
Abstract
Introduction
T
The use of low-dose biophotonics therapy, termed photobiomodulation (PBM) therapy, has been shown to reduce pain and inflammation, promote repair, and prevent fibrosis. 5 This therapy was previously known as low-level light/laser therapy. There have been recent advances in our understanding of the biological mechanisms that includes activation of a range of molecular targets such as cytochrome c oxidase, Latent transforming growth factor beta 1 (TGF-β1), and Opsin 4. 6 –8 These chromophores are known to mediate specific biological cascades such as reactive oxygen species (ROS) generation, ATP synthesis, and signal transduction. These, in turn, can potently modulate a broad range of biological responses such as pain, inflammation, immunomodulation, wound healing, and tissue regeneration. Despite the availability of PBM devices for more than six decades, limited research in mechanisms of action, the complexity of disease-specific biological mechanisms, as well as nuances in treatment delivery have prevented its acceptance as a mainstream therapy. 9 Further, clinical studies for PBM therapy for trismus have noted limited, often inefficacious, clinical outcomes, and, therefore, more well-designed human studies are critical. 10 –13
We recently reported a case series of patients with oral mucosal and salivary gland cGVHD that included management with PBM therapy in cases that did not respond to conventional systemic and topical therapy of GVHD. 14 The current report focuses on the management of fibrosis that may be seen in cGVHD where treatment included PBM. We report two cases with severe oral cGVHD associated with trismus (mouth opening of 35 mm or less), intraoral fibrous bands, and severe dysphagia that were effectively managed with PBM therapy.
Case Report 1
A 12-year-old male with acute myeloid leukemia (M1, CD33 positive) received an allogeneic-matched unrelated donor HSCT conditioned with total body irradiation (TBI)/cyclophosphamide. He developed acute GVHD (Grade 4) involving the skin, liver, and gut. cytomegalovirus (CMV) viremia and episodes of respiratory distress were noted. He then developed chronic GVHD and was seen 3½ years post-HSCT due to cGVHD with sclerodermatous features, bronchiolitis obliterans, dysphagia, cataracts, and oral involvement. Diagnoses included secondary hypertension and gingivitis. He did not report having a dry mouth, and no clinical evidence of hyposalivation was apparent. A lip biopsy was not necessary to establish a diagnoses in this case with a clear medical history, whereas a tongue biopsy was performed due to evident clinical changes that confirmed oral cGVHD with involvement of proximal esophagus. Due to oral and esophageal GVHD in addition to sclerodermatous changes, he had significant dysphagia and obtained majority of his nutrition via G-tube, except for limited liquid intake by mouth. He had difficulty with choking on attempted oral intake and had experienced several episodes of aspiration pneumonia. He had a single episode of balloon esophageal dilation, but this was not successful and symptoms continued. When seen for oral cGVHD, his medications had included prednisone (20 mg/day), sirolimus (0.5 mg), megestrol, atovaquone, methadone (5 mg/5 mL solution-3 mL, as needed), dexamethasone rinse (0.5 mg/5 mL), omeprazole, morphine (10 mg/5 mL; 7.5 mL qid prn), methadone (5 mg/5 mL, 5 mL BID), lisinopril, lorazepam, tacrolimus 0.05% ointment, and ondansetron. Medical management had previously included plaquenil and methotrexate, and Psoralen UV-A (PUVA) therapy and photopheresis. Opioid analgesics were required daily due to oral and pharyngeal pain. He was undergoing physiotherapy and speech therapy that included ultrasound, heat, massage, range of motion exercise, and movement against resistance. Physiotherapy for limited jaw movement was associated with benefit.
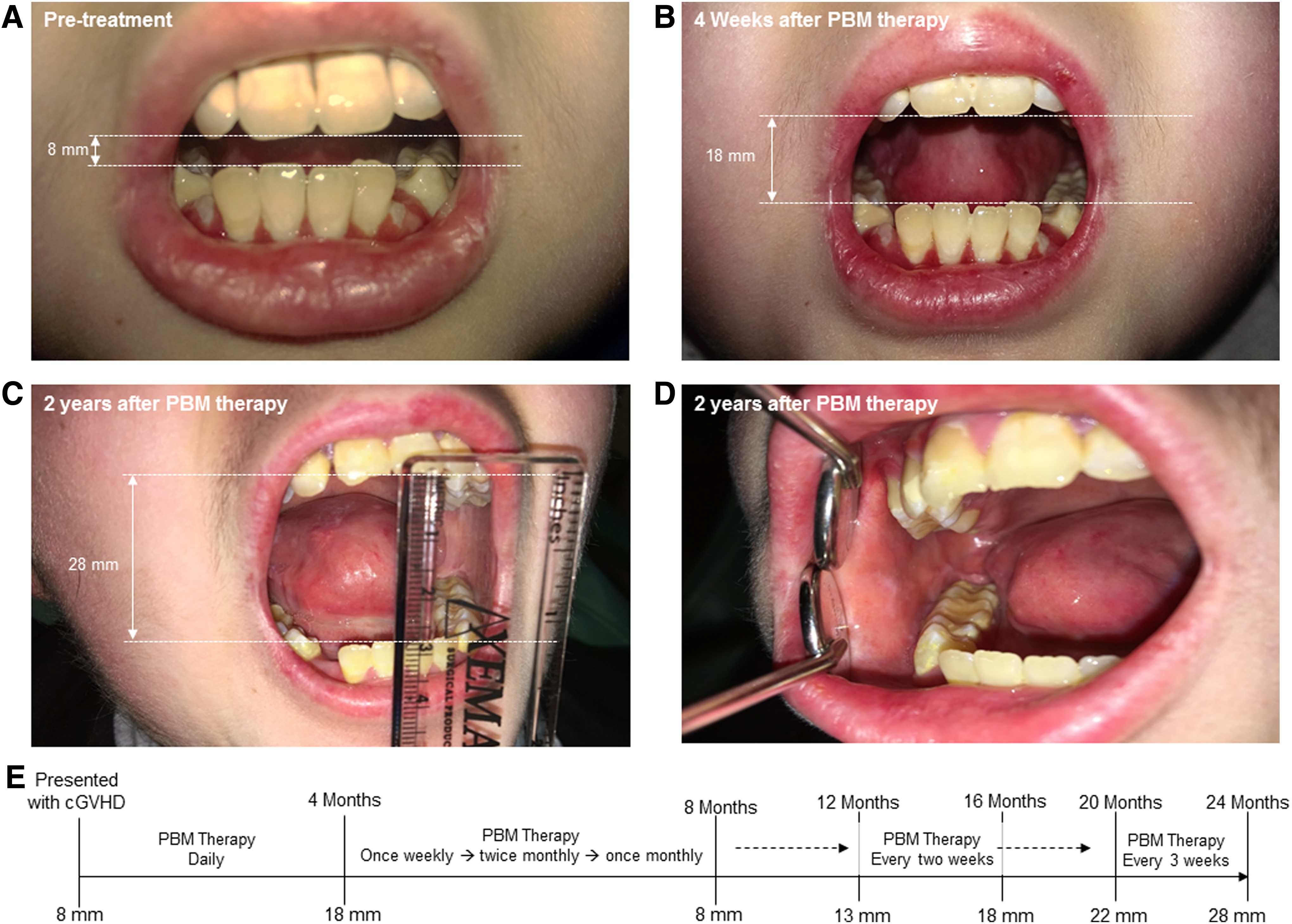
Before beginning PBM therapy, his NIH cGVHD total score was 6, and maximum oral pain was reported as VAS 6–7/10 despite continuing opioid analgesics. 15 Ulceration was present on the cheeks and lateral border of the tongue associated with severe erythema, and edema of gingival tissue with spontaneous bleeding of the maxillary and mandibular attached gingiva was present (Fig. 1A). He did not experience dry mouth, clinically the oral mucosa appeared moist, and a saliva pool was present in the floor of mouth on examination. Prominent, palpable taut linear bands consistent with sclerodermatous changes were present in posterior buccal mucosa bilaterally that limited width of the buccal vestibules on either side. Maximum interincisal range of movement (ROM) was severely limited (intercisal opening <8 mm). The severe pain and restricted ROM complicated performing good oral hygiene.
Treatments were performed at all sites of oral mucosal involvement with the intraoral and extraoral approach that included cheeks, cervical lymph node chain, and to the throat up to the region of the thyroid gland with the bilateral approach. PBM therapy was performed by using a commercially available PBM treatment unit from THOR Photomedicine Ltd (Chesham, Buckinghamshire, United Kingdom). A combination of two different treatment probes was used; namely, for intraoral use, a 660 nm laser probe power at 75 milliwatt (mW), pulsed 2.5 Hertz (Hz), and spot size of 2.5 cm2 with an effective treatment surface irradiance of 30 mW/cm2 for irradiation time of 60 sec per point, energy 4.5 Joules (J) per point, and energy density 1.8 J/cm2. Extraorally, a cluster of 69 light emitting diodes (LEDs) containing 660 and 850 nm LEDs, total power at 1390 mW, pulsed 2.5 Hz, illuminated area 28 cm2, average irradiance 50 mW/cm2, irradiation time 60 sec, energy 83.4 J, and energy density 3 J/cm2 were used.
After 4 weeks of PBM therapy performed twice weekly, the NIH cGVHD score was 3 with mild ulceration and erythema. Oral pain (VAS 3/10) was improved, methadone was reduced to once daily, and morphine continued BID. The patient reported a cautious increase in oral intake and was able to take liquids by mouth due to reduced oral pain. However, he continued to experience choking on oral intake and remained dependent on the G-tube. Due to reduced oral pain, oral hygiene improved with decreased intensity of gingival erythema. He had increased interincisal opening of 18 mm that could be attributed to combined PBM and physiotherapy (Fig. 1B). As his symptoms improved significantly, PBM therapy was reduced to once weekly, with increased time between visits to twice monthly and finally, after 4 months to once monthly. Physiotherapy for jaw limitation was discontinued.
On a monthly PBM treatment schedule, symptoms of sore mouth and dysphagia, increased and mucosal erythema with minor ulcerations recurred. Due to this, the frequency of PBM therapy visits was increased to twice monthly with improvement. During this time, topical budesonide was continued, and opioid use was reduced. When symptoms again improved, increased time between PBM therapy visits was scheduled and initially, he appeared stable for oral GVHD based on symptoms and clinical findings. However, when visits were decreased to once monthly, oral erosions occurred in areas of the cheeks or tongue and frequency of PBM treatment was again increased to twice monthly. The schedule of morphine use was reduced to once daily, and methadone was discontinued as oral mucosal cGVHD improved. Maximum jaw opening progressively improved from 8 mm before PBM therapy to 13 mm after 4 months of treatment followed by 14 mm after 8 months, and increased flexibility of cheeks was noted. At 1 year after PBM and physiotherapy, jaw opening was noted to be 18 mm. At 18 months, he was assessed for dysphagia with possible plans for dilation, he had been initiated on plaquenil, and a prior trial of Gleevec was discontinued due to nausea and emesis. Repeated esophageal dilation was considered based on the choking episodes and findings of a restricted esophageal aperture of 2 mm on a swallow study. However, this was not repeated due to limited success of prior dilation treatment and a concurrent increase in jaw opening that reportedly decreased choking and improved his oral intake.
After one additional year of PBM therapy every 3–4 weeks, jaw opening increased on a gradual basis to a maximum of 22 mm and normal diet, with no history of choking on food for approximately 1 year and return to full diet. When PBM therapy was scheduled every 3 weeks, GVHD was stable with mild nonspecific erythema and gingivitis, with rare isolated mucosal erosions, and a progressive increase in ROM of the jaw and resolution of dysphagia was seen. Over a 2-year period, he had a gradual increase in the range of jaw opening with PBM despite physiotherapy being discontinued, with a maximum opening measured at 28 mm (Fig. 1C). The submucosal bands in the posterior buccal mucosa became less prominent on the right, and it became nonpalpable on the left. Increased vestibular depth and width were noted that increased the ease of performing oral hygiene (Fig. 1D). Dysphagia improved significantly, and he required less time to complete meals with no choking incidents. His diet had increased texture and he had returned to his routine, pre-HSCT diet. An outline of the progression of cGVHD restriction of mouth opening as well as responses to PBM therapy are presented (Fig. 1E).
Case Report 2
A woman born in 1986 who was diagnosed with pre-B-cell acute lymphocytic leukemia received an allogeneic HSCT from a 9/10 matched unrelated donor after myeloablative conditioning with TBI/cyclophosphamide in 2010. She developed acute GVHD of the oral cavity and the skin. In 2011, severe cGVHD manifested with extensive scleroderma, sicca syndrome, and bronchiolitis obliterans, for which she was treated with prednisone, rituximab, imatinib, ultraviolet therapy, and extracorporal photopheresis with limited success.
In 2014, she was referred for treatment of caries of the anterior teeth under general anesthesia, due to the patient's fear of injections for local anesthesia. She presented with severe sclerodermatous changes involving the face, resulting in a limited mouth opening (20–22 mm) and severely reduced lip and cheek mobility with an inadequate lip closure, resulting in drooling. The limited mouth opening hindered a comprehensive intraoral exam and objective scoring of oral cGVHD severity. Nevertheless, erythema and ulcerations could be observed at the anterior buccal mucosae and tongue. A limited mouth opening and highly sensitive mucosae also hampered oral hygiene measures and professional preventive measures. Her vermillion lips were hyperkeratotic, stiff, and swollen; lesions were present. Physiotherapy for mouth opening was suggested (TheraBite) but this resulted in angular lesions, which were slow to heal, and compliance was low. Her skin was sclerotic, with painful ulcerations manifesting at her abdomen. The range of motion of her wrists and elbows was very limited, for which she was treated with physical therapy. Methotrexate (MTX, 10 mg/week) was added to the immunosuppressive regimen, but GVHD progressed and when she was hospitalized with a Staphylococcus epidermidis bacteremia and MTX treatment was discontinued.
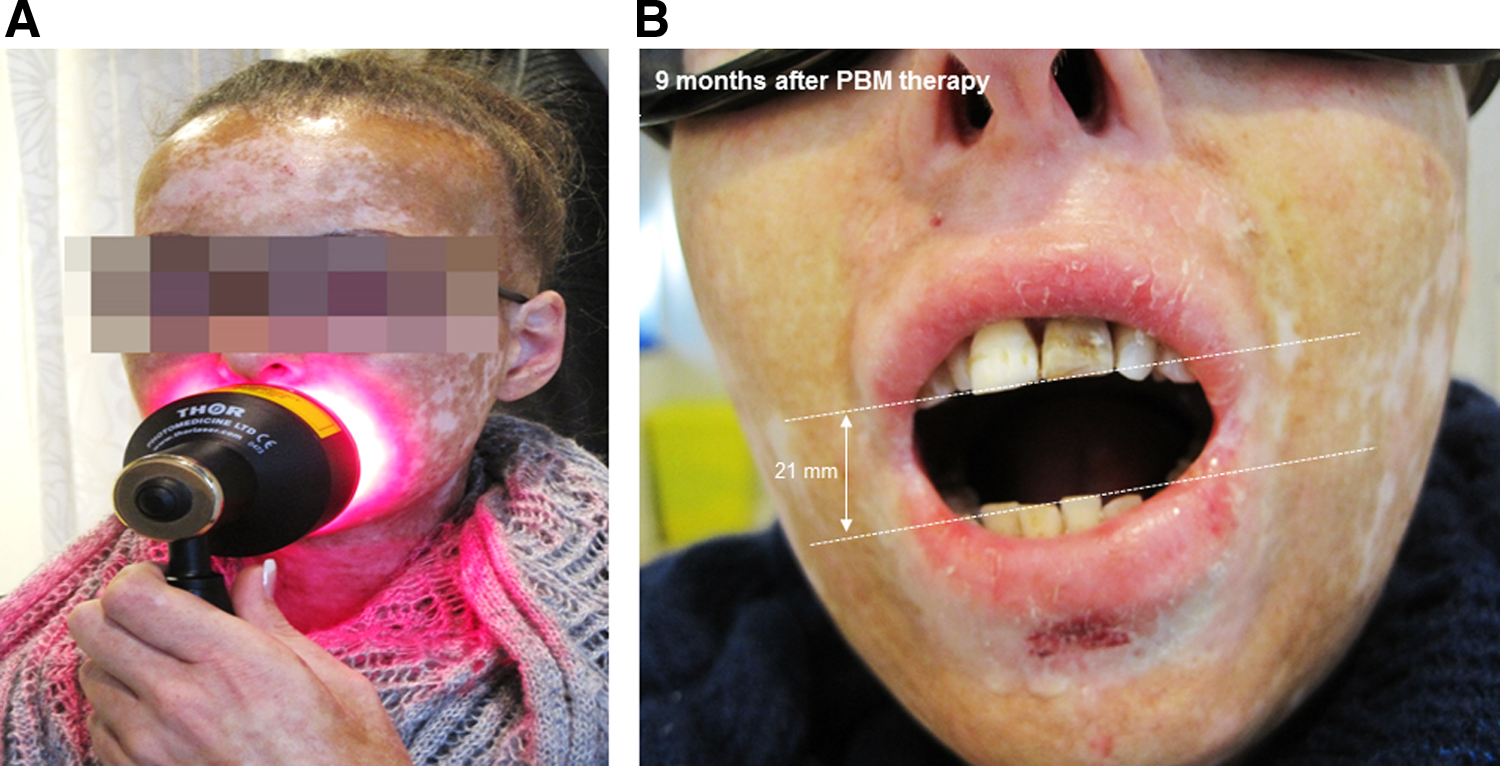
In 2015, she was referred for oral cGVHD. We were not able to assess the oral NIH cGVHD total score due to the limited mouth opening. Unstimulated salivary flow was 0.2 mL/min; stimulated salivary flow was not assessed as she could not tolerate stimulation with flavorless chewing gum. The interincisal mouth opening was 17 mm. She was reluctant to use any topical oral agents, due to mucosal sensitivity (VAS 7/10). Extraoral and intraoral PBM treatment as described earlier were performed twice weekly. Further, we used the cluster of 69 LEDs to specifically treat her lips (Fig. 2A). Moreover, in addition to deep tissue manipulation by the physiotherapist, her wrists and elbows were illuminated with the extraoral LED cluster probe (described earlier) and a third treatment probe with five 810 nm lasers at 200 mW each, 5.96 W/cm2, pulsed 2.5 Hz, 60 sec, 6 J per laser, and 357.6 J/cm2 each. This treatment regimen was continued for 9 months (with a few short interruptions); her mouth opening increased to 21 mm, her cheeks felt less stiff, and oral sensitivity decreased (VAS 3/10) (Fig. 2B). In addition, swallowing became less difficult and the range of motion of the elbows and wrists improved. As cGVHD appeared to be stable, systemic prednisone 5 × 2.5 mg daily was slowly tapered, but PBM therapy was continued at least once a week. Unfortunately, when the patient was unable to attend PBM visits for a number of weeks due to injuries as a result of a fall, orofacial cGVHD deteriorated again, suggesting that PBM therapy should be continued over extended periods for continued therapeutic benefit.
Discussion
Our prior report showed improvement in oral cGVHD-related symptoms and signs when PBM therapy was added to topical and systemic therapies that were inadequate by themselves, in managing clinical disease. 8 The current report also highlights the additional utility of PBM treatments in the management of secondary complications of tissue fibrosis in oral cGVHD. Our findings further support prior published reports of oral cGVHD mucosal lesions that are effectively managed with PBM therapy. 16 –19 The observations in our current report indicate that PBM therapy is an additional non-invasive adjunctive treatment modality, along with physiotherapy and palliative pharmacological interventions, in the effective management of sclerodermatous changes in oral cGVHD.
The major tissue responses involved in fibrosis are a pronounced extracellular matrix (ECM) synthesis, predominantly collagen that fails to organize into routine (basket-weave) patterns. Fibrotic tissue has prominently increased ECM rather than dramatic changes in cells generating them, the fibroblasts. There is growing evidence that cell lineage switching (epithelial-mesenchymal or mesenchymal-epithelial transitions) may also contribute to these exaggerated ECM elaboration processes. Skin fibroses usually manifests as either Keloids or hypertrophic scars whereas mucosa, surprisingly, usually scars minimally. 20,21 This appears to be a teleological adaptation to counter the significant routine biomechanical injuries to the mucosal surfaces. The non-scarring nature has been attributed to multiple factors that are unique to the mucosal biology, including moist secretions (e.g., saliva in oral cavity), presence of distinctive ECM (but yet to be fully described), and discrete molecular signaling pathways (e.g., increased TGF-β 3:1 ratios). 22,23 However, there are examples of discrete oral conditions that manifest with prominent scarring responses, a classical example being oral submucous fibroses that is common in South-East Asia. 24
Interestingly, a key aspect of the biological response to scarring is the presence of a prominent inflammatory response. 25 –28 This inflammatory reaction appears to provide a conducive cellular and cytokine milieu to promote the scar-promoting autocrine signaling responses. A prominent role for growth factors (TGF-β, PDGF, CTGF, HGF, and VEGF), cytokines (IL-1β, IL-5, IL-6, IL-13, IL-21, IL-4R, IL-13R,GM-CSF, TNF-α, oncostatin M, WISP-1, IFN-γ IFN-α/β, IL-12, IL-10), chemokines (CXCL-1, 2, 12, CCL-2, 3, 6, 17, 18, CXCL-10, 11, CCR-2, 3, 5, 7, CXCR-2, 4), immune modulators (TLR3, TLR4, TLR9), matrix modulators such as enzymes and proteases (MMPs, TIMPs, proxyl hydroxylase, integrins, integrin-linked kinase), cell adhesion modulators (Cadherins, ICAM-1, VCAM-1), and, more recently, regulator RNA (miR-29b, miR-29c, miR-200a, miR-141 and miR-199a) have all been implicated in the scarring process. 24 Besides various effective pharmacological clinical interventions, the most clinically effective treatment for scarring has been the recognition, and mitigation, of biomechanical forces that exacerbate scar phenotypes. 25 –27 Besides providing a fundamental understanding of the scarring process, these molecules offer attractive precision-medicine targeting strategies that can be broadly categorized into three distinct functional groups, namely scar triggers (inflammation), scar modulators (ECM turnover remodeling and angiogenesis), and scar effectors (ECM elaboration). 29 –32
The use of biophotonics in various aspects of clinical dentistry is revolutionizing patient care. 9 The use of various light sources, including lasers, LED, and broad-band light, at low doses has been shown to be effective for PBM therapy. As previously noted, there have been major advances in our understanding of the PBM mechanisms and this has added credence to the plethora of clinical and lab-based studies that have noted treatment efficacy. A major focus of PBM mechanisms has been with the absorption by Cytochrome C Oxidase and induction of ROS, ATP, and nitric oxide. Although this mechanism is clearly central to specific pathophysiological processes, several other PBM-modulated molecular pathways have been identified both inside and outside the cell, including activation of NFκB and TGF-β1. 9 Interestingly, both these molecules have pro-inflammatory and pro-fibrotic functions and their induction by PBM therapy would seem counter-intuitive to their potential therapeutic roles in cGVHD fibroses noted in this article. Nonetheless, the molecular dichotomy of the observed clinical PBM effects has been repeatedly demonstrated. A simple analogy to this observation can be drawn from the current practice of debriding and generating bleeding margins in chronic wounds to restart the healing process. PBM therapy appears to subtly follow a similar restart of the pathophysiological healing processes that we previously termed resychronization. 9 Given the limited, and well described, biological pathways driving various pathophysiological responses, the context in which specific molecules are evoked along with their autocrine regulatory loops likely dictates eventual biological outcome. This also suggests that perhaps there may be potential novel insights into precise biological roles of these pathways evoked by PBM therapy than previously understood with conventional interventions.
The use of PBM therapy in cGVHD would be largely aimed at mitigating the inflammatory components initiating tissue fibroses (Fig. 3). There is significant evidence from laboratory studies that have assessed the anti-inflammatory effects of PBM therapy from a wide range of injuries in the molecular, cell-tissue, and animal model. 33 –38 Hence, as highlighted in this article, the use of PBM therapy was associated with improvement in clinically apparent, prominent mucosal fibroses and associated functional impairment. It should be emphasized that both patients had pharmacological as well as physical therapy in addition to PBM therapy, with the latter being a critical component to most effectively resolve tissue fibrosis. Individual contributions, either synergistic or additive, of these conventional and PBM therapies could be addressed in future controlled clinical studies. Another distinct feature of cGVHD is cutaneous fibrosis. The use of lasers for skin rejuvenation and scar revision is routinely being practiced in dermatology. 39,40 Interestingly, the second patient reported that the range of motion of her elbows and wrists improved significantly with PBM therapy, in addition to physical therapy. The combination of intra- and extraoral PBM treatments in both cases as well as additional skin treatments raise interesting paracrine effects or bystander phenomenon that have been shown to have additional therapeutic benefits. 9 In addition, there may be a role for the use of PBM therapy for the management of fibrosis associated with radiotherapy or after mastectomy.
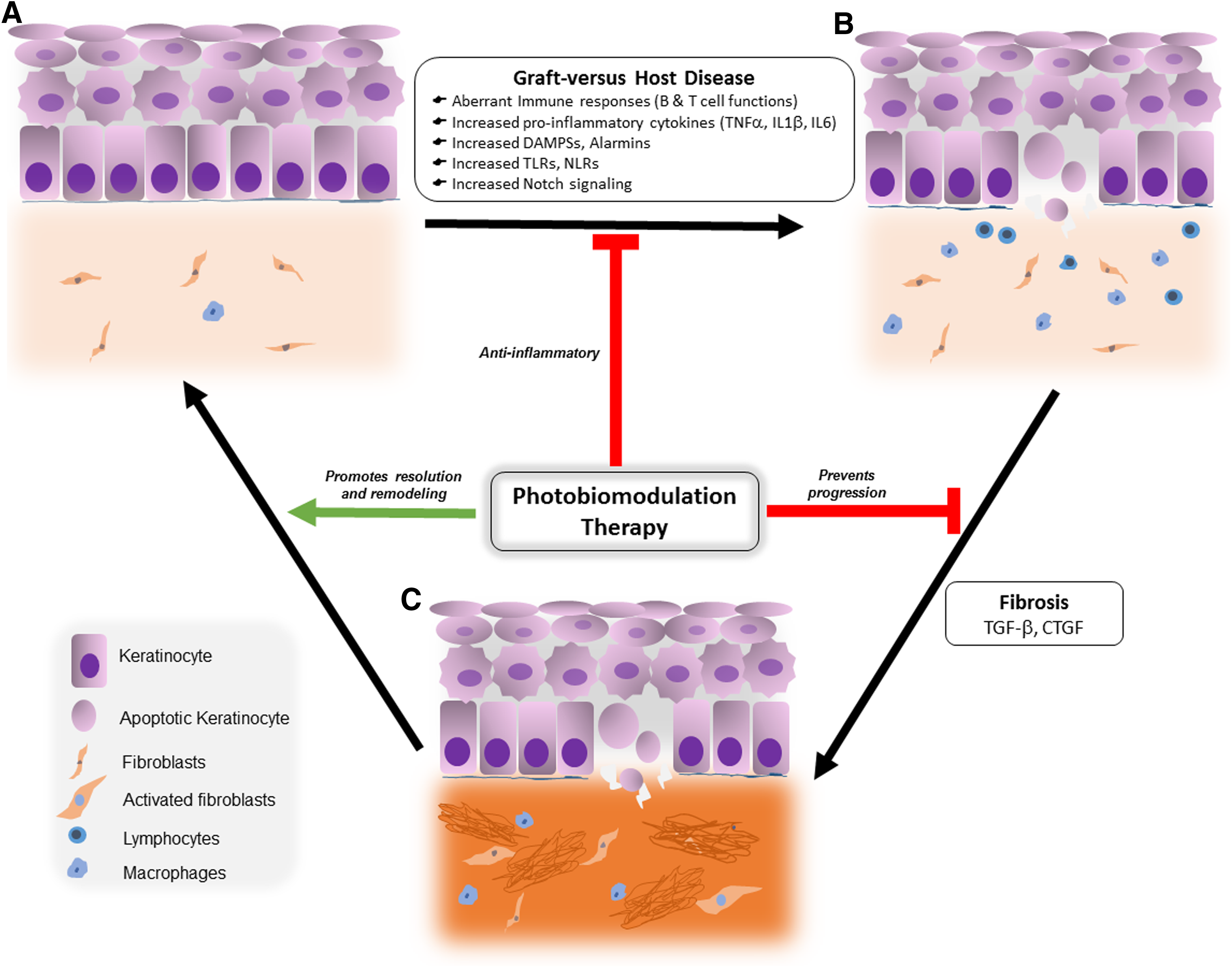
Potential mechanisms of action of PBM therapy in cGVHD.
A major obstacle for more popular PBM clinical use has been a lack of rigorous treatment regimens. This appears to arise from two major reasons: First, the lack of a precise mechanistic rationale for PBM use, namely, what biological process exactly—pain, inflammation, immune response, or healing—is being targeted? Second, a lack of understanding of a specific molecular or cell type such as the fibroblast, endothelial cell, or macrophage driving the fibroses would logically require individualized PBM dosing parameters, as recently noted. 41 In both the cases in this study, a combination of intra- and extraoral treatments with irradiances ranging from 30 to 50 mW/cm2, 2.5 Hz, and 1.8 to 3 J/cm2 for 60 sec were used. Treatments performed daily after patient presentation followed by longer gaps in treatments (repeated either every 2 or 3 weeks) in a sustained manner appeared to be important to get maximal benefit. As evident in Case 1 (Fig. 1E), interruptions in treatment resulted in a relapse of symptoms, including oral ulcers, restricted mouth opening, and pain emphasizing the importance of treatment repetitions and timing. Home-use devices with preset dosing offer an attractive possibility given the multiple, repeat dosing regimens and few such devices are currently available for specific ailments. However, there remains a significant need for future development of these home-care devices that have fixed dosing regimens, unlike current clinical units, to maximize safety and specifically evoke sustained therapeutic biological responses.
The use of lasers for PBM therapy has inherent clinical safety issues of inadvertent exposure, especially to the eye. In addition, GVHD has been identified as a potential risk factor for the development of second primary oral malignancies, and although it is very unlikely that PBM promotes tumor genesis it seems prudent to avoid exposure of (pre)-malignant oral lesions to PBM until more information is available on PBM therapy and tumor behavior. 42,43 There is a known risk of second malignancy, including oral squamous cell carcinoma (SCC), in patients with GVHD. However, it is important to consider the significance of symptomatic chronic GVHD on overall quality of life, including nutrition, oral-dental functions, and social and economic impact in relation to the potential malignancy risks. In addition, PBM therapy seems to reduce oral inflammation as well as the need for using immunosuppressive therapies that may contribute to SCC risk. Moreover, PBM therapy has been extensively used in the management of oral mucositis after oncotherapy and there has been no evidence suggesting a negative impact on incidences of recurrences or secondary malignancies in these patients. Nevertheless, vigilance is indicated and in vivo studies are necessary. Besides the safety issues of using the small spot sizes of lasers, treatments with these devices require longer treatment times to cover all affected areas. These are now being countered by the development of large arrays, often combining LEDs and laser diodes or LEDs alone that are more practical and essentially offer better therapeutic dose windows. A recent study outlined the molecular mechanism mediating laser phototoxicity involving generation of heat and ROS in biological tissue that can be clinically monitored by ensuring PBM surface treatment temperature does not rise more than 45°C. 44 This may provide a convenient real-time monitoring of PBM treatments. In conclusion, the use of PBM therapy represents a non-invasive adjunctive therapy in the management of secondary complications of fibroses from cGVHD. The clinical evidence clearly shows the therapeutic benefit from this treatment warranting more, well-designed future studies to carefully establish the efficacy and clinical safety for PBM therapy in cGVHD.
Footnotes
Acknowledgments
The authors thank Dr. Renée Koppelmans for providing editorial assistance. This work is supported by UB new faculty start-up funds (PRA).
Author Disclosure Statement
No competing financial interests exist.