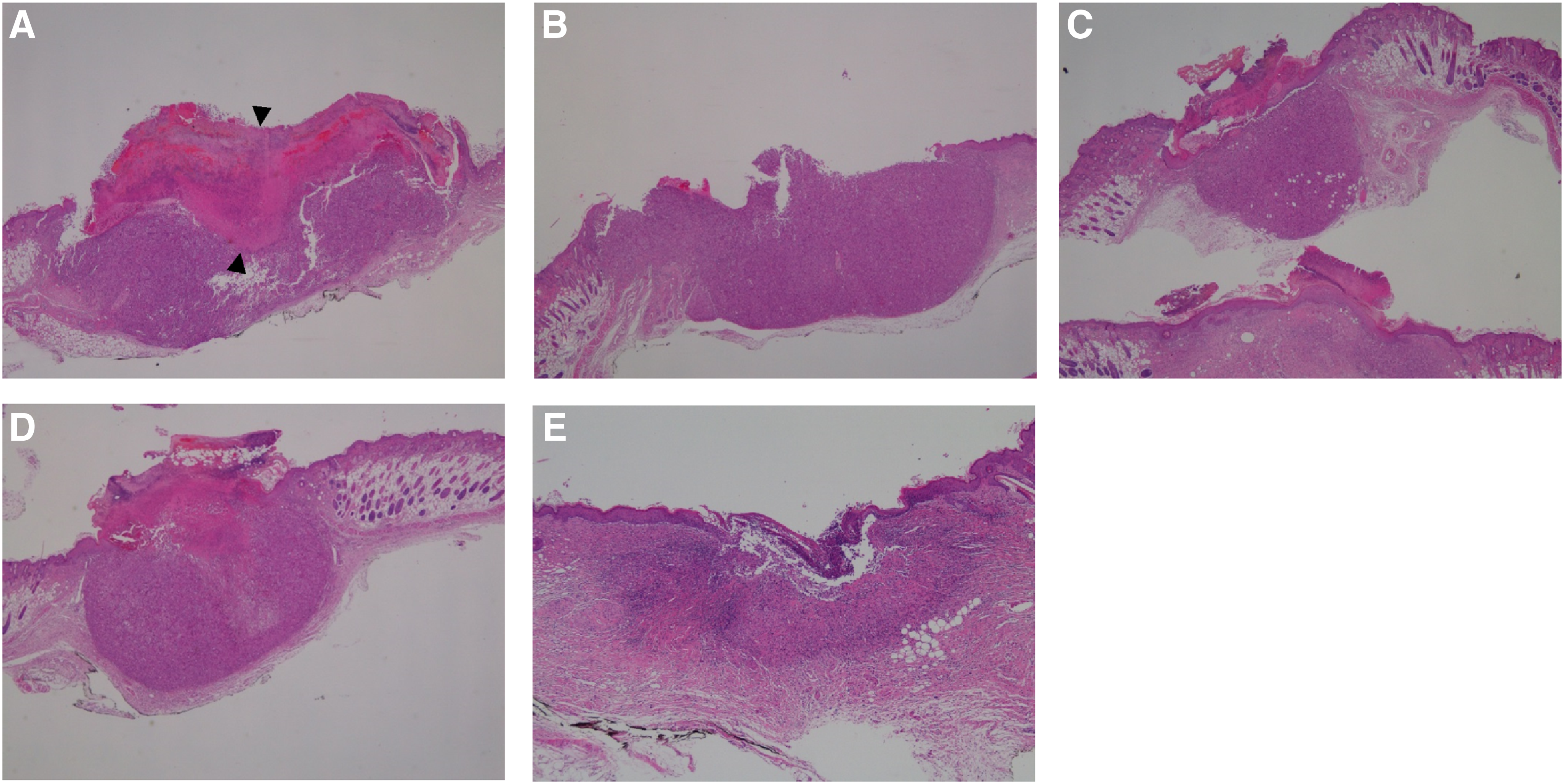
Microscopic findings after different numbers of PDT sessions (H&E, 20 × ). The tumor exhibited an ulcerative cluster on its surface, central tumor necrosis, and a peripheral area of viable tumor layers.
Comparisons of tumor volume and histologic results
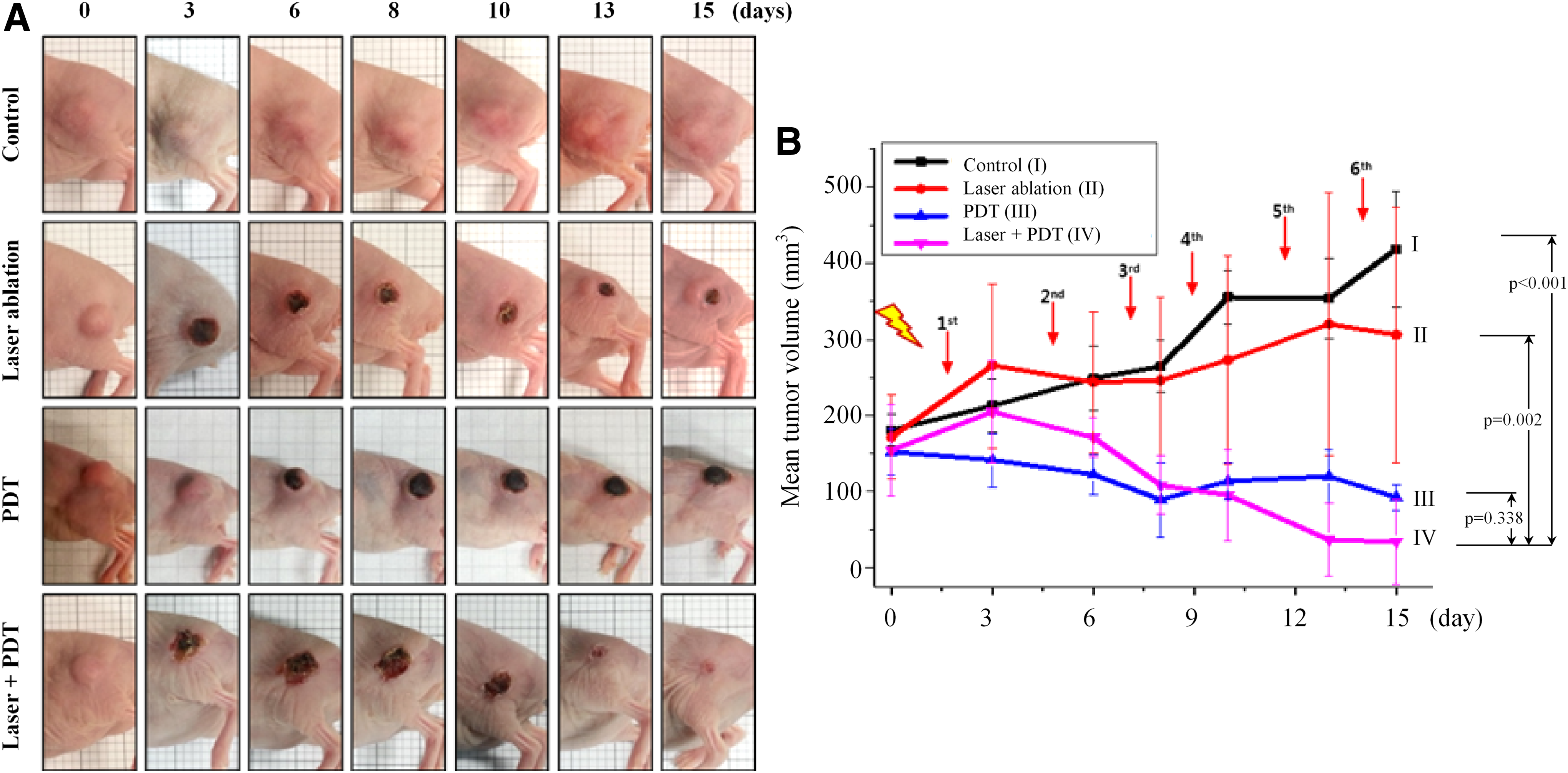
During 15 consecutive days, the effects of the treatments on the xenograft mice breast tumor models were compared among the four different groups. In group II, although superficial ulceration occurred diffusely, the tumor volume increased gradually rather than decreased. However, in groups III and IV, the tumor volume significantly decreased after the first treatment. In group IV, the superficial ulceration healed after the fifth treatment of PDT and the trend of tumor volume was reversed to a decreasing pattern after 9 days, in contrast to that in group III (Fig. 6A, B).
All breast tumors in the mice models were removed in each group and subjected to pathological examinations. In group A, the breast cancer cells were tightly packed in the entire tumor. In group II, the laser effects involved the production of central zones of necrosis and coagulation, while the breast tumor cells were still viable in the peripheral zone. However, in group III, superficial ulceration occurred and the eschar was removed. The number of breast tumor cells was significantly decreased in the group IV (Fig. 7).
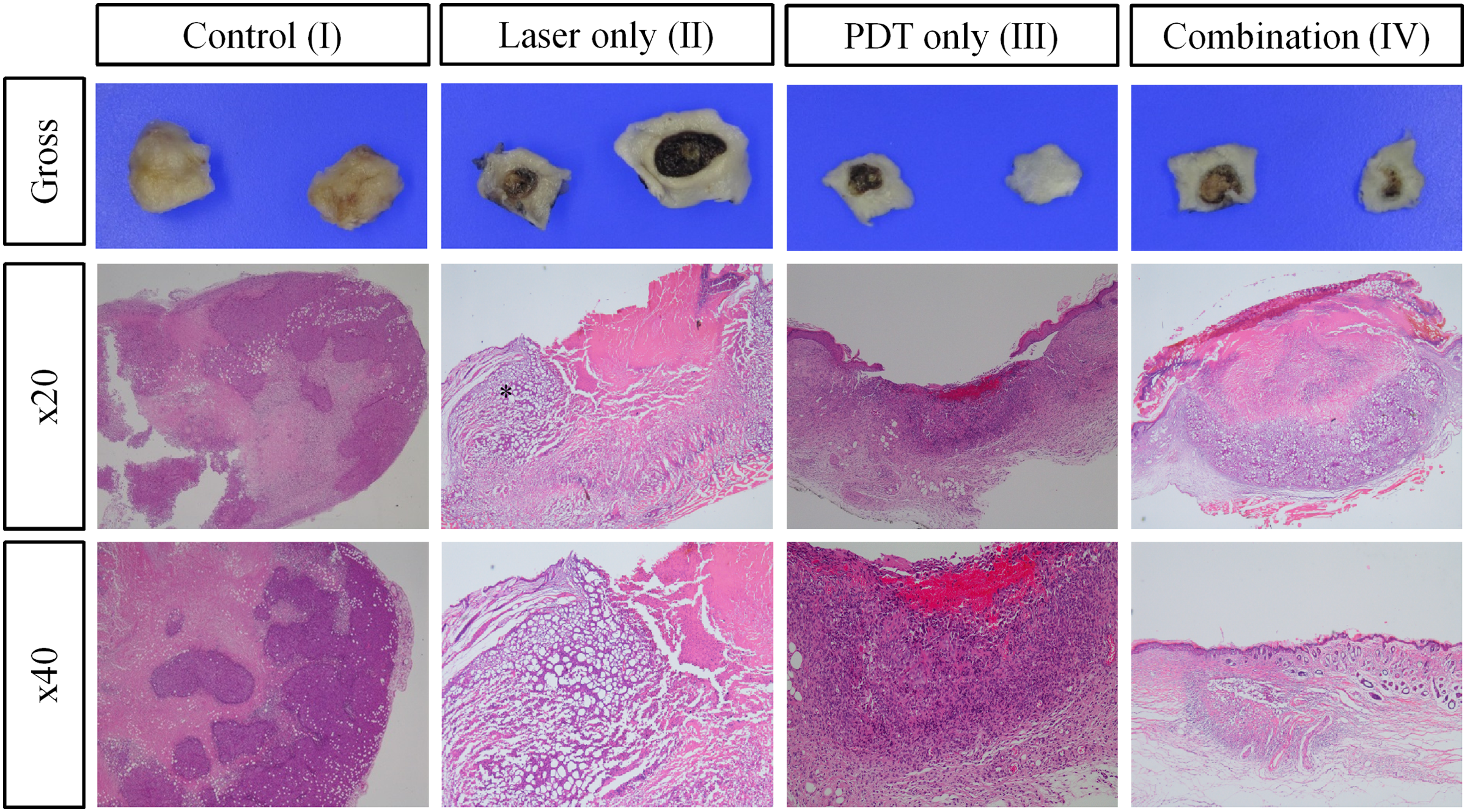
All MDA-MB-231 tumor in xenograft mice was removed in each group and subjected to pathological examinations. In group II (laser only), the tumor cells revealed central thermal necrosis and coagulative necrosis resulting from the laser ablation therapy. In group III (PDT only), the tumor exhibited a surface ulcerative cluster and erosion induced by phototherapy. The underlying tumor cells revealed a reduction in volume and some necrosis, but no cauterizing effect occurred. In group IV (combination laser and PDT), the laser effects were shown in the central thermal necrotic zone, along with superficial ulceration and eschar.
Statistical results
A significant interaction between groups was observed by time (p < 0.001). And group IV showed the most effective result during 15 days and statistical significance compared to group I and II (p < 0.001, p = 0.002). However, there was no significant difference between group III and IV, even if the mean tumor volume of group IV showed the greatest decreasing pattern (p = 0.338).
Discussion
Recently, breast cancer has been diagnosed when it is still at a small size and an early stage by using screening techniques. 21,22 In line with this trend, the surgical scale for breast cancer has been reduced and even nonsurgical treatments, including RFA, cryotherapy, and laser ablation, have been developed. 3 –8 Although these minimally invasive treatments have showed some effectiveness at killing cancer cells, their clinical application is still insufficient because of an inability to manage and evaluate the margin status.
For almost every malignancy that requires surgery for treatment, R0 resection (no cancerous cells seen microscopically) with a negative surgical margin is very important to reduce local recurrence. In particular, because the breast is characterized by the lack of a clear margin distinguishing it from the surrounding organs, obtaining a negative surgical margin would be more important for local control. Furthermore, breast cancer is a very heterogeneous disease, having multiple histological subtypes or a mixed nature involving an invasive focus and an in situ lesion within a single mass. Therefore, even if a sufficient surgical margin has been obtained grossly, a microscopic malignant lesion can still remain in the surgical margin.
We studied laser ablation and PDT with nanoMB injection as a nonsurgical treatment for breast cancer. Specifically, we compared the efficacy of each of these treatments and their use in combination for treating breast cancer in a mice model.
Laser ablation has been widely applied to treat malignancies of various organs. 5,23,24 However, unidirectional laser fiber has a common disadvantage of causing thermal damage to the surrounding structures. To overcome this problem, we studied laser ablation using a multidirectional fiber. 25 –27 This enabled the formation of a round area of necrosis, which ensured the negativity of the margin, and we supposed that the therapeutic effect was sufficient to make a negative margin. However, in a recent study, a single procedure with laser ablation was insufficient for the treatment of breast cancer. Total tumor volume was not significantly decreased during the first 7 days after the initial procedure, despite obvious cell damage being revealed by a microscopic examination. The tumor volume actually increased after eight days. This would have occurred because of the revival of tumor cells in the coagulation zone, which is located in the margin of a breast tumor. This means that, even if cancer necrosis is induced in the center of the tumor by laser ablation, a negative margin could not be obtained by a single procedure with laser ablation.
PDT has been known for several decades to be a light-activated cancer treatment modality for various malignancies. 28,29 The therapeutic effect of PDT is believed to involve the initiation of tumor-specific cell necrosis with a photochemical reaction to generate reactive oxygen species. 30 As photosensitizers, Photofrin and methylene blue (MB) have been used for PDT. 31 –34 However, Photofrin is not water soluble and exhibits nonspecific tissue accumulation and unexpected self-aggregation. Although conventional MB is water soluble, its poor rate of accumulation in cells or tissues is a major disadvantage. Despite these problems, the clinical application of PDT was established. However, PDT showed high morbidity and only superficial penetration. 30,35,36 In our previous study, nanoMB was proven to be a suitable alternative photosensitizing agent for PDT. 20
In a recent study, even though a breast tumor treated with PDT using nanoMB did not increase in size during the treatment period, the decrease in tumor volume was negligible. The reason for this is that the penetration depth was superficial at only about 1 cm and thus the treatment effect only occurred in the vicinity of the PDT laser insertion site.
To overcome the disadvantages of each procedure, we combined both procedures to treat breast cancer in a mouse model, which was shown to have a therapeutic effect. Laser ablation in the central zone and PDT in the peritumoral zone induced not only direct tumor necrosis but also negative margins. Based on these effects, a similar theory to cancer evaluation and marginal evaluation is established. We observed that the tumor volume slightly increased in the early phase of the combination treatment and continuously decreased after 3 days. However, after 9 days, the tumor volume was significantly decreased compared with that in the other groups. At the end of 15 days, there was almost no residual tumor burden.
As mentioned previously, this combined method could have therapeutic effects of not only directly affecting the center of the cancer by laser ablation but also managing the tumor margin by PDT. However, it is still unlikely that this can immediately replace actual surgery in clinical practice. As a limitation of the study, this study could not show statistical difference between PDT-treated group (III) and PDT with laser-ablated group (IV). However, because the decreasing pattern was obviously identified, we would figure out the significant effect of combination treatment with PDT and laser ablation with larger number of animals. Another limitation of this study is that because breast cancer has extremely heterogeneous characteristics, the treatment effect may differ depending on the cancer subtype. Mice with triple-negative breast cancer were cultured because of the subcutaneous inoculation of MDA-MB-231 cells in our previous study, and the results of this study may only be relevant to this type of breast cancer. Further study would be necessary to establish the efficacy of combination technique with laser and PDT for breast cancers.
Conclusions
The combination of laser ablation and PDT showed better results to single treatment by laser ablation or PDT. If further clinical trials can be performed on various cancer subtypes and this approach can be carefully expanded to human beings, it may be a good alternative for the conservative management of early or refractory breast cancer.
Footnotes
Acknowledgments
This research was supported by the Bio & Medical Technology Development Program of the National Research Foundation (NRF) funded by the Government of the Republic of Korea (MEST; No. 2009-0091573). And this research was also supported by a National Research Foundation (NRF) grant funded by the Government of the Republic of Korea (2014R1A5A2009242), a grant from the National R&D Program for Cancer Control, Ministry of Health and Welfare, Republic of Korea (1420040), INNOPOLIS Foundation grant funded by the Government of the Republic of Korea (MSIP; No. 2015DG0004), and a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HI16C0636).
Author Disclosure Statement
No competing financial interests exist.