
Abstract
Introduction
B
The symptoms referred by patients may vary depending on the severity of the neurosensory impairment, 12,13 the lower lip and the chin being the most affected anatomy structures. Paresthesia is usually observed, as also as hypoesthesia. 13,14 Hyperesthesia and allodynia are less common, but frequently cause more disturbances to the patients affected. 9,13
Many factors have been involved in the study of the neurosensory disturbance after BSSO, and some of them even had been placed as risk factors in the international literature, such as advanced age, manipulation of the inferior alveolar nerve during surgery, simultaneous third molar removal, associated surgery (genioplasty), and a small mandibular body. 15 –18 A Cone Beam study of the whole mandible as part of the surgery planning is recommended to help prevent neurosensory impairment. 16
In the numerous attempts to improve and accelerate nervous healing, photobiomodulation was discovered. 19 –21 Among its beneficial effects, researchers found a faster healing of the surgical wound, decrease of postoperative pain, and an increase in magnitude of neurosensory recovery, also restoring the normal function of the affected nerve in less time. 19 –21 These beneficial effects are related only to low-level laser application because the laser light does not produce a thermal effect on the cells (which is seen in high-level lasers used in surgery to cut different tissues). The biomodulation observed in different studies suggests that the cell absorbs the emitted photon and it translates it into energy, stimulating (or inhibiting) a chain of enzymes that activate the physiological processes of swelling and regeneration, mostly preventing the first and energizing the second. 19,22 The rise of the mitochondrial ATP and the intracellular calcium is part of the biological results obtained by stimulating the enzymes and it helps to explain how the cell is able to repair more quickly due to this extra energy produced. 23 The other process observed is that laser energy is best received in tissues with a greater fluid concentration. In patients with recent surgery and undergoing a swelling process, it increases the laser effect due to local edema. Laser light can also stimulate cells that were not exposed to the photons due to systemic effect. About this, researchers have found that the emitted photons reduce inflammatory biochemical markers (such as PGE2, mRNA Cox 2, IL-1β, and TNFα), neutrophil cell influx, and oxidative stress. 24 Some studies have also shown an effect on the lymphatic system associated to this, including better and faster drainage of the edema in the surgical site and carrying biochemical modulators supporting wound healing. This last observation is still on research. 24
Nowadays, the gallium–aluminum–arsenide diode (GaAlAs) is mostly used for photobiomodulation. This laser emits a continuous wave (CW) of 830 nm and an adjustable power of 10–70 mW, transmitted through an optic fiber. The light emitted by this laser has a high rank of penetration into the affected tissues, because the photon is barely absorbed by hemoglobin and water. This characteristic allows the treatment of anatomical structures located 4–8 mm under oral mucosa and bone. 22
The objective of this study was to evaluate the effect of the application of photobiomodulation in a 2-year follow-up period in patients who have been previously intervened with a BSSO and present neurosensory disturbance of the inferior alveolar nerve, due to this surgery.
Materials and Methods
This study is a 2-year follow-up study with two parallel groups, defined as Laser and Sham groups. Protocols and interventions of this investigation were approved by the Local Ethics Committee of Universidad de Los Andes (Santiago, Chile). The population involved is patients treated surgically with BSSO after being diagnosed with dentomaxillary anomalies and previous orthodontist management. The same maxillofacial surgeon, using a short reciprocating blade (REF 5100-37, cut edge 14.5 mm, thickness 0.38 mm), with the TPS reciprocating saw (Stryker CORE, Kalamazoo, MI), performed all surgeries under general and local anesthesia. Procedures were done in three private hospitals in Santiago de Chile. The pharmacological treatment considered antibiotics, nonsteroidal anti-inflammatory drugs (NSAIDs), and corticoids for all patients. Inclusion criteria were patients who underwent BSSO performed by the same surgeon, with a neurosensory deficit as a complication of this surgery and who did not suffer neurotmesis or partial section of the mandibular nerve during the procedure. No restrictions about gender, age, or skeletal class were considered. Exclusion criteria included patients with head and neck tumors, previous infection of the surgical site, nondiagnosed injuries, and treatment based on endogenous photosensible drugs (tetracyclines, griseofulvins, sulfonamides, and furocoumarins) or exogenous (retinoic or glycolic acid) drugs.
Sample size consisted of 73 patients (n = 73) treated in a preceding three-stage clinical trial as part of an investigation line started in Universidad de Los Andes. All patients were invited to participate in the study and provided previous informed consent. Of the 73 patients, 61 had received 8 low-level laser applications, distributed 3 of them during their hospital stay (days 1, 2, and 3 postoperative), and the other five left during postoperative evaluations at days 5, 10, 14, 21, and 28 after surgery. Clinical neurosensory tests were performed as follows: first test was performed the day before the surgery (as control test to compare the results for the postoperative evaluations), postsurgery tests were performed on days 1, 28, 60, 6 months, 1 and 2 years after the surgical procedure. The patients who did not received laser therapy (Sham group) underwent the same procedure as the patients treated with photobiomodulation but with the laser turned off, acting as placebo. Laser and neurosensory evaluations were taken from international literature and were performed as follows.
Photobiomodulation protocol
Laser light characteristics are shown in Table 1. GaAlAs low-level laser was used in each session (Flash Lase III; DMC Equipment, Sao Paulo, Brazil; 810 ± 20 nm, 0.1 W, CW, optical fiber probe with a round tip of 0.6 cm diameter, spot area 0.283 cm2). This laser equipment was previously calibrated for its use. Laser operators and participants used specific protection glasses. In addition, participants were bandaged. Four laser operators were trained and the laser equipment calibrated for its use. Intraoral infrared laser light application sites for all participants were both left and right sides: mandibular and mental foramen and osteotomy site (buccal side in relation to mandibular second molar). Laser protocol is presented in Table 2.
CW, continuous wave; GaAlAs, gallium–aluminum–arsenide diode.
Presented with medians (interquartile range).
Laser application technique consisted of 90 sec of laser application in contact with the patient (31.8 J/cm2, 9 J per site, 27 J in 270 sec of laser application in each session, and a total of 72 J during the whole treatment) in each site (three intraoral applications, 216 J after treatment, counting all sites intervened). 3,19,20 Laser was used in a CW (0.1 W/cm2, optical fiber probe, spot area 0.283 cm2, with a power density of 0.353 W/cm2). Intermaxillary orthodontic elastics were taken out during laser application. Sham group received the same applications, but laser light was turned on and off immediately for treatment so that the laser timer noise helped confusing the patient whether he or she was receiving laser light.
Neurosensory evaluation
Five neurosensory tests were performed in each patient.
• Visual Analog Scale (VAS) of General Sensibility 14,25,26 : The patient is given a visual scale with five different options. He or she must choose the one that fits better in relation to his or her personal perception of the affected area, being (1) lack of sensitivity, (2) almost none, (3) reduction, (4) almost normal, (5) normal. This was defined as an ordinal variable. A control test was performed 24 h before the surgery and the results were used to determine if there was any alteration in the response of the patient after surgery on the same test.
• Sensitivity threshold test: A nylon monofilament (equivalent to 5.07 Von Frey hair filament) is used to observe if the patients are capable of recognizing the direction in which the filament passes through their lower lip (site 1) and chin (site 2). Longitudinal movements are performed without a logical sequence. Out of 10 trials, the patient must correctly indicate the direction in 7 to consider the test positive. This was defined as a dichotomous variable. A control test was performed 24 h before the surgery and the results were used to determine if there was any alteration in the response of the patient after surgery on the same test.
• Two-point discrimination: Using a dry-point compass with a light pressure on the patient skin, the minimum value at which the patient discriminates between one point and another was measured at sites 1 and 2. The distance between the points of the compass was established at 15, 10, 7, 5, and 3 mm. To avoid sequence guessing, no logical arrangement was followed. This was defined as a dichotomous variable. A control test was performed 24 h before the surgery and the results were used to determine if there was any alteration in the response of the patient after surgery on the same test.
• Pain discrimination: Using a dry-point compass, sites 1 and 2 were harmlessly punctured bilaterally, with the same pressure. The patient was given a visual scale to indicate the painful response to the stimuli. The response to painful stimulation was considered positive when the patient indicated feeling the same amount of pain than in the control test (24 h prior surgery) using the visual scale, being 0: no pain, 2: mild sensation, 4: mild pain, 6: moderate pain, 8: severe pain, 10: maximum pain. This was defined as an ordinal variable (for the visual scale) and as a dichotomous variable (positive or negative response to the test). A control test was performed 24 h before the surgery and the results were used to determine if there was any alteration in the response of the patient after surgery on the same test.
• Thermal discrimination: Using an anesthesia tube tempered at a constant temperature of 43–44°C (registered constantly with a thermometer), the patient indicates whether he or she feels the warm stimuli in sites 1 and 2 bilaterally or not. On the contrary, cold was tested cooling an anesthesia tube with ethyl chloride and applying it in the same sites. No logical sequence was used to apply the warm or cold tubes in sites 1 and 2 bilaterally, so the patient could not guess which tube was going to be placed next. This was defined as a dichotomous variable. A control test was performed 24 h before the surgery and the results were used to determine if there was any alteration in the response of the patient after surgery on the same test.
All neurosensory evaluations were performed 24 h before the surgery (basal test), 24 h after the surgery (neurosensory impairment indicator), 28 and 60 days, 6 months, 1 and 2 years after surgery. Evaluations were executed in a dark, quiet, and comfortable room, with patients' eyes closed. Each test was explained and demonstrated to all participants before execution, using the patient's hand as a control site. All five tests were done individually, by the same operator, in the same sequence, but not in the same order within each test. This neurosensory evaluation is the result of other neurosensory tests gathered from international literature. 4,10 –12,19,20,25 –29 Between each test, patients were asked to remove the eye bandage for the explanation of the next test. For the purpose of each test, two anatomic sites were defined for each left and right side: site 1 was lower lip and site 2 was the chin, in a standardized point 20 mm below oral commissure, drawing an imaginary vertical line from this point (in relation to the mentolabial sulcus).
The variables in this study were defined as follows: independent variable was the exposure or nonexposure to laser light; dependent variables were neurosensory return measured by dichotomous tests (tactile directional discrimination, two-point, pain and thermal discrimination) and ordinal tests (VAS for pain and sensitivity). Other factors were correlated with a potential increase in neurosensory disturbance after BSSO and were determined as confounding variables, being age, skeletal class, direction and magnitude of mandibular movement, intraoperative inferior alveolar nerve manipulation, associated mandibular surgery (genioplasty), simultaneous third molar removal, rigid fixation use, and mandibular nerve accident.
Sample size was determined by the number of patients treated in the previous three-stage clinical trial, realized between June 2011 and February 2014 in Universidad de Los Andes, including all patients who received BSSO performed by a surgeon. Before laser therapy, patients were randomly distributed in the Laser and Sham group following simple randomization procedures using Stata 12.1: Data Analysis and Statistical Software (Stata Corp, College Station, TX). Centralized assignment with a third person who communicates via e-mail, giving participants allocation, was used. Neurosensory examiner and patients were blinded to intervention until 6 months after surgery (three-stage clinical trial end).
Medians and interquartile range were used to describe ordinal variables and relative and absolute frequencies for dichotomous variables. The group's comparison for ordinal and dichotomous variables was made with Mann–Whitney's and Fisher's test, respectively.
Results
Participant flow is shown in Fig. 1. Twenty-eight patients from the Laser group failed to complete follow-up period. Five patients were living in foreign countries when the experiment was conducted, 13 voluntarily withdrew from the study, and 10 lived in cities far away from the clinical center. On the contrary, three patients from the Sham group voluntarily decided not to participate in the study. The final sample of patients consisted of 42 patients, 33 in the Laser group and 9 in the Sham group.
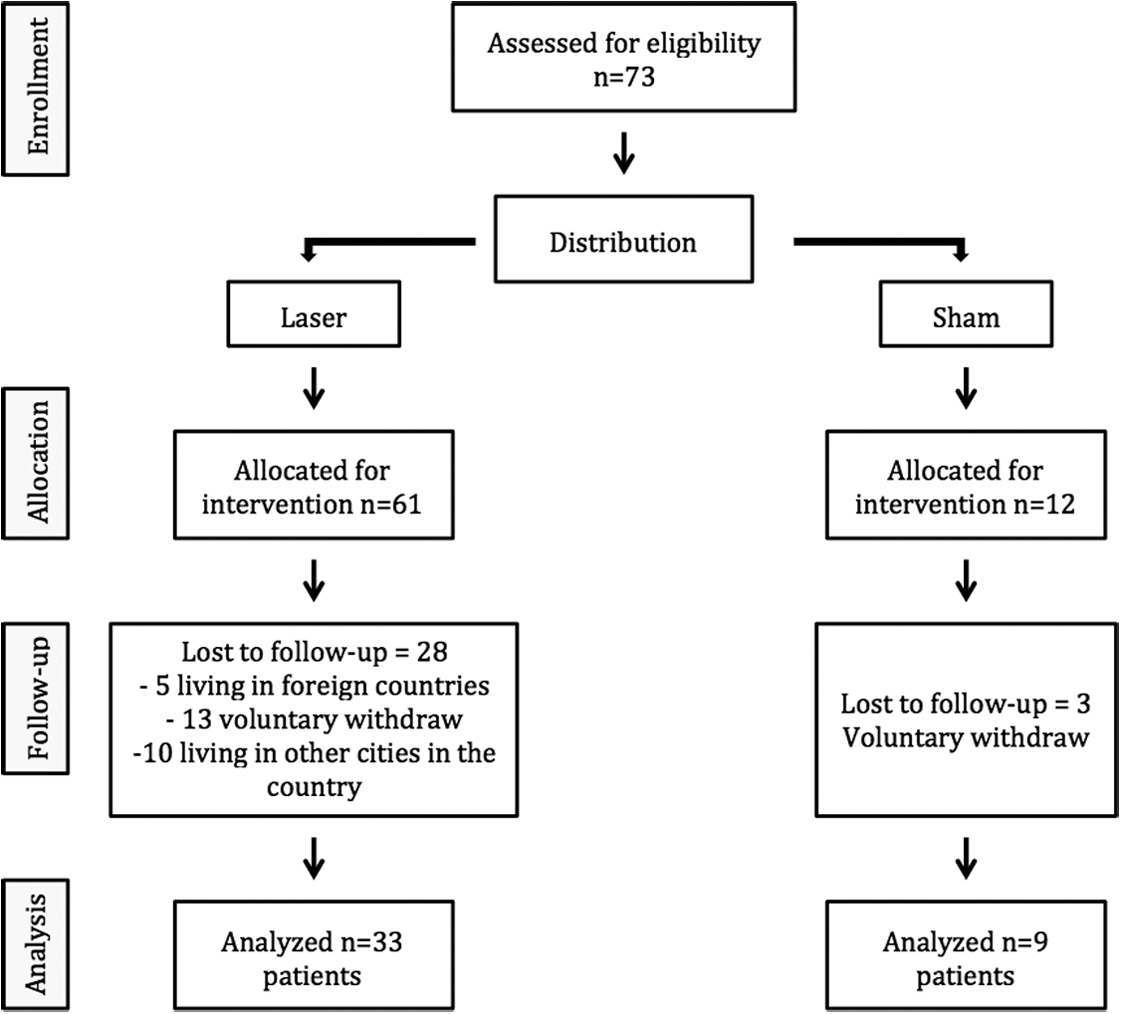
Flow chart of participants involved in the clinical trial. Recruited and loss sample until group conformation.
Even though all participants were blinded to intervention, some patients from the Laser group felt a tingling sensation after laser application, which led them to presume they were part of the Laser group.
Table 2 shows demographic and clinical characteristics of the evaluated patients. Results found on this research are presented in Table 3, showing a follow-up period of 6 months, 1 and 2 years after surgery, percentage of recovered patients for each group, and p-value associated to each test and follow-up time. Statistical relevant results are marked with an asterisk and bold font.
Percentage of recovered patients and p-value associated to each test. Statistical relevant results are shown with an asterisk and bold font.
VAS, Visual Analog Scale.
Discussion
BSSO surgical technique has a wide range of complications, the neurosensory alteration of the inferior alveolar nerve being the most prevalent. Results in this and other studies demonstrate that the lower lip and chin skin are the most affected anatomical structures. 3,19,20,30,31 Outcomes also show clinical improvement in time and magnitude of neurosensory return for the Laser group.
The beneficial effect of photobiomodulation seen in this study was also found in the scientific literature during several years of research (Khullar et al., 20 Miloro and Repasky, 3 Ozen et al., 19 Führer et al. 25 ). Laser application using GaAsAl laser light appears to be a treatment that successfully restores neurosensory function after BSSO.
Restoration of normal neurosensory function is conditioned by many factors, specially the neurosensory damage degree. In this study, all patients who received the therapy indicated feeling a better neurosensory recovery than those who did not receive laser light treatment, but most of these patients also felt a tingling sensation during laser applications, leading them to believe (or to acknowledge) that they were receiving the treatment, affecting the psychological response of the patient toward laser therapy.
Literature supports that certain characteristics of the patient and intraoperative factors can affect the development and severity of the neurosensory disturbance. 16,19,32,33 In this study, we observed that patients with advanced age and those who suffered intraoperative manipulation of the inferior alveolar nerve presented a more severe alteration of the mandibular nerve. Although not enough patients had simultaneous removal of third molars to conclude this as a risk factor in neurosensory impairment development, this combined surgery is rarely done for extraction of third molars, is usually indicated as part of the preoperative treatment to avoid pathological fractures of the mandibular angle, 32,33 and it is preferable to elude simultaneous third molar removal during orthognathic surgery because its relationship in the development of a more severe dysfunction of the mandibular nerve has been observed. 19,32,33
Neurosensory alteration development is always a matter of concern to the surgeon, but due to BSSO characteristics, it is rarely prevented. The mandibular ramus split determines that at least there will be a swelling response of the healing tissues around the mandibular nerve. This swelling compresses the nerve leading to its malfunction. 10,34 In best cases, resolution of the inflammatory process restores the nerve function, but usually the mandibular nerve is affected by other injuries during the BSSO-like traction and compression of its fibers that triggers different degrees of neurosensory impairment. 25 These lesions take weeks, months, or even years to heal in a nervous cell, because of its high complexity and biological specialization. 10,35
As expected in this study, not all patients manifested the same symptoms. Most common among participants was paresthesia of the lower lip and chin skin. Other symptoms contemplated hypoesthesia, anesthesia (first 48 h after surgery), tactile and thermalgesic alterations, hyperesthesia, and allodynia.
Photobiomodulation accelerates this healing process by triggering several biological mechanisms: it promotes microcirculation in the affected area, reducing the local swelling of the surgical wound and the compression around the nervous structure; it moderates inflammatory response by decreasing secretion of inflammatory mediators, favoring healing of the surgical wound; it stimulates mitochondrial metabolism producing excess of ATP that the cell can use to improve the healing process; it inhibits the secretion of nitric oxide (NO) protecting the nervous cell from its neurotoxic effects and by reducing the oxidative stress; and finally, laser light acts directly on rhodopsin kinase stimulating the production of different proteins that induce the nervous cell to repair, such as the nerve growth factor (NGF), calcitonin gene-related peptide, and the GAP-43 protein. 19 –21 Because of these beneficial biological effects (specially the inhibition of NO), some authors recommend starting photobiomodulation 48 h prior surgery. 36 However, the specific biological mechanism of photobiomodulation for neurosensory recuperation has not been completely clarified yet.
No laser treatment protocol has been established in literature, and there are several alternative schemas. A minimum of ten sessions is commonly agreed, ideally three times per week, with direct laser light application on the affected area (intra- and extraorally).
This study was conducted with healthy men and women from different age groups, diagnosed with II to III skeletal class. The wide range of population included in this investigation allows the reproduction of this study in various patients undergoing orthognathic surgery.
Our results show that neurosensory return in both groups was similar within the first 28 days after surgery, except for general sensitivity where both groups showed an alike neurosensory recovery up to 60 days after surgery. Nevertheless, normal neurosensory perception was achieved by a larger group of patients in the Laser group for all the tests performed, suggesting a positive effect of photobiomodulation in the treatment of neurosensory disturbance after BSSO surgery. Further clinical trials and follow-up studies are required to support laser therapy and the application protocol seen in this investigation.
Study limitations include the lack of calibrated instruments to perform the neurosensory tests, the use of subjective tests to evaluate the neurosensory impairment, the absence of a standardized protocol for laser application, physiological adaptation of untreated patients to neurosensory deficit that can lead to false-positive results in tests, results that cannot be extrapolated to other populations in other countries, the loss of patients in the follow-up period (because they declined to join the study), and the unequal and insufficient number of participants in both groups. This last limitation was caused by the fact that all participants from the three-stage clinical trial, as part of the ethical protocol at the end of the investigation, were invited to receive photobiomodulation, reducing the number of patients in the Sham group. Statistical analysis was made to weigh group distribution. The results show that with the tests used in this study to evaluate the data obtained, significant statistical results could be achieved, although homogeneity for studied groups (number of participants and clinical condition) is suggested for more trustful results. Further follow-up studies on this field should not be performed without at least 25 participants in each group.
For future clinical trials, the inclusion of a false laser light (made by the same manufacturer, with the same characteristics) is recommended so that the operator cannot distinguish whether laser light is being applied or not (double blinded).
Conclusions
Photobiomodulation, using GaAsAl laser light, showed a beneficial effect on the sample used in this study compared with the Sham group. In this study, 85% of neurosensory return was reported in treated patients, while the Sham group only recovered 70–75% of normal perception.
Footnotes
Acknowledgments
To Dr. Antoni España as reviewer in the preparation of the final article.
Author Disclosure Statement
No competing financial interests exist.