
Abstract
Introduction
R
Appropriate treatment in the early stage of RCH is critical, and the therapeutic strategy is chosen according to the specific tumor characteristics, such as site, size, and associated complications. Reported treatments for RCH include focal photocoagulation (FPC), photodynamic therapy (PDT), transpupillary thermotherapy, cryotherapy, intraocular injection of antivascular endothelial growth factor (anti-VEGF) drugs or triamcinolone acetonide (TA), and vitreoretinal surgery. 8 –12 However, the long-term therapeutic results of these methods vary. FPC is applied for most small tumors in the peripheral area. Although photocoagulation is effective and widely used, it carries a high risk of bleeding and subretinal exudation and may not be suitable for RCH with local retinal detachment or for JCH. PDT has also been applied for the treatment of RCH. Hussain et al. conducted a retrospective analysis of six eyes from six patients treated with PDT and while response was inconsistent, they concluded that PDT could be used for the treatment of JCH. 13 Subretinal exudation or macular edema may occur during RCH progression or following treatment due to vasoproliferation and vessel leakage. Therefore, in addition to treatment of the tumor bodies, drugs that reduce vasoproliferation and vessel leakage, such as anti-VEGF and TA intravitreal injection, respectively, may also improve vision outcome.
Most previous reports on RCH treatment focused on photocoagulation or PDT monotherapy, while there are few reports on combination therapies. In the present study, we retrospectively analyzed the clinical features, treatment methods, tumor development, and vision outcomes of Chinese RCH patients receiving combined therapies, including PDT, FPC, and anti-VEGF or TA intravitreal injection, to provide more useful information to researchers and ophthalmologists for this complex rare disease.
Materials and Methods
General conditions
This was a retrospective study. Data collection, analysis, and publication were approved by the Ethics Committee of the Zhongshan Ophthalmic Center (No. 2016KYPJ028) according to the principles of the Declaration of Helsinki. Informed consent was obtained from all patients. Patients with RCH who underwent laser treatment and were followed up from November 2011 to December 2016 by the Zhongshan Ophthalmic Center Laser Treatment Department were considered candidates. Patients with other vision-affecting diseases (except ametropia) in RCH eyes, such as corneal disease, glaucoma, cataract, retinal diseases caused by other reason, or optic neuropathy, were excluded. A total of 10 eyes (from 8 RCH patients, 5 males and 3 females) were analyzed. The patient group included six treatment-naive patients and two patients with a history of previous laser treatment. All medical records were reviewed for clinicodemographic information, including age, sex, tumor number, treatment methods, vision outcomes, fundus images, fundus fluorescein angiography (FFA) results, and/or optical coherence tomography (OCT) results. Age at diagnosis ranged from 14 to 36 years (mean, 25.5). Average best corrected visual acuity (BCVA) at baseline was 0.55 ± 0.65 (logMAR). The follow-up time ranged from 12 to 120 months (including the long medical histories of the two previously treated patients), with a mean of 54.3 ± 29.8 months. No patient had severe systemic diseases, such as cerebral hemangioma, renal tumors, hypertension, or diabetes.
A total of 39 RCH tumor bodies were found and treated in these 10 eyes (3.9 ± 3.48 per eye). These included 37 peripheral RCH tumors (Fig. 1) and 2 JCH tumors (Fig. 2). Ten tumor bodies were classified as huge [body diameter >1 papilla disc (PD); Figs. 1 –3 and 5] and 29 as small tumor bodies (body diameter <1 PD; Fig. 4). Eight eyes exhibited macular complications, including five with macular exudates and edema, one with macular exudates, edema, and epiretinal membrane, one with macular epiretinal membrane, and one with macular exudates.
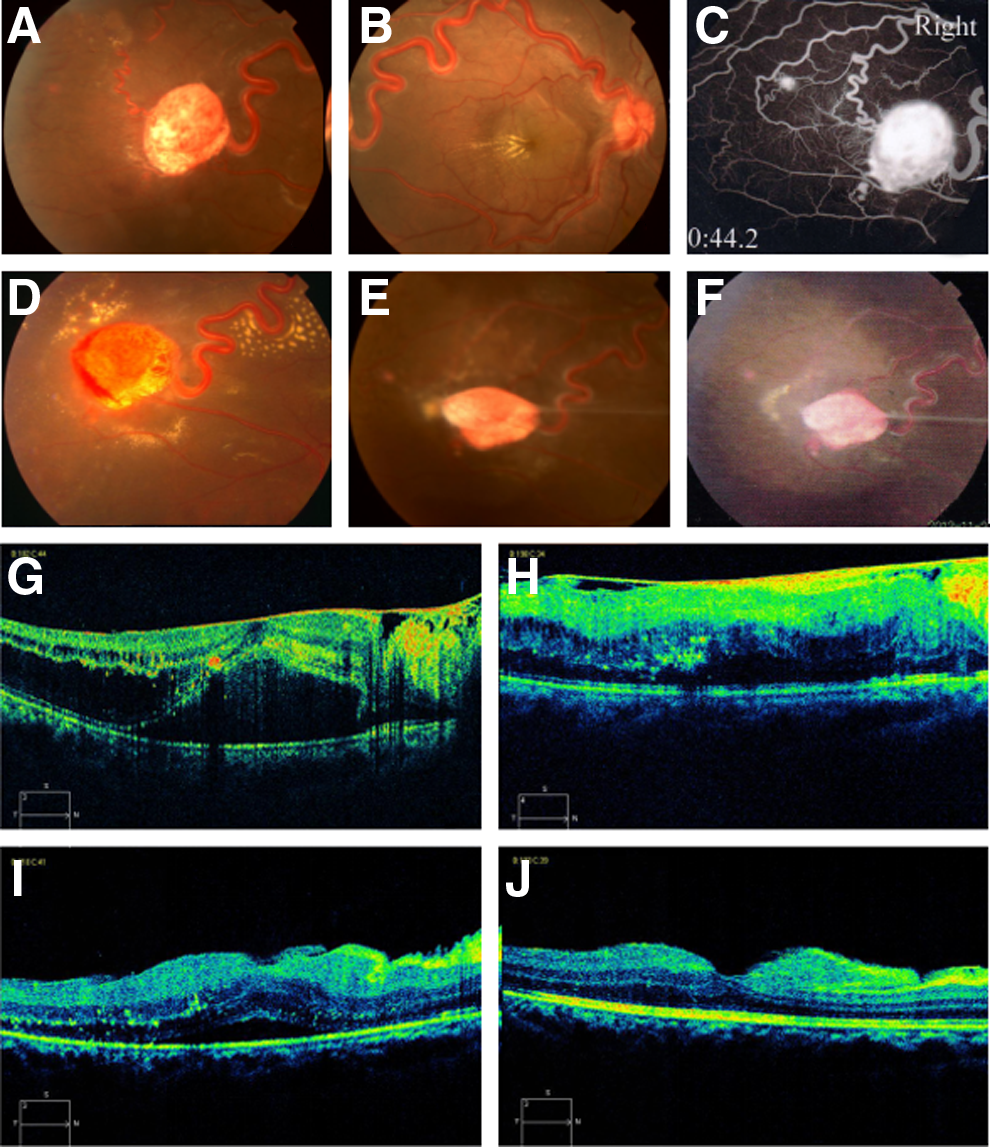
A typical case of huge RCH treated with PDT.
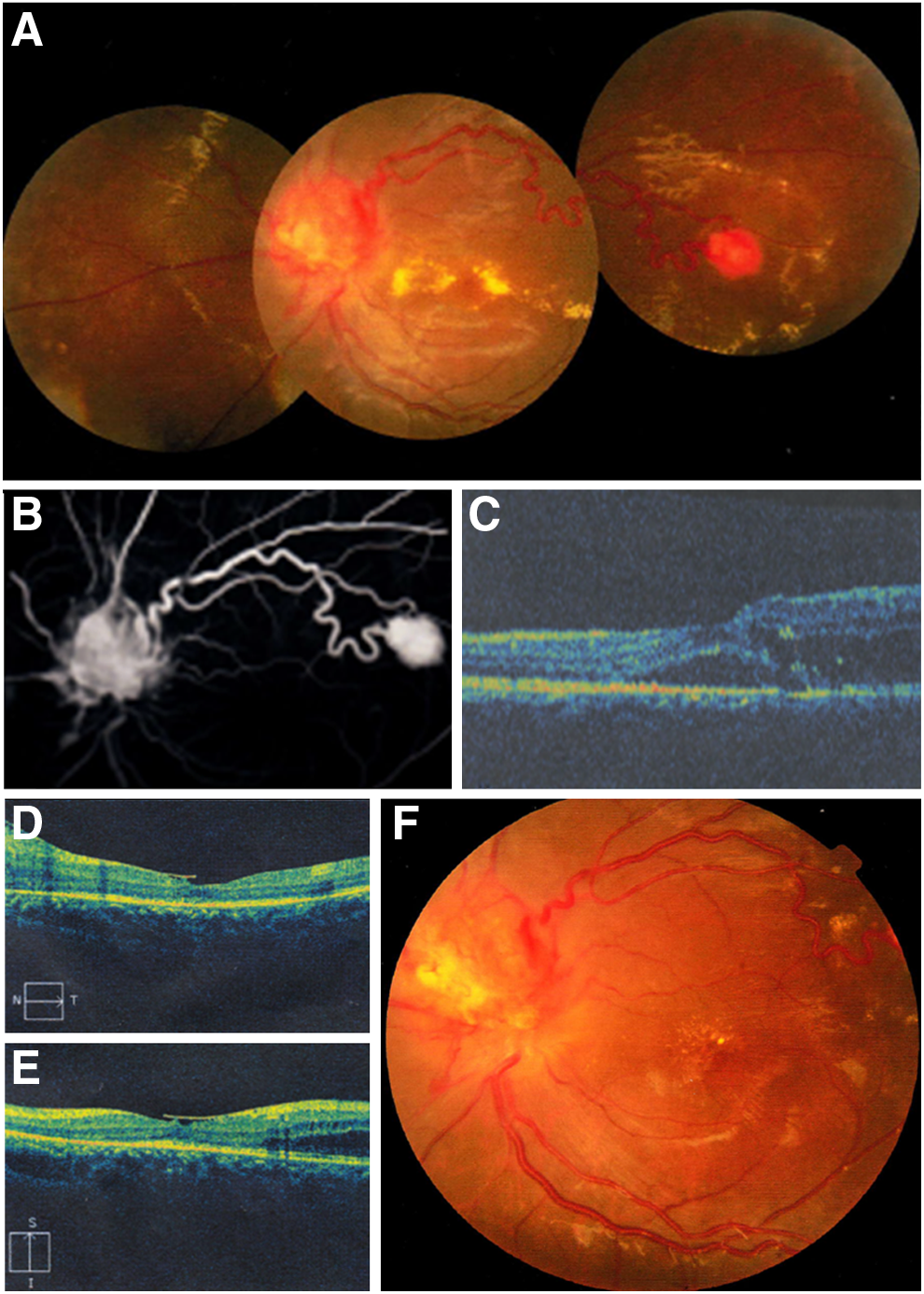
A typical case of JCH treated with PDT.
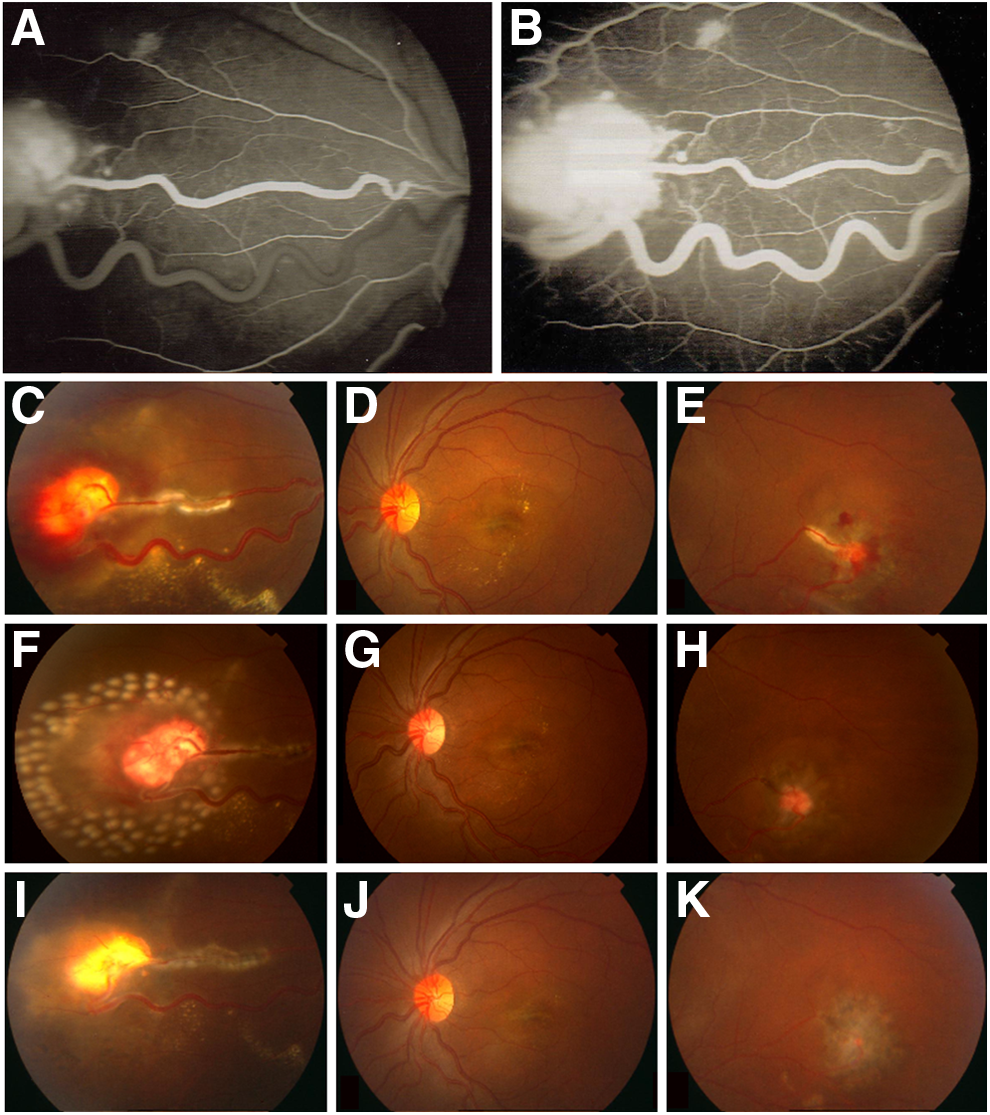
A patient with multiple RCHs, including a huge RCH treated with photocoagulation. (
A patient with recurrent RCHs treated with photocoagulation.
Before treatment, five of seven eyes with huge tumor bodies presented with exudative retinal detachment (and subretinal fluid) around the tumor bodies (Fig. 1C; Fig. 5). In the other two eyes with huge tumors, one developed exudative retinal detachment during the treatment period. Therefore, six of seven eyes with huge tumor bodies were complicated with exudative retinal detachment, while no exudative retinal detachment was observed in eyes with only small tumors.
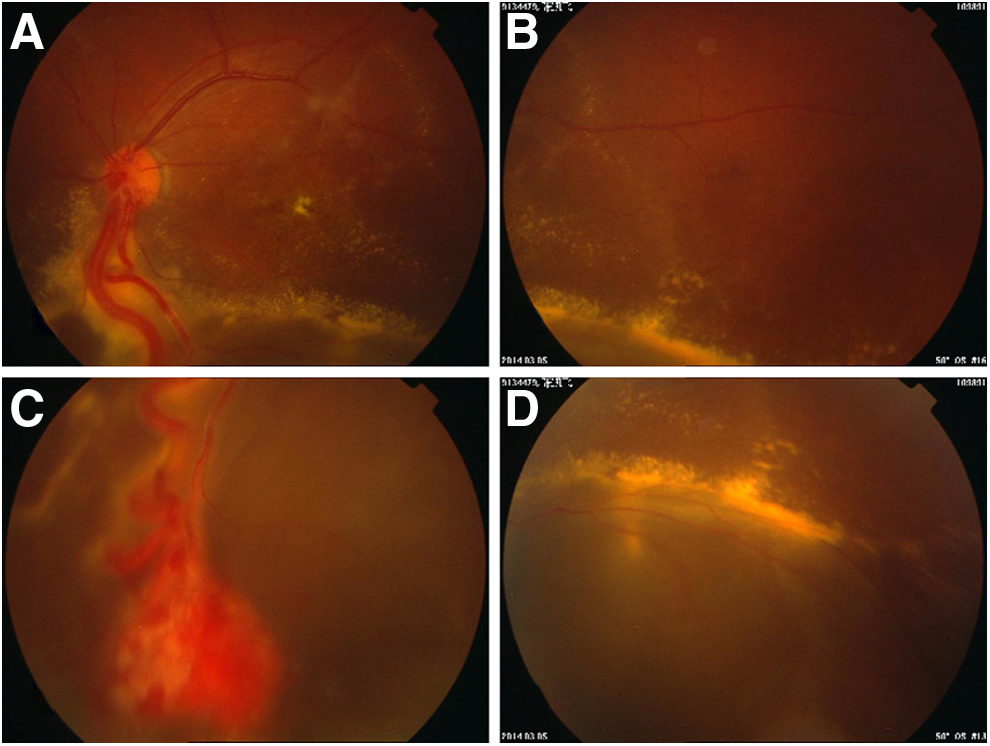
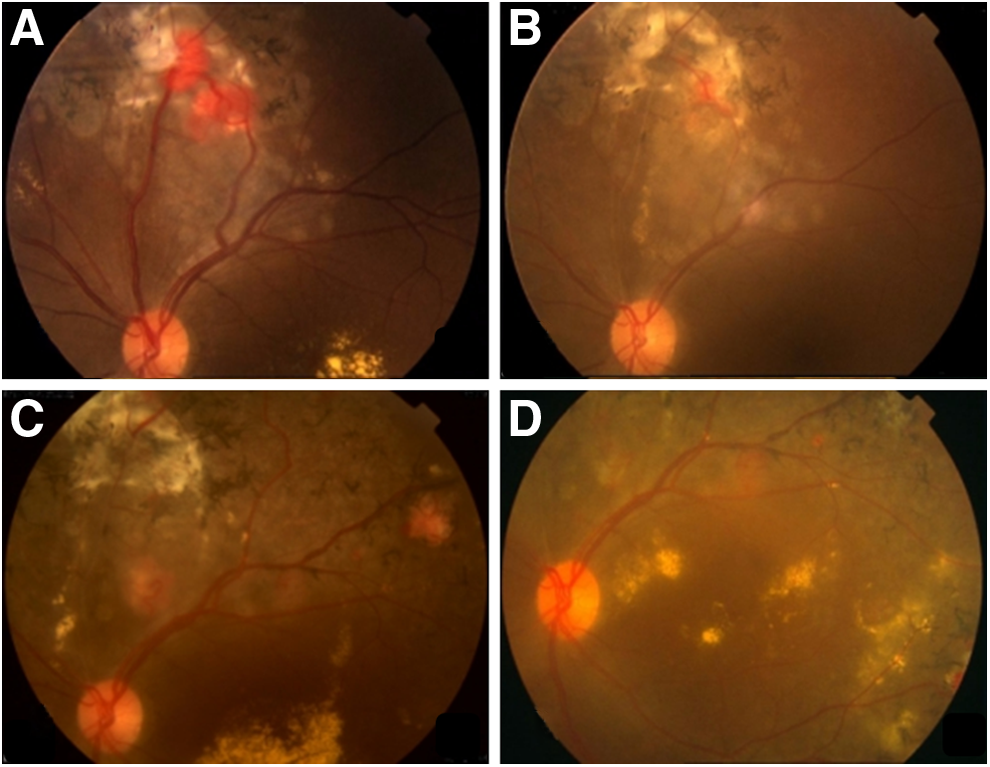
A huge tumor with tumor bleeding and severe local exudative retinal detachment after photocoagulation.
Treatment information
In addition to laser treatments (PDT and/or FPC), some patients received anti-VEGF or TA intravitreal injection, and one patient received vitreous surgery.
The PDT therapy was performed using verteporfin (Novartis, Switzerland) infusion at a dose of 6 mg/m2 body surface area for 10 min according to previous studies. 14,15 Five minutes after completion of infusion, light exposure was performed using the Opal PDT laser system (Lumenis, Inc., Israel) with a diode laser (689 nm) at an intensity of 600 mW/cm2. The whole RCH was covered by the laser spot. In this study, most patients received PDT with exposure time of 166 sec (archiving 100 J/cm2) performed by a single experienced laser doctor, while one patient received a single session of 83 sec (archiving 50 J/cm2) performed by another experienced laser doctor according to clinical judgment. Although both 83-sec (50 J/cm2) and 166-sec (100 J/cm2) exposures have been used for RCH, 13 –17 some studies have found 166-sec PDT more effective, especially when 83-sec PDT resulted in a poor response. 14,16 Therefore, 166-sec (100 J/cm2) PDT was used more frequently for RCH in these patients.
Photocoagulation was performed using a Zeiss Visulas 532 nm laser system (Zeiss, Germany). RCHs <1 PD were directly photocoagulated on the tumor body. For RCHs of diameter more than 1 PD, the nourishing artery was photocoagulated first, followed by tumor body photocoagulation until tumor atrophy or color fading occurred. For RCHs with localized exudative retinal detachment, the back boundary of detachment was coagulated. During FPC, light spot size was 200–500 μm, energy 0.12–0.4 mW, and exposure time 0.1–1 sec. The tumor body turned white after photocoagulation, while other photocoagulated areas turned gray.
Intraocular injection of anti-VEGF (0.5 mg ranibizumab; Novartis or 0.5 mg bevacizumab; Roche, Switzerland) or TA (2 mg; Zhejiang Xianju Pharmaceutical Co. Ltd., China) was applied for complications such as severe subretinal fluid caused by RCH or arising during RCH treatment. One patient received vitreous surgery according to his medical situation.
OCT examination was performed using a Zeiss Cirrus 4000 OCT system (Zeiss) in high-resolution B-scan mode through the macular fovea. The vertical and horizontal scan results were analyzed by an OCT doctor and reviewed by our research group to evaluate the outcomes of macular exudation and subretinal fluid formation.
A total of 11 sessions of PDT and 25 sessions of FPC were applied. Five eyes (three patients) receiving PDT with additional photocoagulation or anti-VEGF according to the clinical situation were classified as the PDT-based group. The other five eyes (five patients) receiving laser therapy without PDT were classified as the FPC-based group.
The PDT-based group received 11 sessions of PDT, 5 sessions of FPC, and 2 anti-VEGF IVJs. The FPC-based eyes received a total of 20 FPC sessions, 3 anti-VEGF or TA intravitreal injections (IVJs), and 1 vitreoretinal surgery without any PDT (Table 1).
FPC, focal photocoagulation; IVJ, anti-VEGF or TA intravitreal injection; PDT, photodynamic therapy.
Statistical analyses
All statistical analyses were performed using SPSS 16.0 software package. Chi-square and Fisher's exact tests were used to compare nonparametric data or proportions between two groups. Last-visit BCVA was compared to baseline BCVA using the related samples Wilcoxon signed-rank test. Pearson correlation analysis was applied to identify possible relationships between clinicodemographic factors and baseline or last-visit BCVA.
Results
Tumor responses and vision outcomes
Of the 10 RCH eyes reviewed, 8 presented with stable tumor bodies, while 2 exhibited active tumors at last visit. Of 39 tumor bodies examined, 35 (89.7%) had regressed (Fig. 1E and F; Fig. 3I and K) or were stable (Fig. 2F; Fig. 4D) at last follow-up, while 4 (10.3%) had recurred.
During follow-up, nine eyes showed some visual improvement (logMAR value decreased) and only one eye showed reduced visual acuity (logMAR value increased) due to vitreous hemorrhage and exudative retinal detachment after photocoagulation. By the end of follow-up, however, four of these nine eyes exhibited reduced vision acuity compared to baseline. Therefore at last visit, vision in five eyes was classified as stable or improved, and vision in five eyes was reduced. The mean last-visit vision of these 10 eyes was slightly worse than baseline (logMAR 0.72 ± 0.53 vs. 0.55 ± 0.65), but the difference did not reach significance (p = 0.484 by Wilcoxon signed-rank test).
Of the 10 RCH eyes reviewed, 4 (40%) exhibited a final BCVA worse than 1.0 logMAR, and most of these were complicated by macular disorders or exudative retinal detachment. The other six eyes had a last-visit BCVA better than 1.0 logMAR, including two eyes better than 0.0 logMAR. However, these two eyes with last-visit BCVA better than 0.0 logMAR also had better baseline BCVA. In addition, the tumors were small, fewer in number, and farther away from the macular and optic papilla areas.
Effects of different laser-based treatments on tumors and vision
Although the PDT-based group was younger than the FPC-based group (16.8 ± 6.26 vs. 29.6 ± 5.08 years, p = 0.099), average tumor number, average huge tumor number, and average small tumor number per eye were similar between groups (Table 2).
The data of age, follow-up, tumor no., huge tumor no., small tumor no. are expressed as mean ± SD. Follow-up data, months.
SD, standard deviation.
Of the 10 RCH eyes, 6 (3 eyes in each group) achieved good RCH control with no recurrence during the entire follow-up period, while 4 eyes exhibited RCH recurrence (2 eyes in each group). Of these recurrences, two were controlled at last visit. Therefore, tumors in eight eyes were well controlled at last visit, while only two eyes with four RCHs, one eye in the PDT-based group with one huge tumor, and one eye in the FPC-based group with one huge tumor and two small tumors were active at last visit (Table 3).
The data baseline VA and last-visit VA are expressed as mean ± SD. Baseline VA and last-visit VA mean the best corrected vision acuity value of logMAR. VA improved means VA logMAR value decreased, VA stable means no change to VA value, and VA worse means logMAR value increased. Controlled means RCHs were stabled or depressed. Uncontrolled means RCHs progressed or were recurrent.
VA is equal to BCVA in this article.
BCVA, best corrected visual acuity; RCH, retinal capillary hemangioma; VA, visual acuity.
The baseline BCVA logMAR value did not differ significantly between PDT-based and FPC-based groups (0.52 ± 0.85 vs. 0.57 ± 0.47, p = 0.675 by Chi-square test). The last-visit BCVA logMAR value was also similar to baseline BCVA in the PDT-based group (0.44 ± 0.59 vs. 0.52 ± 0.85, p = 1.0 by Wilcoxon signed-rank test). In contrast, the last-visit BCVA logMAR value in the FPC-based group was above baseline (0.99 ± 0.32 vs. 0.57 ± 0.47, p = 0.273 by Wilcoxon signed-rank test), suggesting worsened vision, although the difference did not reach statistical significance. Further, last-visit logMAR visual acuity (VA) value was lower in PDT-based group than the FPC-based group (0.44 ± 0.59 vs. 0.99 ± 0.32), suggesting better vision outcomes using PDT-based therapy, although again the difference did not reach significance.
Vision of all five eyes in the PDT-based group was improved at some point or remained stable during the treatment and follow-up periods. However two eyes eventually exhibited decreased VA (increased logMAR value) during the follow-up period due to tumor recurrence and formation of macular epiretinal membrane and exudative retinal detachment. Therefore, at the last visit, vision was improved or remained stable in three of five eyes in the PDT-based group.
Of the five eyes in the FPC-based group, four showed some visual acuity improvement during the follow-up period, while the remaining one eye with exudative retinal detachment and vitreous hemorrhage showed vision deterioration even at the beginning of follow-up. In the four eyes with improved or stable visual acuity at the early stage following treatment, two showed stable or improved VA at last visit, while two eyes showed decreased vision at last visit, both of which had tumor recurrence. Therefore, in the FPC-based group, visual acuity was improved or remained stable in two eyes and decreased in three eyes at the end of follow-up (Table 3).
Complications during treatment and follow-up
Main complications that may relate to the treatments included hemorrhage (Fig. 3C and E; Fig. 5C) and subretinal fluid increase (Fig. 5D). Other complications that appeared gradually after laser treatment included vitreous proliferation (Fig. 1E and F) and macular exudates (Fig. 4C), which may be caused by the tumors rather than directly by the laser treatments. Intraocular hemorrhage occurred in four eyes (40%), increased subretinal fluid in four eyes (40%), and other complications such as macular exudation and vitreous proliferative membrane formation in five eyes (50%).
No tumor bleeding or vitreous hemorrhage was observed following any of the 11 PDT sessions, but one eye exhibited vitreous proliferation and one eye slightly increased subretinal fluid. A total of 25 FPC sessions were conducted, including 20 sessions in 5 FPC group eyes and 5 sessions in 2 PDT group eyes. After FPC treatment, four eyes exhibited tumor bleeding and vitreous hemorrhage; three eyes deteriorated subretinal fluid and one eye vitreous proliferation (Table 4).
Treatment related means complications appear or be more severe after treatment. One eye in PDT groups presented bleeding and subretinal fluid deteriorated after FPC treatment, therefore these complications were considered as FPC related.
Factors related to vision outcomes
Eyes with low baseline VA or reduced VA posttreatment frequently exhibited huge tumors, macular complications, subretinal fluid accumulation, and vitreous hemorrhage. Due to the small case size of this study, no factors were significantly correlated to baseline visual acuity. However, RCH with macular exudates was weakly correlated with low baseline BCVA (or higher logMAR value, r = 0.61, p = 0.06). Similarly, macular edema was weakly associated with low baseline BCVA (or higher logMAR value, r = 0.54, p = 0.11).
Correlation analysis on clinicodemographic factors that may impact last-visit vision outcome revealed a significant correlation between higher visual acuity (lower logMAR) and age at first treatment (r = 0.66, p = 0.04). In contrast, lower acuity (high logMAR) was associated with the presence of subretinal fluid before treatment (r = 0.69, p = 0.03) and the use of anti-VEGF or TA intravitreal injection (r = 0.66, p = 0.04). Thus, young age at first treatment is predictive of better prognosis and subretinal fluid accumulation at baseline (and need for targeted treatment) with worse prognosis. Although tumor size may also influence prognosis, the correlation did not reach statistical significance (r = 0.53, p = 0.12). Subretinal fluid accumulation was strongly correlated with larger RCH tumor size, and large RCHs were usually complicated with subretinal fluid both at baseline (r = 0.67, p = 0.03) and after treatment (r = 0.68, p = 0.02), so tumor size may affect prognosis indirectly. There were also weak associations between posttreatment VA and baseline macular edema (r = 0.42, p = 0.22), baseline macular exudates (r = 0.44, p = 0.20), and the selection of treatment modalities, including laser photocoagulation (r = 0.49, p = 0.15) or PDT (r = −0.48, p = 0.16). Baseline vision showed no significant correlation with visual prognosis (r = 0.10, p = 0.79; Table 5).
Indicates that p-value is <0.05.
JCH, juxtapapillary capillary hemangioma.
Clinical results of JCH
JCH locates near to the optic disc, which may directly compress the optic nerve or induce macular edema. Treatment of JCH is difficult, and the results are variable. In our study, two eyes (20%) had JCH, both treated with PDT and other combination therapies. The vision of one eye was improved from 0.52 to 0.2 logMAR after the first session of PDT and remained stable for almost 1 year (Fig. 2) before recurrence and appearance of subretinal fluid. After another session of PDT on this JCH and a huge tumor near the macular area, as well as injection of anti-VEGF for subretinal fluid, both the JCH and huge tumor started to regress but the macular subretinal fluid did not disappear. As small tumor bodies can also cause subretinal fluid accumulation, a session of photocoagulation on multiple small tumor bodies was added, which resulted in slow reabsorption of subretinal fluid. However, macular epiretinal membrane was found and persisted, and vision was poor at last visit (1.3 logMAR). In the other patient, vision in the RCH eye was 0.2 logMAR at baseline and was improved slightly to 0.15 logMAR after laser treatment. During long-term follow-up, the tumor recurred, and vision slowly decreased (logMAR increased to 0.7 by last visit). However, due to the small number of JCH cases, we cannot draw any firm conclusions on treatment efficacy.
Discussion
RCH is a rare vision-threatening disease. The treatment strategy for RCH is chosen according to tumor characteristics. Laser photocoagulation is still widely used for most peripheral RCHs. In this study, five RCH eyes were treated by photocoagulation-based treatment, of which three (60%) exhibited tumor control, one (20%) remained active (recurrent) at last visit, and one (20%) required vitreoretinal surgery. Of all tumors treated by photocoagulation, 82.4% (14 of 17) were controlled at last visit. Considering that one huge tumor in this group was treated with vitreoretinal surgery, the exact tumor control rate by photocoagulation was 76.5% (13 of 17), similar to the rate (74%, 26 of 35) reported by Singh et al. 8 Although photocoagulation was effective for most peripheral RCHs, some complications were found in our study, including bleeding and subretinal fluid accumulation. One case with a huge RCH displayed severe complications following FPC, including hemorrhage and exudative retina detachment, which could not be controlled by anti-VEGF and TA injection. These complications were resolved by vitreoretinal surgery. Despite treatment, vision outcome was still poor (1.3 logMAR).
PDT is used with increasing frequency for the treatment of RCH, especially for large tumor bodies or JCH. The dose of photosensitizer (verteporfin), laser intensity, spot size, and other parameters were the same as in previously reported cases. Different exposure times, including 83 sec (a total laser energy of 50 J/cm2) and 166 sec (100 J/cm2), have been reported and both were effective for RCH. It was found that when treatment with 83-sec PDT was ineffective, 166-sec exposure induced a stronger effect and inhibited RCH progression. 13 –15 Further, 166-sec PDT (100 J/cm2) did not induce additional complications. 16
Schmidt-Erfurth et al. 17 reported tumor regression with resolution of macular exudates and serous retinal detachment in five eyes from five patients initially showing solitary capillary hemangioma on the temporal optic nerve accompanied by exudative decompensation and decreased visual acuity at 12 months post-PDT (100 J/cm2, same as 600 mW/cm2 × 166 sec, the same exposure as in our study). In addition, VA was increased or stable in two eyes (but decreased in three eyes). 17 A retrospective analysis of six eyes of six patients treated with PDT, including five with 83-sec exposure time (50 J/cm2) and one with initial 83-sec PDT followed by two sessions of 166-sec PDT (100 J/cm2) due to poor response, found tumor regression or stabilization in five eyes (two regressed and three stable) and tumor progression in one eye despite PDT and subsequent cryotherapy at follow-up (24–60 months; mean, 36). 13 The later unresponsive RCH tumor received PDT with 83-sec exposure. Thus, visual acuity was improved in only two eyes following PDT, while three eyes showed deterioration.
In the current retrospective analysis, the one patient receiving a single session of PDT with 83-sec exposure showed tumor recurrence at 6 months following an initial period of regression. This patient received another two sessions of PDT with 166-sec exposure time, which resulted in tumor regression and stability for 24 months. For all other PDT treatments, the exposure time was 166 sec, and each session was performed by the same experienced doctor. In our PDT-based treatment group, all eyes exhibited tumor control (tumor was regressed or stable) for a substantial period after treatment, and 80% (4 of 5) of RCH eyes were still controlled and stable at final follow-up. Moreover, 60% (3 of 5) showed stable or improved vision. Considering our results and the aforementioned studies, it can be concluded that both 166-sec (100 J/cm2) and 83-sec (50 J/cm2) PDT are effective for control of most RCHs, while 166 sec has a stronger effect in cases showing poor response to 83-sec PDT.
We found that PDT is safer than FPC for RCH treatment. Reported complications of PDT include transiently increased subretinal fluid, macular edema, increased hard exudates, retinal edema, and subretinal hemorrhage around the lesions. 18,19 In the current study, we found transiently increased subretinal fluid in only one RCH eye, which disappeared after anti-VEGF treatment and one session of photocoagulation. Moreover, no severe complications such as vitreous hemorrhage or severe retinal detachment were noted.
This study included two JCH eyes, both treated with PDT-based combination therapies. JCH is a difficult type of RCH to treat as it is near or over the optic nerve head and so presents a high risk for vision loss secondary to subretinal and intraretinal fluid accumulation, epiretinal membrane, and exudative retinal detachment. Both PDT and anti-VEGF treatments have been used for JCH, but the results were not always satisfying. 13,17,20,21 In our study, PDT-based treatment inhibited JCH progression and improved visual acuity in the short term. However, vision in both JCH eyes ultimately decreased because of complications. Therefore, the long-term efficacy of PDT-based treatment for JCH appears to be poor.
We also conducted correlation analysis to identify possible factors related to RCH prognosis. Younger age at first treatment was one important factor associated with good vision outcome. Another important factor was the prolonged presence of subretinal fluid (especially exudative retinal detachment) at baseline, which indicated poor vision outcome. Although anti-VEGF or TA intraocular injection may reduce subretinal exudation or accelerate the absorption of macular edema, it did not improve vision at long-term follow-up. Subretinal fluid accumulation was strongly correlated with larger RCH tumor size, both before and after treatment, which may affect vision prognosis. However, we found no significant difference in vision outcome between PDT- and FPC-based therapies due to the small sample size and intragroup variation.
Limitations of this study include the retrospective design, lack of strict control between two laser-based treatments, and the small sample size. Thus, our conclusions are relatively limited. A prospective clinical study on this area should be done in the future to provide more effective evidences.
Conclusions
Although good long-term vision outcomes were obtained in some peripheral RCH cases after treatment, deterioration of vision was observed in other cases even when the tumor body regressed or was stable, and complications such as macular edema and exudates were resolved. It is hard to compare the effects of different treatment methods on visual acuity due to lack of strict control of the research; however, laser photocoagulation may carry a higher risk of bleeding and severe subretinal fluid accumulation, which may indirectly lead to poor vision outcome. Therefore, PDT should be recommended for RCH if available. It is clear that more effective therapies are required for difficult RCH cases, including JCH and those with exudative retinal detachment or macular edema.
Footnotes
Acknowledgments
This study was supported by the Medical Scientific Research Foundation of Guangdong Province, China (A2015162), and by the Natural Science Foundation of Guangdong Province, China (2016A030313344). The authors thank Dr. Hui Xiao of Zhongshan Ophthalmic Center, Sun Yat-sen University for help with OCT result analysis.
Author Disclosure Statement
No conflicts of interest are declared.