
Abstract
Introduction
Cancer
I
A series of molecular events that primarily alter the normal properties of cells result in cancer formation. In cancer cells the signaling system that controls and prevents the overgrowth and invasion of neighboring tissues is inactivated. 3 Thus cancer cells with altered regulatory systems grow in the absence of distinct signals that induce normal division and cell growth and so are able to metastasize and invade other tissues. 3
Treatment of Cancer
Conventional cancer treatments
At present there are a large number of cancer treatments available, including chemotherapy, radiotherapy, surgery, monoclonal antibody therapy, immunotherapy, and/or various combinations of these approaches. The choice of therapy is principally based on the type and stage of the disease, as well as the overall health condition of the patient. 4,5
The main problem in using most conventional cancer therapies such as anticancer drugs (chemotherapy) and radiation is their low selectivity for cancer cells, coupled with their often high toxicity to nontargeted cells in the body. 6,7 This most often causes severe side effects which can be more unbearable than the disease at that set moment in time. 6,7 In contrast to radiation therapy and chemotherapy as cancer treatment, an unconventional method known as photodynamic therapy (PDT) was developed. 8
Unconventional cancer treatments
PDT is an alternative method for the treatment of a variety of diseases that require the eradication of pathological cells (i.e., cancer, infectious microorganisms, and other diseases). 8 It involves the administration of photosensitizer (PS) to targeted pathological cells and the localization of light at an appropriate wavelength to excite the PS. 8 This causes the production of cytotoxic reactive oxygen species (ROS), such as singlet molecular oxygen, hydroxyl radicals, and/or superoxide anions, which achieve photocytotoxicity through oxidatively stressing pathological cells, as well as causing damage to their cellular macromolecules such as lipids, proteins, or nucleic acids. 9 –11 The photodynamic activity of PSs is based on photooxidative reactions, which induce multiple consecutive biochemical and morphological reactions. 12 PDT has been applied to a variety of tissues that are accessible to light exposure, including the skin, retina, bronchial tree, and the majority of the gastrointestinal tract for the treatment of cancer cells. 11
Photodynamic Therapy
Principle stages of PDT
Photosensitized PDT reactions in targeted cancer cells involve oxygen and a PS that has been excited by a light source, which generates cytotoxic damage. 13 After the absorption of photons the PS is transformed from its ground state to its triplet excited state through a short-lived singlet state. 9 There are two mechanisms by which a PS can induce cell damage during PDT applications (Fig. 1) as follows 8 :
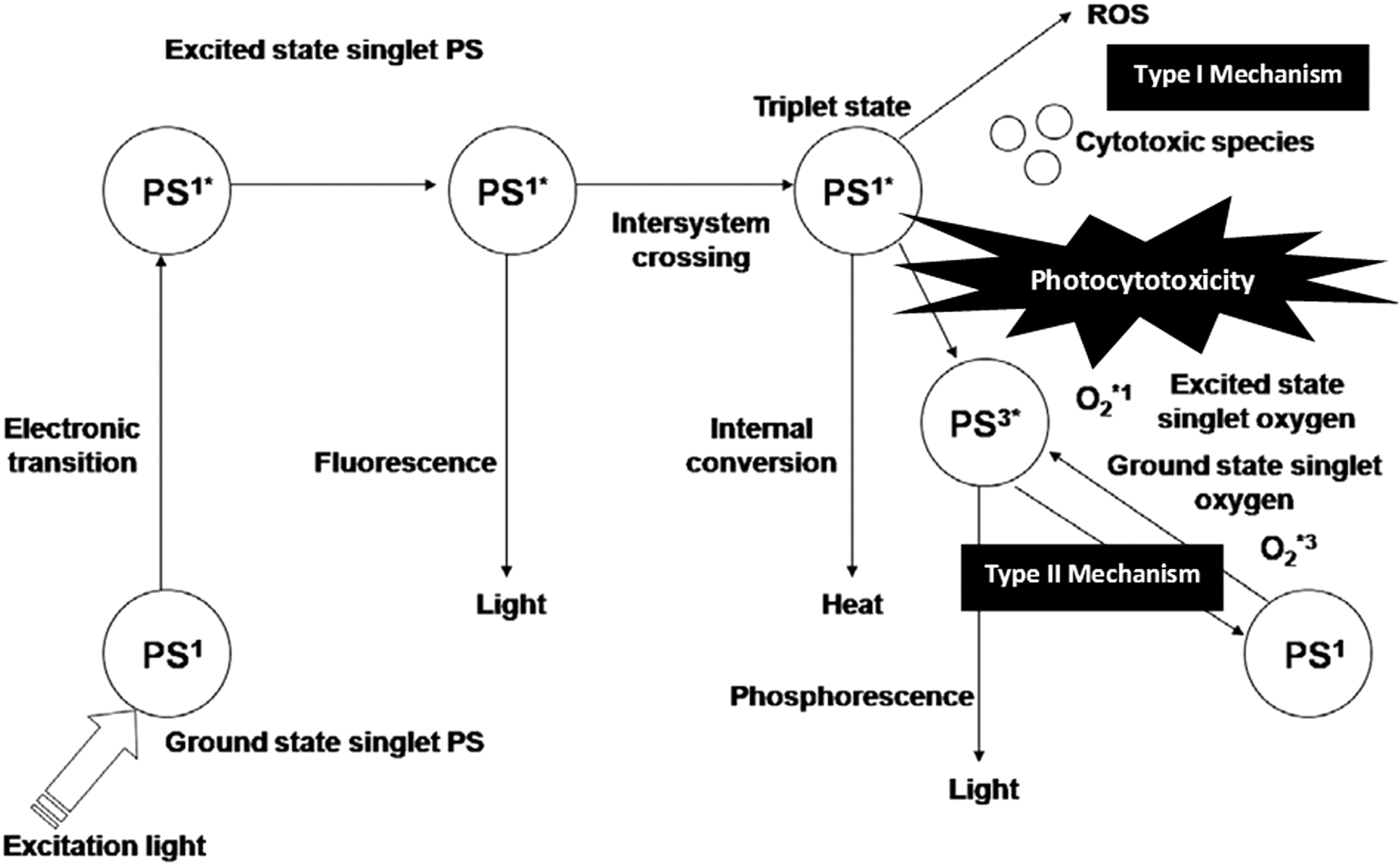
The photophysical and photochemical mechanisms of photodynamic therapy photosensitizer ROS generation. 8 ROS, reactive oxygen species.
1. In type 1 mechanisms the PS in its triplet state reacts with macromolecules and so undergoes electron or hydrogen atom transfer reactions with oxygen leading to the production of ROS and macromolecule degradation, which is cytotoxic to the cell. 9,13
2. In type 2 mechanisms the PS in its triplet state reacts with oxygen in its triplet ground state, which forms cytotoxic singlet oxygen inducing cellular damage. 9,13
3. Transfers its energy directly to ground state triplet oxygen to form both oxygen species in the singlet state and excited state, which are both potent oxidizing agents. 9,13
Mechanisms of PDT facilitated cytotoxicity
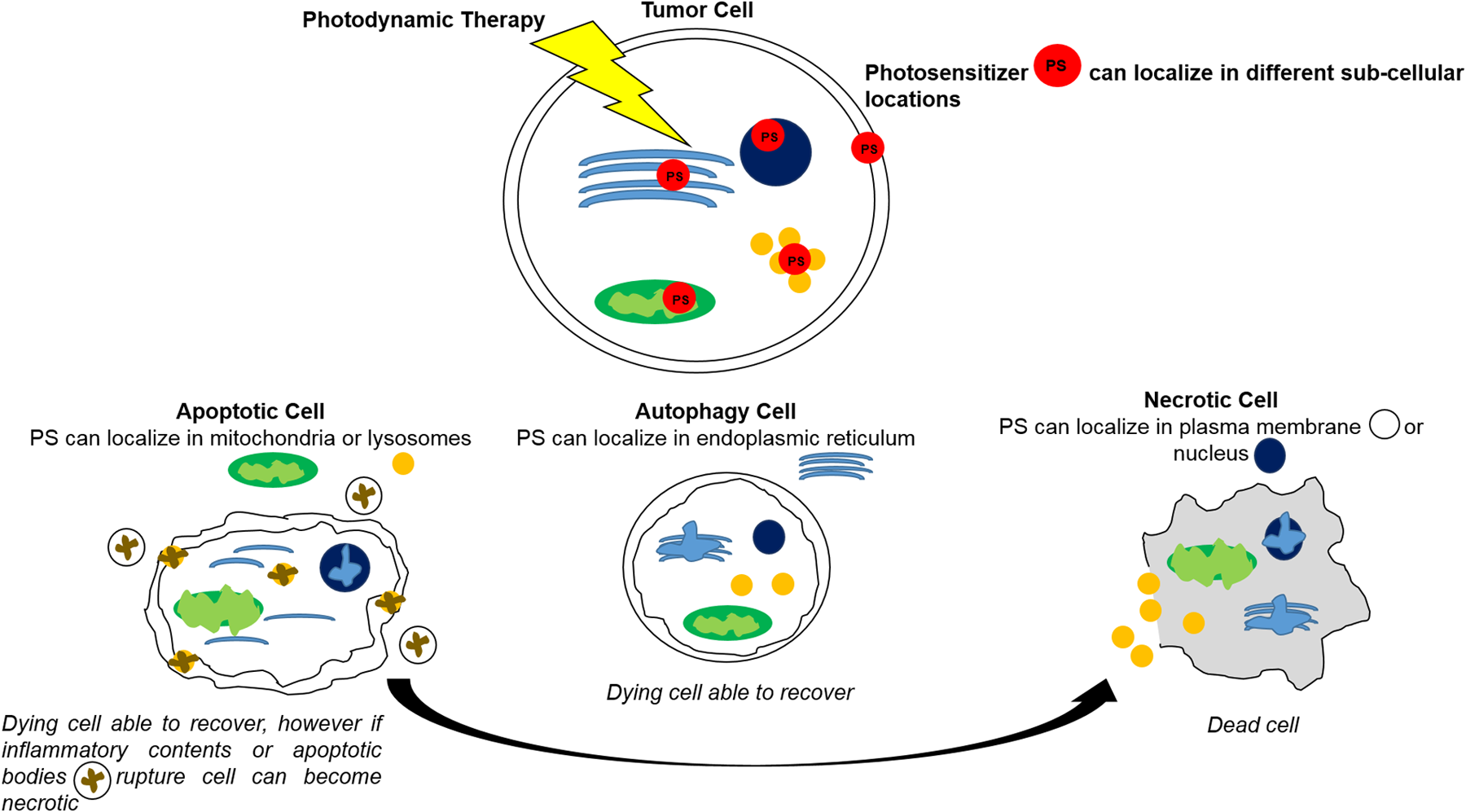
Literature suggests that there is evidently no single pathway that leads to cell death after PDT. 13 PDT induces cancer cell damage by three main cell death pathways, namely apoptosis, necrosis, or autophagy, 2,8 –10 and these mechanisms can occur singularly or simultaneously (Fig. 2). 14
Apoptosis
Apoptosis is the most common cell death modality when cells respond to PDT. 14 PDT destroys cancer cells by inducing apoptosis through diverse signaling pathways, which are coupled with caspases, Bcl-2 protein family members, and apoptosis inducing factors. 8
In cell death events where the apoptotic pathway is unavailable (for instance, in conditions were there are low ATP levels), 10,11 PDT can cause cancer cell death through the induction of a necrotic or autophagic mechanism. 14 –16
Necrosis
Necrosis is characterized by cell dysfunction through swelling and rupture of the mitochondria and/or cell membrane, which causes cellular cytoplasm to leak into the extracellular space and so overall induce cell lysis. 16
Autophagy
Autophagy is the process whereby organelles and the cell cytosol become encased in vacuoles termed autophagosomes and once fused with lysosomes, their contents are digested and recycled. 17,18 However, it is well known that if PDT induces autophagy in cells, they can sometimes recover from this form of cell death or become hyperactivated. 16,18 Generally, autophagy occurs in a Bax independent method and is usually stimulated in parallel with apoptosis, which destroys cancer cells. 19
These three mechanisms (apoptosis, necrosis, and autophagy) are dependent on a variety of parameters, including the nature of the PS applied, the PDT dose, as well as the genotype of the cells. 5,8
PDT challenges
The success of PDT is influenced by a number of factors such as how efficiently singlet oxygen is generated, which includes the chemistry of the PS used, the light intensity and wavelength utilized, as well as the initial oxygen concentration. 13 Even though conventional PDT has significantly improved the quality of life and life expectancy of patients with cancer, further advances in relation to its therapeutic efficacy are required to overcome some noted side effects (e.g., PS hydrophobicity and poor selectivity between diseased and healthy cells). 10,20,21
In more recent years researchers have been exploring new strategies to improve the effectiveness of PDT PSs, such as the possibility of integrating PDT PSs with nanotechnology to increase their efficiency. 22 According to Ulatowska-Jarza et al. and other scientists, 5,23 nanotechnology may assist in overcoming some of the difficulties associated with PDT PSs. Nanotechnology commonly deals with structures and systems with a size <100 nm, and these small nanostructures have unique physical, chemical, and biological properties that can be adapted and utilized within PDT PS applications. 24
Nanotechnology and Nanoparticles
The nanotechnology industry has matured and expanded at a rapid pace in the last decade, which has led to the research and development of nanomaterials with potential application in interdisciplinary fields such as medicine, electronics, and biomaterials. 5,24,25 Nanomedicine is defined as the use of nanotechnology in biomedical science and it utilizes nanomaterials that are precisely engineered for new diagnostic and drug delivery technologies in therapeutic treatment modalities. 25 One of nanomedicine's long-term objective is to transform and improve current healthcare systems by selectively targeting and fighting terminal diseases in more efficient ways. 5,24,26
The growing interest in nanomaterials is an attribute to their structural properties which are entirely different from both the molecule (atom) and bulk solid materials. 27 For instance, nanomaterials have an increased surface area to mass ratio which alters their reactivity tremendously, as well as other unique physical, optical, electronic, and chemical properties. 25,28,29 Thus to overcome limitations of some traditional diagnostic and therapeutic agents, these novel properties of nanomaterials could possibly be exploited. 5,25
Nanoparticles and PDT
In nanoparticle (NP)-based PS drug delivery systems, PSs are either encapsulated in or immobilized to NP platforms through covalent/noncovalent interactions. 32 A major advantage of conjugating photosynthetic drugs to NPs is the yield of high surface to volume ratio and high PS drug loading capabilities that these particles can attain. 33 More specifically, nanotechnology is attractive in PDT for three major reasons as follows: (1) targeting potential enhances PS concentration at the desired site and reduces toxic effects toward normal tissues/cells; (2) nanoparticles can improve the solubility of hydrophobic PSs; and (3) NPs can maintain a constant rate of PS delivery at desired sites due to zero-order release kinetics. 32 Thus in an effort to enhance PDT, functionalized NP platforms are utilized to promote either passive or active PS drug delivery in tumor cells. 34 PDT PS NP platforms consist of various types of organic and inorganic compounds such as liposomes, quantum dots, gold NPs, polymers, micelles, magnetic NPs, dendrimers, and carbon-based NPs 32 ; examples of various types of NP platforms have been illustrated in Fig. 3.
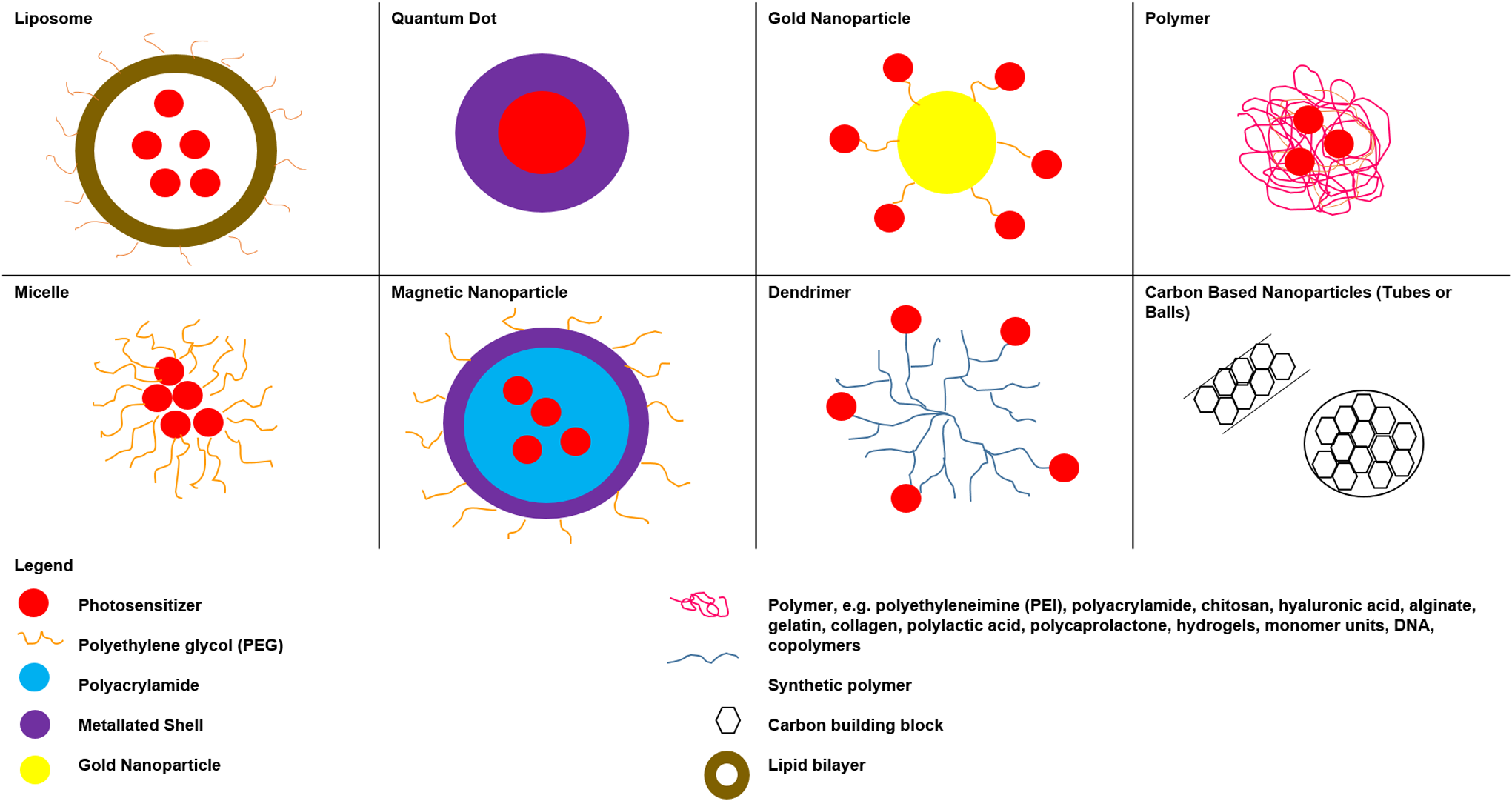
A variety of nanoparticle platforms are being studied for use in photodynamic therapy photosensitizer cancer drug targeting. These include liposomes, quantum dots, gold nanoparticles, polymer materials, micelles, magnetic nanoparticles, dendrimers, and carbon-based nanoparticles. 31
Organic nanoparticles
Organic NPs are composed of organic compounds such as lipids, proteins, polysaccharides, or polymers, which have low toxicity and versatility in terms of carrying a diverse selection of PS drugs. 35 Generally, in terms of PDT PS drug delivery organic NP platforms promote passive phagocytic absorption or controlled release of photosynthetic drugs. 36 –38 Passive biodegradable organic NPs include the following: liposomes, oil dispersions, dendrimers, polymeric particles, and polymeric micelles, whereas passive nonbiodegradable organic NPs include ceramic-based NPs such as silica, alumina, and titania. 34,38 A number of PDT studies have been listed in Table 1 which demonstrate the use of organic NPs, which passively accumulate in cancer cells due to the enhanced permeability and retention (EPR) effect. 2,9,20,35,39,40
HB, hypocrellin B; NPs, nanoparticles; PS, photosensitizer.
However recent studies have noted that passively absorbed PS drug carrying NPs can elicit acute hypersensitivity in normal cells, as they cannot exclusively differentiate between cancerous and normal cells, and so sometimes distribute in healthy tissues. 34,41,42 Thus in an effort to increase PS drug carrying NP specificity and reduce unwanted PDT PS NP passive uptake side effects, significant effort in recent years has been devoted to the synthesis and characterization of cell targeting PS NP bioconjugates which are only actively absorbed into specific cancer cells. 37
Inorganic nanoparticles
Inorganic NPs generally consist of an inner inorganic core composed of either a metal or a metallic oxide and an outer organic shell which stabilizes it in biological environments, while it transports photosynthetic drugs. 32 Further, inorganic NPs can be modified by the addition of biomolecules such as ligands or antibodies, which further enhance PDT PS tumor cell targeting as the drug can only be actively absorbed by specific receptors of tumor cells, eliminating any PS drug uptake or cytotoxic effects of PDT treatment occurring in healthy cells. 33,37 Moreover, inorganic NPs have unique size-tunable optical properties, which enhance their abilities to induce active cellular uptake of the photosynthetic drugs they carry, as well as PS light activation within the optimal therapeutic wavelength of PDT, or can be up-converted to emit high-energy photons upon excitation by the low-energy near infrared. 8,42 –44 Examples of active PS carrier NPs, which have been used in cancer treatments, include quantum dots, metal based NPs, up-converted NPs, magnetic NPs, and carbon-based NPs. 32 A number of PDT studies are listed in Table 2, which demonstrate the use of enhanced inorganic NP PS drug carriers, that actively/specifically accumulate in targeted cancer cells and so promote the PDT effect. 5,21 –23,46
NIR, near infrared; NPs, nanoparticles; PS, photosensitizer.
Conclusions
A variety of organic and inorganic NPs have been developed for targeted and effective delivery of photosynthetic drugs. This review demonstrates that NPs can offer solutions to address crucial limitations of conventional PS drug delivery and so enhance the overall efficiency of PDT cancer treatment. Nanomaterials combined with PS drugs increase the water solubility of hydrophobic PS drugs. NPs improve the target-specificity of PS drugs using passive targeting to tumor tissues through the EPR effect. Surface modification or up-conversion of PS loaded NPs with active targeting ligands further enhances the selective accumulation of PS drugs in tumors. However, it must be noted that a NP performance as PS drug carrier is dependent on the size and surface functionalities of the particle, the PS release rate, as well as the NP disintegration rate once absorbed into specific cells. 9
Thus nanotechnology PDT based therapies for cancer which have minimal side effects and high specificity are on the surge, where the main challenge is to develop a PS drug delivery nanosystem that is capable of circulating in the blood stream, which remains undetected by the immune system, however is recognized by the desirable tumor target, which is able to signal it for effective drug delivery. 5,34
Despite the significant efforts to develop modified nanosystems for efficient PDT cancer treatment, it still currently remains a challenge in research to develop a nanostructured drug delivery system based on surface-functionalized NPs that combine targeted tumor molecular recognition with effective production of reactive singlet oxygen from PSs under PDT irradiation, which are considered to be bio-safe in clinical settings and so require continuing investigation. 29,47
Footnotes
Acknowledgments
The authors sincerely thank the National Nanoscience Postgraduate Teaching and Training Platform (NNPTT), the University of Johannesburg, and the National Laser for their financial grant support. In addition, this work is based on the research supported by the South African Research Chairs Initiative of the Department of Science and Technology and National Research Foundation of South Africa (Grant No. 98337).
Author Disclosure Statement
There is no conflict of interest as no competing financial interests exist. In addition, the material in this review article has only been submitted to the journal Photomedicine and Laser Surgery and has neither been published nor is it considered for publication elsewhere.