
Abstract
Introduction
D
In the context of tissue repair, this may be benefited when the main biological events that enable it are stimulated, that is, nutrition, cell proliferation, and control of inflammation and infection. 4 –6
Therapy involving the use of low-power laser has attracted many researchers' attention, mainly, its use in photodynamic therapy (PDT). This therapy involves the irradiation of cells/bacteria by light of specific wavelength, and in the presence of a photosensitizing drug, which generates reactive oxygen species when it absorbs the incident radiation. PDT has presented promising and effective outcomes in promoting bacterial death and skin wound treatment. 7,8
PDT has been a therapeutic alternative to accelerate the tissue repair of cutaneous wounds, and several clinical researches proved its benefits. 2,8 –12 This therapy may favor the repair process by promoting photobiomodulation in the tissue to be irradiated and reducing local inflammation, since laser therapy increases mitochondrial activity and ATP synthase, induces cell proliferation, and increases the production of nucleic acids and collagen synthesis. 13 Besides the cicatricial effect, the PDT presents antimicrobial effect. 7,8,14
Hamblin et al. 15 verified that PDT reduced the healing time of wounds performed on the dorsum of mice and infected with Pseudomonas aeruginosa. A 90% reduction in the total amount of bacteria in the wound was observed when compared with the group treated only with Methylene Blue or with the group treated only with laser.
The combined effect of the photosensitizer and laser radiation results in an antimicrobial and biomodulator effect of the tissue environment that enhances the tissue repair process. 16
Several studies have shown PDT-positive effects on wound healing, where a reduction in total healing time has been observed as a result of the decrease in the time of the inflammation stage, formation of early granulation tissue, and acceleration of reepithelialization. 16 –19
The need for the development of therapeutic protocols that accelerate the healing promotes a series of studies with the aim of providing quality in the cicatricial process and minimizing the time of resolution of the tissue lesion. The use of reliable and practical methods to describe wound healing, quantify wound size, compare the same lesion at various times in the repair process, and document the evolution of the lesion is indispensable in the therapeutic practices used to stimulate wound healing. 20 –22
According to Goldman and Salcido, 20 the measurement of the wound can occur through the dimensional evaluation of the lesion, where the measurement of the nominal area is calculated in square centimeters (cm2), multiplying two perpendicular dimensions. Although imprecise, especially in the case of imperfectly shaped wounds or cavities, this method provides a basis for an objective assessment of wound healing. 23
The method of measuring images by computer programs has gained a growing prominence in laboratory and clinical research; in this method, which is defined as digital morphometry, a camera is positioned at a fixed distance from the wound to capture the images. Later, the images are analyzed in an image measurement program that allows the initial measurement to be obtained and can be compared with the other measurements during the cicatrization to determine the evolution of the tissue repair process. 24 Moreover, this method of measurement generates less discomfort for the patient, since it is not necessary to touch the lesion, unlike the method in which the ruler or the caliper touches the wound for measurement. 25
The appropriate and periodic assessment of wound size is essential to document the evolution of the healing process more faithfully and to demonstrate the outcomes of the proposed treatment or the need to re-evaluate the proposed therapy. 20,26
In this context, it was proposed in the present study to perform a macroscopic morphometry evaluation of the diabetic ulcers lesion area in humans treated with PDT, comparing two methods of wound size measurement: nominal area and digital morphometry.
Materials and Methods
The study protocol was approved by the Research Ethics Committee of the Universidade Camilo Castelo Branco and registered in the Plataforma Brasil for clinical trials under the code CAAE: 43253315.0.0000.5494. The study was carried out after approval by the committee and the subsequent reading, acceptance, and signing of the Informed Consent Term by all patients.
A clinical study was conducted, by convenience sample, experimental, and controlled, and composed of 12 patients of both sexes with diabetic ulcers in lower limbs. Patients were evaluated by endocrinologists and vascular surgeons, and satisfying the inclusion criteria, they were allocated according to the order of arrival in each experimental group.
The patients were divided by convenience into two groups, group A (control)—conventional treatment: composed of six patients who had lesion and/or lesions in the lower limbs and who used collagenase/chloramphenicol medication during the whole experimental period, and group B (PDT)—treatment with PDT: composed of six patients who had lesion and/or lesions of lower limbs and who underwent conventional drug treatment (collagenase/chloramphenicol) and were also submitted to PDT with Methylene Blue dye 0.01%, (Imbralab–Química e Farmacêutica Ltda, Azlabor Co, Ribeirão Preto, Brazil) associated with low-power laser therapy in 660 nm
The inclusion criteria were: clinical diagnosis of diabetes mellitus, at least 1 year ago, with clinical follow-up, both sexes were accepted, presenting at least one neuropathic/vascular leg/right and/or left and/or both limbs and leg ulcer; with ability to understand the given instructions and sign the Free and Informed Consent Form.
Patients without any of these conditions were excluded from the study: patients with diabetes mellitus who did not complete the proposed treatment and assessment sessions, who refused the treatment, and who were performing other treatment than the topical use of collagenase/chloramphenicol, such as oral or parenteral corticosteroids, immunosuppressive agents, or cytotoxic agents.
All patients, from both sample groups, received conventional daily treatment with collagenase/chloramphenicol ointment (collagenase 0.6 U/g + chloramphenicol 0.01 g/g, Pomada Dermatológica; Cristália—Produtos Químicos Farmacêuticos Ltda, Itapira, Brazil). Patients were advised to wash their ulcers with water and mild soap in their homes and then dry them with sterile gauze. The ointment was applied evenly over the full extent of the lesion, once a day, throughout the experimental period.
The topical application of the photosensitizing drug was done by means of a dropper, along the entire border and in the central portion of the lesions, and 5 min was expected for the application of the low-power laser.
The low-power laser irradiation was done through the contact technique, where the laser applicator pen was held perpendicular to the skin, at points around the border of the lesion and inside the lesion area. Parameters of the employed red laser at 660 nm wavelength were: 30 mW of power, laser beam area of 0.04 cm2, irradiation time of 8 sec, and a dose of 6 J/cm2 per point (Laserpulse IBRAMED, Amparo, Brazil). The external application was made by the point technique keeping a distance of 1.0 cm from one point to another around the lesion and 0.5 cm from the edge of the lesion; these distances were demarcated by a dermatographic pen. The internal application was done by the technique of scanning per points, keeping 1.0 cm apart from one point to the other, inside the lesion, so that any part of the ulcer was irradiated. To treat the inside of the ulcer the applicator pen was wrapped with plastic film to prevent contamination of the lesion.
Group B received PDT three times a week, on interspersed days (Monday, Wednesday and Friday), over a period of 22 days, totaling a number of 10 sessions. The entire experimental procedure was performed in the same period of the circadian cycle, to avoid variations in data collection. Asepsis of the wounds was performed with direct jets of 0.9% sodium chloride (saline solution) and dried with sterile gauze for the PDT application.
The evolution of the ulcers was evaluated weekly by measuring the length and width of the ulcers, in the first session of each week (1st, 8th, 15th days) and in the last session (22nd day). Each wound was also photographed and its area measured in the sessions already mentioned. Images were taken by standard distance of 30 cm from the lesion area, with the digital photographic camera Sony® Cyber-shot 14.1 Mps (Sony Co, Tokyo, Japan) fixed to a portable tripod.
Area size analysis
For the evaluation of the nominal area of the wound, a millimeter ruler was used and the wound was measured in its greatest length and width; then, multiplying one measure by the other, the area in cm2 was obtained. For the statistical analysis, only the measurements taken in the first session (1st day) and in the last session (22nd day) were considered.
The areas of the photographed ulcers were measured weekly using ImageJ software (U.S. National Institutes of Health, Bethesda, MD). For this analysis, each ulcer edge was manually delimited with the mouse, using the ImageJ software feature, and the entire lesion was circled to calculate the area. The computerized area of the lesion was then determined by using the scale of the ruler photographed with each ulcer. All evaluation using ImageJ software was performed by the same examiner who was not aware of the identification of the samples being analyzed.
Ulcers were evaluated at the beginning, middle, and end of treatment by digital camera, to obtain the repair evolution of the lesions. Through ImageJ software was quantified: the ulcer total areas and the Ulcer Healing Index (UHI). This last index is defined as UHI = (Initial area − Final area/Initial area), where: UHI = 1 represents total reepithelialization; UHI = 0 no sign of reepithelialization; UHI >0 reduction and UHI <0 increase of ulcer area.
Statistical analysis
The t-test for paired samples or the Wilcoxon test (when the variances were significantly different) was used to observe significant difference between patients from the same sample group (control or PDT) comparing before and after the treatment application.
The Mann–Whitney test was applied to observe the existence of significant difference between the two methods of measurement: the UHI and the reduction of the nominal area of the wounds.
The statistical test was applied with significance level of 5% (p < 0.05). The software used was Minitab 17® (Minitab, Inc., State College, PA).
Results
Clinical evaluation of the patients
Information about the clinical conditions of the patients are presented in Table 1, such as gender, age, smoking habit, time of the ulcer, type of affection, history of amputation, and previous/current treatment of the ulcer and diabetes. It can be observed from Table 1 that the two patient groups together comprise seven females and five males, with an average age of 70 years. The time in which patients had the ulcer spanned over a large range from a minimum of 1 month up to a maximum of 19 years. Patients' diabetes was treated with either injectable insulin or oral hypoglycemic drugs. Different ointments have been used to treat patients' ulcers previously, but, after the initiation of the study, only the collagenase/chloramphenicol ointment was applied to all patients.
Fibrase® (fibrinolysin, deoxyribonuclease, chloramphenicol; Pfizer SA, São Paulo, Brazil).
Aquacel Ag Extra® (Convenac; Curativos SA, São Paulo, Brazil).
PDT, photodynamic therapy.
Macroscopic clinical aspects
Figure 1 displays the initial and final clinical evolution of ulcers of control group and group treated with PDT. Photographs were chosen from only two patients of each group to document the differences between the two treatments: collagenase/chloramphenicol alone and collagenase/chloramphenicol combined with PDT, with regard to the clinical aspect and size of the ulcer.
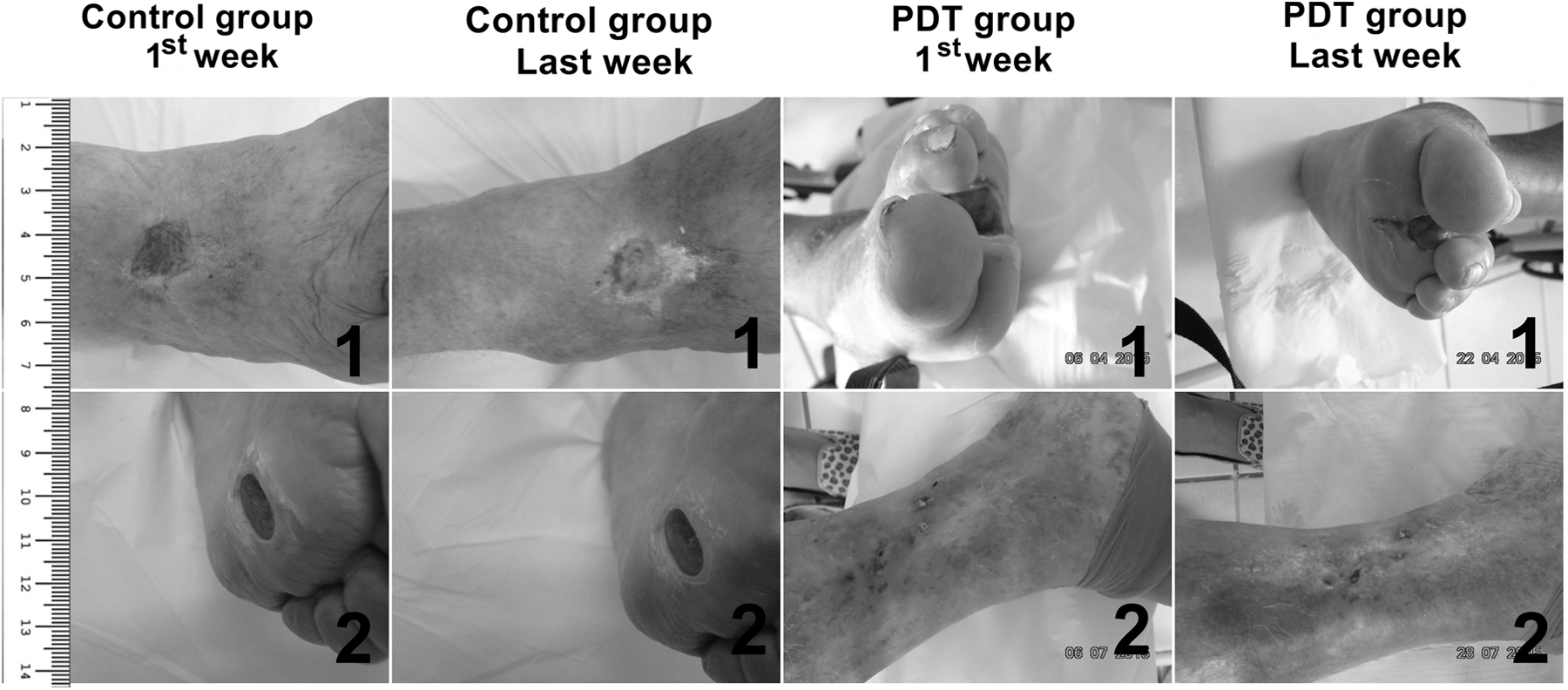
Photographs showing the initial and final aspects of the clinical evolution of ulcers. Control group: 1 (UHI = 0.06) and 2 (UHI = 0.03); PDT group: 1 (UHI = 0.55) and 2 (UHI = 0.61).
The clinical evolution of ulcers was followed during the experimental period, where an improvement is observed of tissue repair in patients treated with PDT, mainly about the macroscopic aspects of neovascularization, epithelialization, and reduction in the area of the lesions; these observations have occurred most notably in patients 1, 4, 5, and 6 of the PDT group.
Comparative analysis of wound area sizes
Table 2 presents a comparative analysis of wound size determined by variables nominal area (cm2) and wound area by ImageJ (cm2), in relation to the control and PDT groups, and according to the accomplishment of the treatment (before and after).
p Value for the Wilcoxon test at p < 0.05.
The results of Table 2 evidence the presence of a significant difference in the comparison of the nominal size of the wounds of patients submitted to PDT when compared with pre- and post-treatment (p = 0.036), and in the area of wounds by ImageJ (p = 0.036) for both groups, control and PDT groups. It is possible to observe by means of the wound size that the PDT promotes a decrease in the nominal size of the wounds of the PDT group (p = 0.036), which could not be observed in the control group (p = 0.10). In addition, PDT also has a positive effect on the area of wounds determined by ImageJ, that is, there is a significant decrease in the area of wounds when compared before and after PDT. Moreover, the area of the wounds by the ImageJ of the control group also presents a significant decrease (p = 0.036), evidencing that the control treatment also has a positive effect on the reduction of the wound area by ImageJ.
UHI and wound area reduction analysis
Table 3 shows the wound area outcomes for all patients evaluated in the study. The initial area Ia and final Fa were calculated by the ImageJ, in the first and last weeks for both groups. Afterward, the patient's UHI was calculated. UHI = 1 is considered as indicative of total wound closure.
PDT, photodynamic therapy; UHI, Ulcer Healing Index.
Table 4 shows the results of the nominal wound area of all patients evaluated in the study (control and PDT groups), and the percentage of the wound reduction.
PDT, photodynamic therapy.
Table 5 presents the descriptive statistics of the two wound area reduction parameters: (a) the UHI, calculated by the values of the initial and final area measurements of all the patients (control and treated), obtained by ImageJ software, and (b) the reduction percentage of the nominal area of the wounds, calculated from the width and length measurements of each lesion, at the beginning and at the end of the treatment of the control and PDT groups.
p Value for the Mann–Whitney test at p < 0.05.
PDT, photodynamic therapy; UHI, Ulcer Healing Index.
The results presented in Table 5 show that both the UHI and the nominal area reduction lead to the same outcome, namely that the PDT accelerates the closure of diabetic wounds
Discussion
Various techniques are used to measure wounds in the clinical area, from the simplest to the most complex. The suitability of the different methods of wound measurement may differ according to the clinical context and the available material and institutional resources. 21
Clinical evaluation and macroscopic measurement of cutaneous wounds are the most common methods for healing studies. The macroscopic morphometric evaluation aims to establish a comparative parameter between the first measurement and the other measurements obtained during the evolution of the cicatricial process. 24
Clinical studies show different ways of evaluating and quantifying the evolution of tissue repair, such as through the UHI, which allows demonstrating efficacy and comparing different treatments, normalizing the different sizes of ulcers. In addition, the use of quantitative methods to measure the area, in short treatment times, prevents the use of ineffective therapy over a long period of time in chronic ulcers and the need for additional treatments. 27
According to Flanagan 26 and Gilman, 28 the percentage of reduction of the wound area is an important indicator to distinguish wounds that will have a good prognosis of cicatricial evolution throughout the treatment. An area reduction of less than 20–40% in the first 2–3 weeks of treatment is an indicator that the wound is not responding adequately to the proposed therapy.
For the assessment of the nominal area of the wound the measurement was made with the aid of a ruler, measuring it in its greater length and width. This technique is considered easy to perform, low cost, and provides an estimative of the lesion size. However, according to some studies, this method of wound measurement, although very frequent in the clinical routine, is very subjective and is considered a more basic form of evaluation, in relation to scientific rigor. 29 –31
The clinical–photographic evaluation of the ulcers and the quantification of the superficial areas were also carried out using ImageJ software, and the UHI evaluation form. The ImageJ software is an important method of quantitative analysis of the evolution of cutaneous ulcers, which allows the demonstration and quantification of the dynamic evolution of wound healing. 2,32
The initial (first week) and final (last week) areas were calculated by ImageJ software, in the control group and in the PDT group, and determined the UHI of each patient. Data revealed a statistically significant difference when we compare the values of the patients of the control group and PDT (p < 0.05). This outcome provides the information that the reduction of the wound area was significantly higher in the wounds of the group treated with PDT, evidencing the efficacy of treatment for wound healing proposed in the present study.
The nominal wound area was also calculated in all patients evaluated in the study (control group and PDT group), as well as the percentage of wound reduction. When comparing the sample groups, there were statistical differences in the percentage of wound reduction of the nominal area of patients in the PDT group, suggesting that this therapy had positive effects on the acceleration and reduction of the lesion area of pati
In the work of Minatel et al., 2 the authors evaluated the efficacy of phototherapy (LEDs 660/890 nm) in the treatment of leg ulcers in diabetic patients at a dose of 3 J/cm2, 30 sec, two times a week, followed by daily dressing with silver sulfate at 1% for 12 weeks, and it was observed that the proposed therapy promoted tissue repair, leading to reduction of lesion area, when analyzed by ImageJ software. Carneiro, 33 in murine model, reported a reduction in the wound perimeter of animals treated with PDT (660 nm laser, dose 120 J/cm2, 100 mW, and Methylene Blue) and that the reduction was more pronounced on the 14th day postinjury in the group treated with low-power laser. Data from Minatel et al. 2 and Carneiro 33 are both in agreement with the present study
On the contrary, data from the work of Sperandio et al. 8 do not agree with results from the present study, since they did not observe significant statistical differences in the areas when comparing wounds treated with PDT, control wounds, and treated with Methylene Blue dye alone, suggesting that PDT did not produce a faster closure of the evaluated lesions. However, it should be considered that the therapeutic protocol in that study consisted of a single application of PDT, which may be considered insufficient to accelerate the closure of the lesions.
Nominal and ImageJ mean size area analyses: when comparing the variable nominal area in relation to the control and PDT groups, and pre- and post-treatment, it was observed that there was a statistical difference in the comparison of the nominal size of the wounds of PDT group when compared before and after the treatment (p = 0.036). On the contrary, for the control group when comparing pre and post-treatment, a reduction in ulcer area was found that was not statistically significant (p = 0.10) because of the large data dispersion. Moreover, the comparison of the area of wounds by ImageJ with respect to control and PDT groups, and before and after treatment, shows that there is statistical difference between pre and post-treatment for both patient groups (p = 0.36)
The area of wounds, calculated by ImageJ in the control group, also shows a significant decrease over time (p < 0.05), revealing that the treatment of the control group with the collagenase/chloramphenicol ointment also has a positive effect in reducing the area of wounds; however, this effect is less than when the collagenase/chloramphenicol is combined with PDT.
Furthermore, the present study also shows to doctors, nurses, and health team treating patients with diabetic ulcers in hospitals, clinics, and infirmaries that there is more than one reliable method to evaluate the evolution of the wound area size, the choice of which to use, depending on the resources of hospitals and clinics. Two methods were tested in this study: the nominal method of measurement and the ImageJ software. The first is easier and low cost, but it is very time consuming, requiring a great effort of the health staff; whereas the second is more expensive, but could be faster when using a computer system
Conclusions
It can be concluded from data that the treatment with PDT speeds up the closing of diabetic ulcers, confirming the hypothesis of the study. Also, data suggest that either one of the two studied methods can be used to evaluate the morphology of the areas of diabetic ulcers in the follow-up of tissue repair process in a reliable way.
Footnotes
Acknowledgments
P.M.C. acknowledges Brazil University for the financial support during the entire accomplishment of this work.
Author Disclosure Statement
No competing financial interests exist.