
Abstract
Introduction
H
The lack of conditions for health assistance to the population and the inadequate cleaning procedures of hospital surfaces accent the dissemination of potentially pathogenic microorganisms, allowing the occurrence of contamination. The possibility of failures in the hygiene of health professionals and processes of material sterilization are factors that contribute to inefficiency of infection control in general healthcare environments. 2 –4
According to ANVISA (National Agency of Health Surveillance) in Brazil, the environmental contamination by bacteria, fungi, and viruses is a substantial safety risk to patients and professionals. The surface decontamination is a primary and obligatory element to assure the security of patients and health professionals. Such procedures act directly in prevention and control of infections, reducing the high levels of microorganisms found in these locations. 5 Thus, constant care in the decontamination of surfaces can improve the overall infectious conditions.
Decontamination of surfaces is performed by contacting the surface with some disinfecting agent. The success of disinfection depends on factors such as the type of microorganisms, concentration of active chemical substances, and the overall duration of the disinfection process. 6 However, in certain cases, hospital surface contamination can recur rapidly after cleaning since the safety against nosocomial infections has not shown satisfactory levels of disinfection. 7 The type of surface can affect the removal of microorganisms as well as retain chemicals that can cause irritations. 8
Some technologies have entered the healthcare market for enhancing the containment of multidrug-resistant microorganisms. Ultraviolet (UV) light is one of the technologies widely used for inactivating bacteria, viruses, and fungi in disinfection of surfaces, air, water, and the food processing industry. 6,9 It can be an alternative for microbial inactivation of hospital surfaces, with security for the operator.
UV irradiation is a fraction of the electromagnetic spectrum, with a wavelength ranging from 200 to 400 nm. UV is subdivided into three distinct spectral areas, including ultraviolet C (UV-C; 200–280 nm), UV-B (280–320 nm), and UV-A (320–400 nm). The antimicrobial effect of UV-C light is caused by its ability to damage the DNA and RNA of microorganisms, causing adjacent thymine bases on the same DNA strand to covalently bond together, forming thymine/thymine dimers. This effect promotes blocking transcription and replication, affecting the functions of the microorganisms, causing their death. 10 –12 UV-C irradiation is, however, mainly responsible for the germicidal effect. The way UV-C acts, there is no chance of resistance developing.
The aim of this study was to evaluate the effectiveness of the Surface UV® device in reducing the counts of Staphylococcus aureus, Streptococcus mutans, Streptococcus pneumoniae, two strains of Escherichia coli, Pseudomonas aeruginosa, Candida albicans, and other clinical microorganisms isolated from different surfaces of a public health hospital. The idea is to add such a procedure to better improve the possibilities of decontamination in public health facilities without the abusive use of chemicals.
Materials and Methods
Study design
Figure 1 illustrates a flowchart with the studies performed.
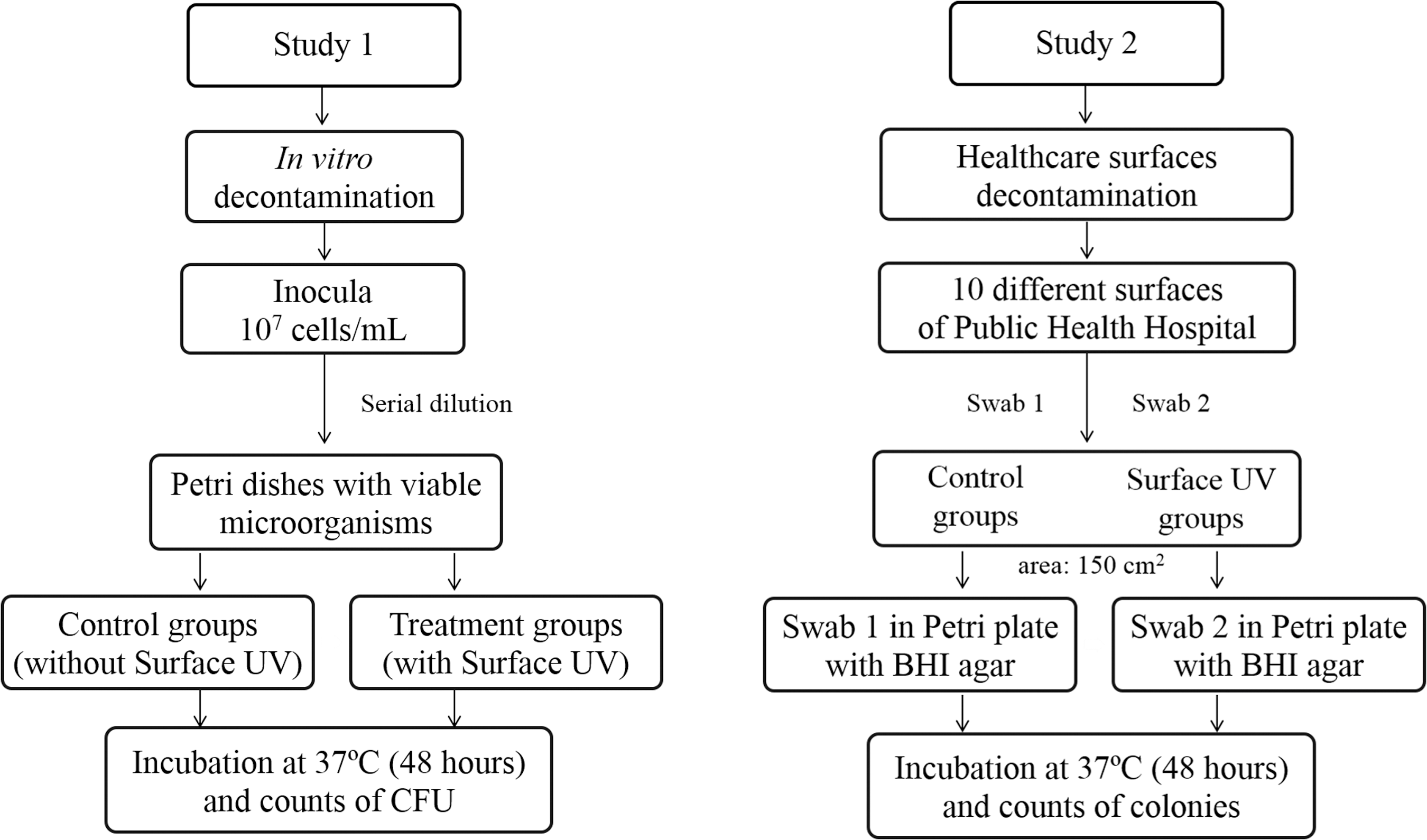
Flowchart of the studies performed.
Device setup and optical characteristics
The Surface UV device (MMOptics, Sao Carlos, Brazil; Fig. 2A) was developed by the laboratory support technician from the Optics Group of the Sao Carlos Institute of Physics (PI Patent: BR 20 2014 006540-2) with the advantage of presenting a configuration base UV-C lamp used for surface disinfection acting in microbiological control.
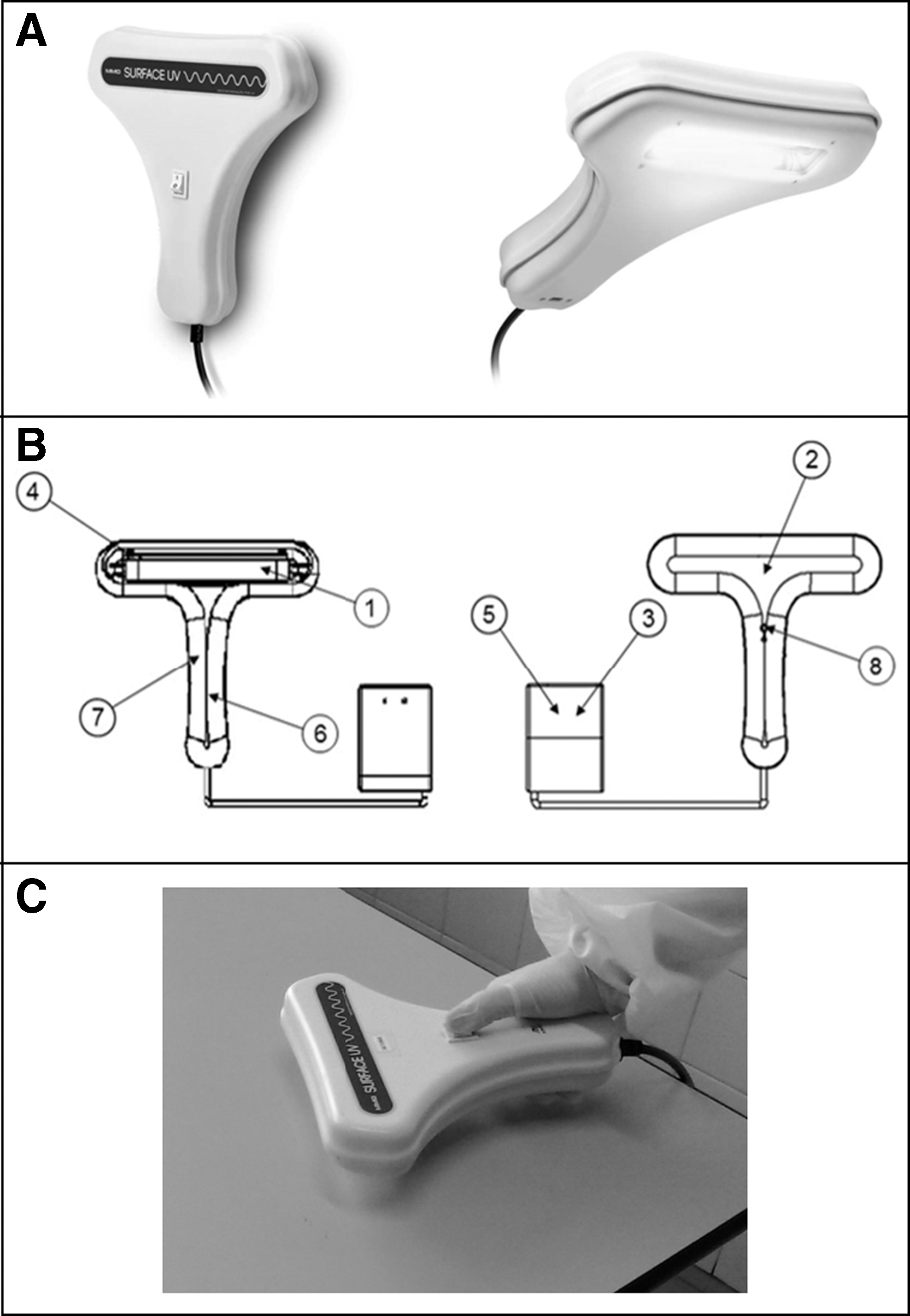
This UV light emits UV-C at 254 nm and produces a total irradiance of 13 mW/cm2 at a distance of 1 cm of the surfaces. It contains a security feature that allows illumination only when the lamp is facing the surfaces, avoiding ocular exposure.
A schematic drawing of the device and its main parts is shown in Fig. 2B. These parts were included to consider the following aspects: susceptibility for surface decontamination of laboratories, hospitals, dental clinics, and specific medical environments. For the safety of the operator there is a mercury sensor attached to the UV-C lamp, with the purpose of protection, that switches off the UV-C light when it is not positioned to the surface.
Study 1: in vitro decontamination using Surface UV (controlled conditions)
Microorganism strains and growth conditions
The microorganisms used for the in vitro decontamination tests were gram-positive bacteria S. aureus (ATCC 25923), S. mutans (ATCC 25175), S. pneumoniae (ATCC 49619), gram-negative bacteria E. coli (ATCC 25922), E. coli (ATCC 8739), P. aeruginosa (ATCC 14502), and the yeast C. albicans (ATCC 90028). These microorganisms were chosen to represent different structural models of cell walls, and because they are used to test the efficiency of antimicrobial agents. The bacteria S. aureus, S. mutans, S. pneumoniae, two strains of E. coli and P. aeruginosa were cultivated in the brain/heart infusion (BHI) broth at 37°C for 24 h and the yeast C. albicans was grown on Sabouraud's dextrose agar at 37°C for 24 h. Afterward, the suspensions were homogenized, centrifuged at 1000g for 15 min, and resuspended in phosphate-buffered saline (PBS). The inoculum suspensions of all microorganisms were quantified through the optical density and adjusted for approximately, 107 cells/mL.
Experimental methodology
In this experimental method, all tests consisted of irradiating the microorganisms spread on Petri dishes with culture medium and quantifying the viable population after irradiation. Before irradiation, the inoculum suspensions were homogenized, and aliquots of 100 μL were transferred into microtubes containing 900 μL of PBS to carry out the serial dilution until 10−5. Aliquots of 25 μL of all dilutions of bacteria were uniformly spread on Petri dishes with BHI agar, and aliquots of 25 μL of all dilutions of C. albicans were homogeneously dispersed to Petri dishes with Sabouraud's dextrose agar. This procedure was performed for the control groups (without Surface UV application) and treatment groups (with Surface UV application). All the treatment groups' plates received the irradiation at a distance of 1 cm for 60 sec and, in this condition, the light dose was 0.78 J/cm2. After that, plates were maintained at 37°C for 48 h to carry out the counts of colony-forming units (CFU).
Data analysis
After the decontamination, the CFU were quantified, and the results were compared to the control group, which did not receive the Surface UV application. Each experimental group was independently tested three times and measured in triplicate, resulting in nine measurements per group. For the purpose of analysis, CFU/mL values were transformed into a base 10 logarithm (log10), and for the statistical analysis, the paired-sample t-test was performed between the control groups (nonirradiated) and their respective irradiated groups. Differences were considered statistically significant at p ≤ 0.05.
Study 2: healthcare environmental surface decontamination (real conditions)
Surfaces chosen for Surface UV application
To perform a proof-of-principle for a practical application of the device under real conditions of microbial inactivation, experiments were performed on different surfaces of Public Health Hospital, located in Araraquara, Brazil. To verify the action of the Surface UV device on surface decontamination of the healthcare environment, healthcare workers such as nurses, nursing aides, and other healthcare providers used the device on surfaces of Public Health Hospital from January until July of 2016.
A total of 10 different surfaces were chosen to receive the treatment as follows: (1) workbench of bacteriology laboratory, (2) blood sampling chair, (3) children's changing table of child healthcare room, (4) doctor's office desk of medical clinic room, (5) doctor's office desk of sexually transmitted diseases room, (6) handle hospital drawer of leprosy room, (7) doctor's office desk of vaccines room, (8) doctor's office desk of dermatology room, (9) gynecology chair of woman's health room, and (10) hospital cafeteria and kitchen. As these places are frequented by numerous people every day and probably have a high contamination, they were chosen for this investigation.
Experimental methodology
The application protocols were the same for all surfaces. To collect samples of 10 different surfaces, an area of ∼150 cm2 was delimited and divided into two sections. Before irradiation, the control samples were collected from one section using a sterile swab. After UV irradiation, the treatment samples were collected from the other section using another sterile swab. The irradiation was performed at a distance of 1 cm from surfaces, in a slowly scanning mode, for 60 sec resulting in a light dose of 0.78 J/cm2 and intensity of 1.3 × 104 μW/cm2. All samples were collected from surfaces with sterilized swabs and passed directly on a Petri plate containing BHI agar. The cultures were maintained at 37°C for 48 h, and then the growth of colonies was analyzed. This experiment was performed in three distinct areas of each surface and on three independent days. An image of the use of the device is shown in Fig. 2C.
Data analysis
After the procedure, the number of colonies recovered from each nonirradiated and irradiated section of surfaces was quantified. Thus, all the colonies that appeared on the plates were counted. As the collections were carried out directly on the surfaces and passed to Petri plates containing BHI agar, it was not possible to standardize the initial microorganism concentrations on each surface. Thus, the results were expressed as a percentage of microbial reduction to evidence the decrease, disregarding the variation of the initial inoculum from surface to surface. The rate of microbial reduction was determined by (N 0 − N/N 0) × 100 (N 0 = number of colonies from the nonirradiated section, N = number of colonies from irradiated section). Each irradiated section was compared with the corresponding control section, which did not receive the Surface UV. All experiments were performed on three different days and measured in triplicate, resulting in nine measurements per group.
Results
The results are divided into two different studies: (1) the microorganism's inactivation in vitro performed in the presence of gram-positive bacteria S. aureus, S. mutans, S. pneumoniae, gram-negative bacteria E. coli (two strains), P. aeruginosa, and yeast C. albicans, and (2) the surface decontamination of healthcare environments with the comparison of nonexposed and exposed contaminated surfaces to the UV light.
The data of study 1 are shown in log (CFU/mL), and the reduction of the microorganisms in vitro after Surface UV application is indicated in Fig. 3. The results indicated a significant log10 reduction factor of 6.5 for S. aureus, 6.7 for S. mutans, 6.2 for S. pneumoniae, 5.4 for E. coli, 5.2 for E. coli (ATCC 8739), 5.4 for P. aeruginosa, and 6.7 for C. albicans.
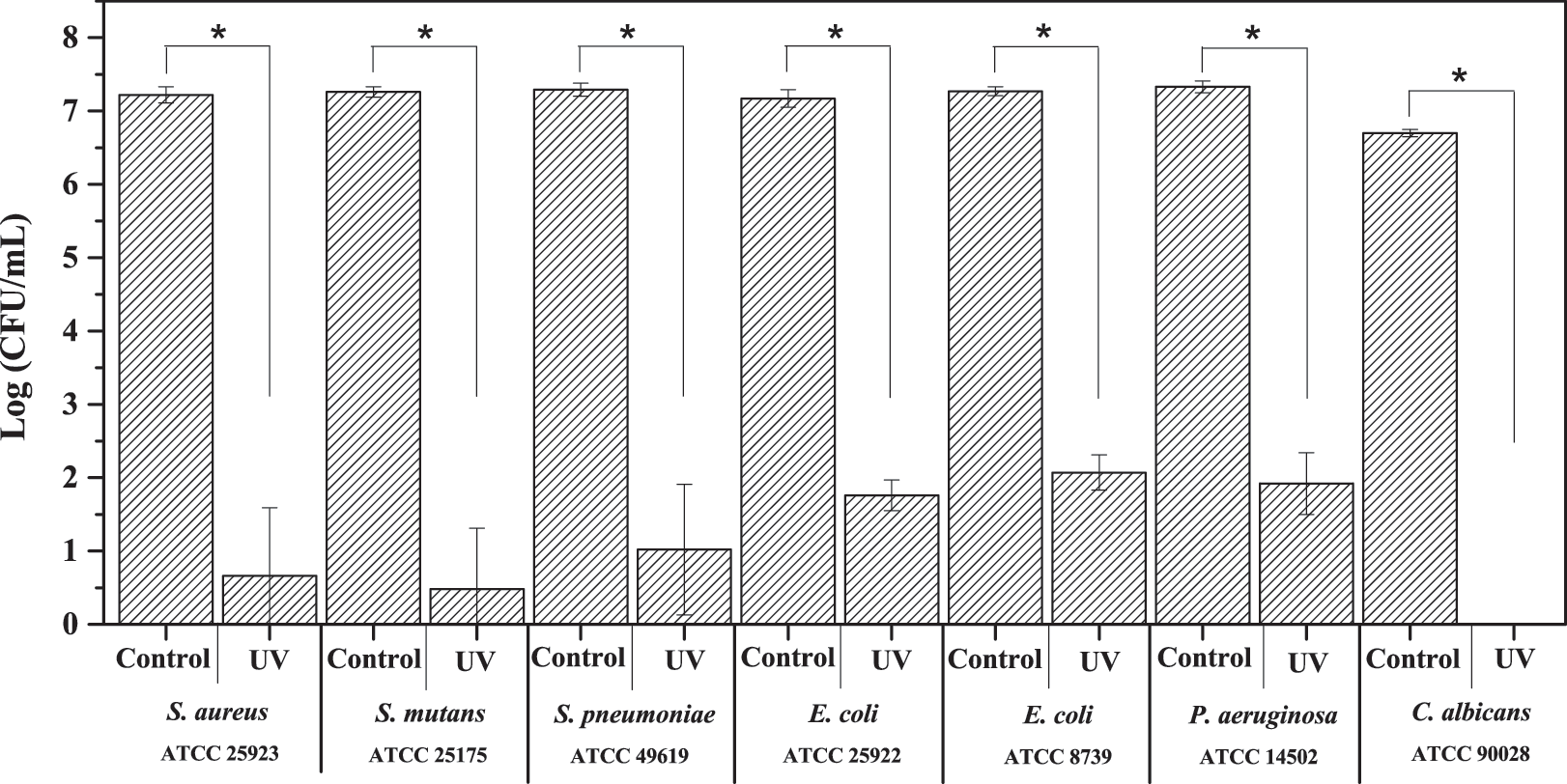
Log10 (CFU/mL) of Staphylococcus aureus (ATCC 25923), Streptococcus mutans (ATCC 25175), Streptococcus pneumoniae (ATCC 49619), Escherichia coli (ATCC 25922), E. coli (ATCC 8739), Pseudomonas aeruginosa (ATCC 14502), and Candida albicans (ATCC 90028) before and after the Surface UV application with 0.78 J/cm2 of light dose and 1.3 × 104 μW/cm2 of intensity. Data are shown as mean and standard deviation for log10 CFU/mL. Statistical significance was defined at *p ≤ 0.05 level. CFU, colony-forming units.
Figure 4 shows the results of study 2 in a box plot graph with the percentage of microbial reduction for each treated surface of Public Health Hospital of Araraquara. A significant reduction of microorganisms level on 10 hospital surfaces was observed when the Surface UV was used in microbial-rich environments.
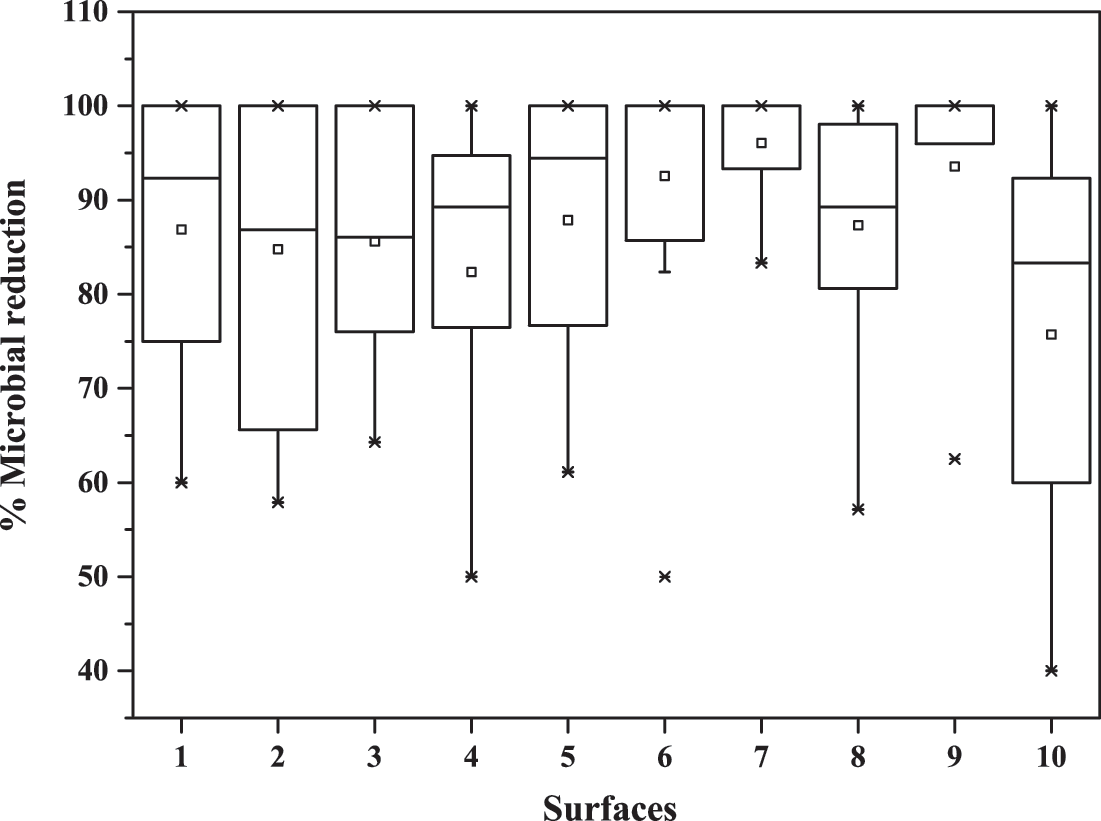
Percentage of microbial reduction after Surface UV application on surfaces of Public Health Hospital of Araraquara: (1) workbench of bacteriology laboratory: 86.9%, (2) blood sampling chair: 84.8%, (3) children's changer table of child healthcare room: 85.6%, (4) doctor's office desk of medical clinic room: 82.3%, (5) doctor's office desk of sexually transmitted diseases room: 87.9%, (6) handle hospital drawer of leprosy room: 92.6%, (7) doctor's office desk of vaccines room: 96.1%, (8) doctor's office desk of dermatology room: 87.3%, (9) gynecology chair of woman's health room: 93.6%, and (10) hospital cafeteria and kitchen: 75.7%. The symbol “□” represents the mean; the symbol “×” represents 99% and 1% of the data; and the upper and lower lines represent the maximum and minimum values, respectively.
Discussion
The results of this study concern the verification of the efficiency of a device developed for surface decontamination using UV-C light.
The presence of pathogenic microorganisms in the hospital environments is mostly related to the huge flow of patients with infections. Air can transport microorganisms through different particle sizes that can carry them in these environments. Moreover, some species of bacteria and fungi can be kept in an ambient environment without the necessary growth conditions (O2, pH, temperature, nutrients, water, osmolality), which also facilitates the occurrence of contaminations. In hospitals, all the surfaces are routinely cleaned and disinfected, according to predetermined cleaning policies of each hospital, or when surfaces appear visibly dirty, and always after patient discharge. The frequency of cleaning and disinfection and the type of substances used for this depend on the clinical risk, patient turnover, the intensity of people traffic in the area, and surface characteristics. 13 In practice, many patients use the same location in between procedures. That increases the risk of infection.
The Surface UV may be used on all surfaces of health services, which can be vehicles of microorganisms in hospital infections: furniture, countertops, sinks, beds, equipment, supports, balance, floors, wall partitions, doors, windows, air conditioning, and computers, among others. All of these surfaces may be involved in the epidemiological chain of hospital infections for being reservoirs for many microorganisms that can be transmitted to patients through hand contamination of professionals, equipment, objects, and any contaminated material. In an important review, Dai et al. presented the potential of UV-C irradiation as an alternative approach to current methods, 14 especially in vitro and clinical studies.
For study 1, the decontamination procedure of microorganisms showed an efficient reduction of all microorganisms studied, indicating that Surface UV is a possible method to be applied to surfaces provided its application could be performed in conjunction with standard hospital disinfection procedures. It is known that in the inactivation of microorganisms, the effectiveness of UV-C light depends on intensity and radiation time due to the complexity of each microorganism. A 60-sec irradiation was used and this irradiation time was satisfactory to a log10 reduction factor of 6 for gram-positive bacteria and fungi, and 5 for gram-negative bacteria. The choice of this light dose was based on studies already described in the literature 12 to ensure an efficient microbial reduction, in addition to ensuring the practicality of this device application for a short exposure time. This efficient result in short exposure time indicates the possibility for use with success to assist in the decontamination in real spots.
The results of study 2, the surface decontamination of Public Health Hospital of Araraquara, differed by structure and design of furniture surface, chosen due to their increased use in the hospital rooms. The material and design of surface may influence the behavior of light incident on the surface. In addition, the structure of furniture can also change the adhesion of microorganisms and form resistant biofilms to sterilization processes, making it difficult in certain cases in the decontamination process.
The decontaminated surfaces were composed of these materials, respectively: (1) granite, (2) leatherette, (3) formica, (4) medium-density fiberboard (MDF), (5) glass on wood, (6) painted iron, (7) MDF, (8) MDF, (9) plastic, and (10) wood with plastic towel. In all of them, the procedure of decontamination showed a microorganism reduction above 75%. Even though this is an encouraging result, it is still necessary to improve the protocols and the radiance time to provide total eradication of microorganisms on surfaces of healthcare environments. It is predicted that doubling exposure time will promote 3–4 log decay. While the in vitro experiments were contaminated with planktonic form of microorganisms, the real surfaces were probably contaminated with biofilms, naturally demanding more irradiation to an efficient reduction.
The probable reason for high standard deviations in these results comes from the variability of the samples. Each collect was done on three different days, and the microorganism quantity may change from one day to another. Moreover, the transient microbiota also changes due to the flow of people in this environment. Whereas the current disinfection methods can exhibit viability failures, high cost, and toxicity, the use of this device in hospital routine may help positively in controlling contamination. Besides that, the Surface UV can also be considered a green and highly sustainable technology; it brings environmental benefits by reducing the use of chemicals, which have high costs to public health systems and toxicity risk to the population.
Since is necessary to avoid the use of mercury lamps due to environmental consequences, the second prototype version of this device will be developed using a 262 nm light-emitting diode system, which will also reduce the size and cost of a future device.
Conclusions
This study showed the importance of developing this device as a light source for assisting in surface decontamination, improving infection control of healthcare environments by UV-C light. The Surface UV has shown promise in reducing surface contamination of laboratories and healthcare environments with good results, showing microbial reductions in different situations. Thus, its use may help to disinfect surfaces easily, quickly, effectively, and safely. However, the results presented in this study were achieved with just 60 sec of use of equipment. Therefore, it is possible to improve the decontamination procedure by increasing radiance time, which would increase the level of inactivated microorganisms. Preliminary studies have shown a significant increase with increased time of exposure.
The important conclusion remains the fact that simple and environmentally friendly devices can be used for improving the contaminated areas that receive a large flux of patients. This device and technique are also undergoing tests in two intensive therapy units for implementation in hospitals to assist the decontamination protocols that already exist in these environments.
Footnotes
Acknowledgments
The authors acknowledge the financial support of FAPESP and the company MMOptics for providing the device. This work was supported by FAPESP (CEPID/CEPOF No. 13/07276-1). T.Q.C. was supported by CAPES fellowship.
Author Disclosure Statement
No competing financial interests exist.