
Abstract
Introduction
C
One disadvantage of ceramic brackets is the debonding procedure. 4 Ceramic is a very hard and brittle material with a correspondingly low modulus of elasticity. There is consequently a greater risk of fracturing the ceramic brackets and enamel during debonding. 6 Reports in the literature suggest that increasing the bond strength to the enamel surface in ceramic brackets may increase the risk of enamel fractures or bracket fractures during the debonding procedure. 6 –9 For aesthetic reasons, ceramic brackets are often used in the upper front teeth. Damage to the enamel in these teeth may require substantial restorative treatment. In addition, bracket fractures make it impossible to re-use the same bracket in a corrected position. Additional risks are aspiration, ingestion, and damage to the eyes caused by ceramic fragments. The remaining bracket base fragments on the tooth also need to be removed with a diamond bur in a high-speed handpiece. This leads to longer treatment times and considerably increases the risk of enamel damage. 10
Various methods have therefore been developed to simplify the debonding procedure with ceramic brackets. One of these is the use of special pliers for specific bracket systems 11 for mechanical debonding. Another option is to influence the bracket failure mode using electrothermal debonding devices. 4,12,13
In recent years, the use of high-energy lasers in orthodontics has focused on facilitating the ceramic bracket debonding procedure. The efficacy of laser systems such as the neodymium-doped yttrium aluminum garnet (Nd:YAG), 14 –16 diode laser, 4 CO2 laser, 10,17 ytterbium fiber lasers, 18 Er:YAG laser, 19 and Tm:YAP 20 has therefore been investigated (Table 1). A previous study has shown that removing ceramic brackets using a novel diode laser with a wavelength of 445 nm influences the failure mode, so that the risk of ceramic bracket fractures can be reduced. 21 On the basis of micrographs evaluated at magnifications of 10 × and 20 × and scanning electron microscopy images, the significantly reduced amount of residual adhesive material on the enamel surface after laser application did not lead to a greater risk of enamel defects. 21 The brackets were removed in the study using bracket removal pliers immediately after laser application. Bracket debonding using pliers involves the application of shear, pressure, and tensile forces and represents the conventional treatment method. This method led to low adhesive remnant index (ARI) values, but it was not possible to investigate the influence of the novel diode laser on the precise shear bond strength (SBS) values that are needed for bracket debonding.
Definition of the laser parameters in different studies with the focus on laser-assisted bracket debonding; W (Watt) SI = [W].
The aim of this study was to investigate the influence of the novel 445-nm diode laser on SBS and the enamel surface, testing the hypothesis that using the novel diode laser before debonding of ceramic brackets significantly reduces the shear bond forces (SBS values), consequently reducing the risk of enamel fractures and bracket fractures during the debonding procedure.
Materials and Methods
Sample selection and bracket placement
Thirty caries-free human third molars with an intact enamel surface were used. All the teeth being studied had been extracted for orthodontic or surgical reasons. The study was conducted in full accordance with standard ethical principles (World Medical Association Declaration of Helsinki, version VI, 2002). Patients were informed that their teeth were to be used as part of a research project. Immediately after extraction, the teeth were stored in a physiological saline solution containing 0.001% sodium azide. The roots of the teeth were removed using a diamond cutting disc (Superdiaflex G®; Horico, Berlin, Germany). The clinical crown was embedded in Palavit G® (Heraeus Kulzer, Wehrheim, Germany). A cylindrical plastic tube with a diameter of 16.5 mm was used as a pillar (Hornbach-Baumarkt-AG, Neustadt, Germany). The crowns were aligned with their vestibular surfaces parallel to the upper end of the test tube. To provide a standardized enamel surface, the molars were planed and polished in a second step using an interproximal polishing system (O-drive OD30 instrument®, KaVo, Biberach, Germany) with an oscillating grinding wheel (OS® segment discs; Komet, Besigheim, Germany). The whole process was controlled microscopically under 20 × magnification. Each tooth was randomly assigned, on a computer-generated basis, either to the laser-assisted debonding group (laser group) or to the conventional debonding group (control group), resulting in 15 samples in each group.
A commonly used polycrystalline, active and self-ligating bracket system called In-Ovation C (GAC, Gräfelfing, Germany) was used in a preliminary survey. 21 The bracket base for this needed to be as flat as possible, as the brackets are mounted on flat enamel surfaces so that the maximum adhesive strength can be achieved. The bracket of tooth 11, with a base size of 16 mm2, was therefore used. Before bracket bonding, the teeth were dried with a dental air syringe, followed by conditioning of the enamel surfaces with GEL ETCH® (5 mL phosphoric acid; Ormco Corporation, Orange, CA) for 20 sec. The etching gel was removed using a water spray and the enamel surface was dried with a dental air syringe. Subsequently, the enamel surface was coated with the bonding agent Transbond XT® (3 M Unitek, Monrovia, CA). The brackets were bonded to the tooth in a standardized manner using Transbond XT adhesive paste (3 M Unitek). Transbond XT is a commonly used adhesive system for bracket bonding and has a high adhesive strength. 4,22 Before polymerization of the adhesive paste, each bracket was applied to the tooth for 10 sec with a force of 300 g (Correx Force Gauge, Bern, Switzerland). 6 The curing took 40 sec for each bracket, using a light-emitting diode (LED) device with a light intensity of 1200 mW/cm2 (Elipar™ FreeLight™ 2, 3 M ESPE, Neuss, Germany). To ensure maximum adhesive strength, the samples were stored in a physiological saline solution containing 0.001% sodium azide at a temperature of 37°C for at least 24 h. 10,20
Laser system
A novel class IV diode laser system (SIROLaser Blue; Sirona, Bensheim, Germany) with a wavelength of 445 nm was used for laser-assisted debonding. The system was set to an output power of 2 W/cm2 (2 J/cm2) in continuous-wave mode (CW), resulting in an effective output 1.76 W/cm2 (±0.05 W/cm2) at the fiber tip. These parameters have been found to be appropriate for debonding, as shown in a previous study 21 (Table 2). The handpiece was used with a 320-μm (core diameter) fiber and was activated with a finger switch.
Definition of the laser parameters in this study; W (Watt) SI = [W]; J (Joule) SI = [J]; cw, continuous wave mode.
Debonding
The diode laser can transfer its energy by absorption into pigmented tissues or materials. As the ceramic brackets and the adhesive material contain few pigments, each bracket base in the laser group was blackened laterally and cranially using a black crayon before debonding (edding® 400; edding Vertrieb Ltd., Wunstorf, Germany) (Fig. 1).

A bracket base in the laser group, blackened laterally and cranially with a black crayon (edding®400, edding Vertrieb Ltd., Wunstorf, Germany) before debonding.
Shear tests were performed on a standardized and computer-controlled hydraulic testing machine (Zwick 1120.25; Messrs. Zwick, Ulm, Germany). Immediately before bracket removal, laser energy was applied to three sides of the bracket bases for 5 sec each (lateral–coronal–lateral, a total of 15 sec) using the laser tip in contact mode in a 90° angle to the bracket surface (Fig. 2). This results in a total dose of 30 J/cm2. The bond strength was measured in shear mode at a crosshead speed of 1 mm/min until bracket removal was achieved. The SBS needed to debond or initiate bracket fracture was recorded and then converted into pressure (MPa) as a ratio of force per bracket surface area (16 mm2).
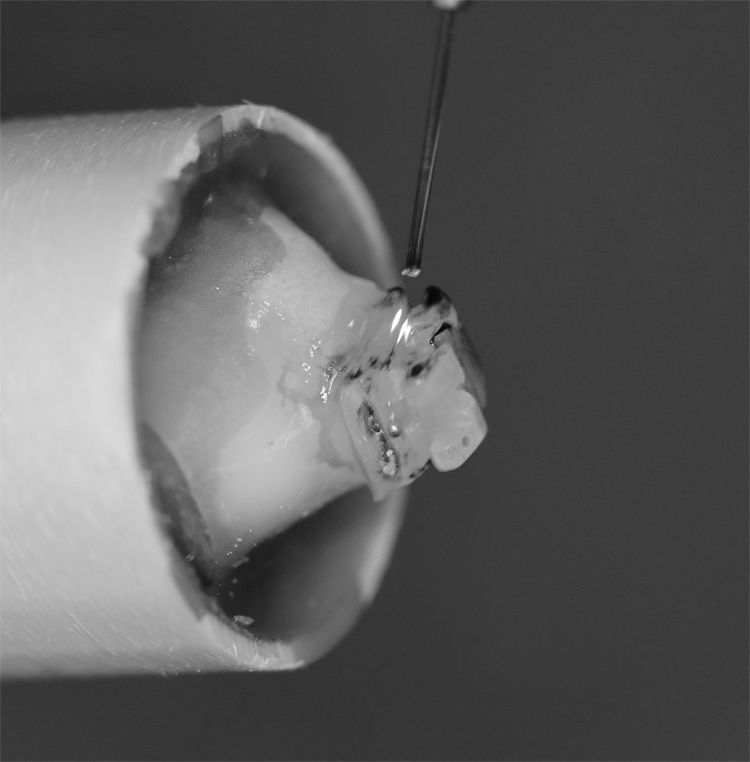
Laser application, with the laser tip in contact mode at a 90° angle to the bracket surface.
Adhesive remnant index
After bracket removal, the enamel surfaces were examined using a light microscope and the corresponding ARI score was assessed 23 using 10 × magnification. The following classification of ARI scores was used: 0, no adhesive remaining on the tooth; 1, less than 50% of the adhesive remaining on the tooth; 2, more than 50% of the adhesive remaining on the tooth; and 3, all of the adhesive, with a clear impression of the bracket base, remaining on the tooth.
After bracket removal, photomicrographs of the enamel surface were taken with 10 × magnification.
Statistics
Statistical calculations were carried out using SPSS, version 17.0 (SPSS, Inc., Chicago, IL) and the G*Power® program (Franz Faul, University of Kiel, Germany). Normal distributions for SBS values and pressure were tested using the Shapiro–Wilk test. As the values were normally distributed, t-tests were then carried out to analyze intergroup differences. The distribution of the ARI scores was analyzed using the chi-squared test. For all tests, the significance level was set at p < 0.05.
Power analysis was used to estimate the number of cases required, which yielded 15 samples per group to achieve a test power of p > 80%, an α error of 0.05, and an effect size of 0.98 with two-sided observation.
Results
Shear bond strength
Comparison of the SBS values observed in the two groups showed that they were significantly lower statistically in the laser group than in the control group (p < 0.05; Table 3). Accordingly, the pressure values in the laser group were also significantly lower statistically (p < 0.05; Table 3 and Fig. 3).
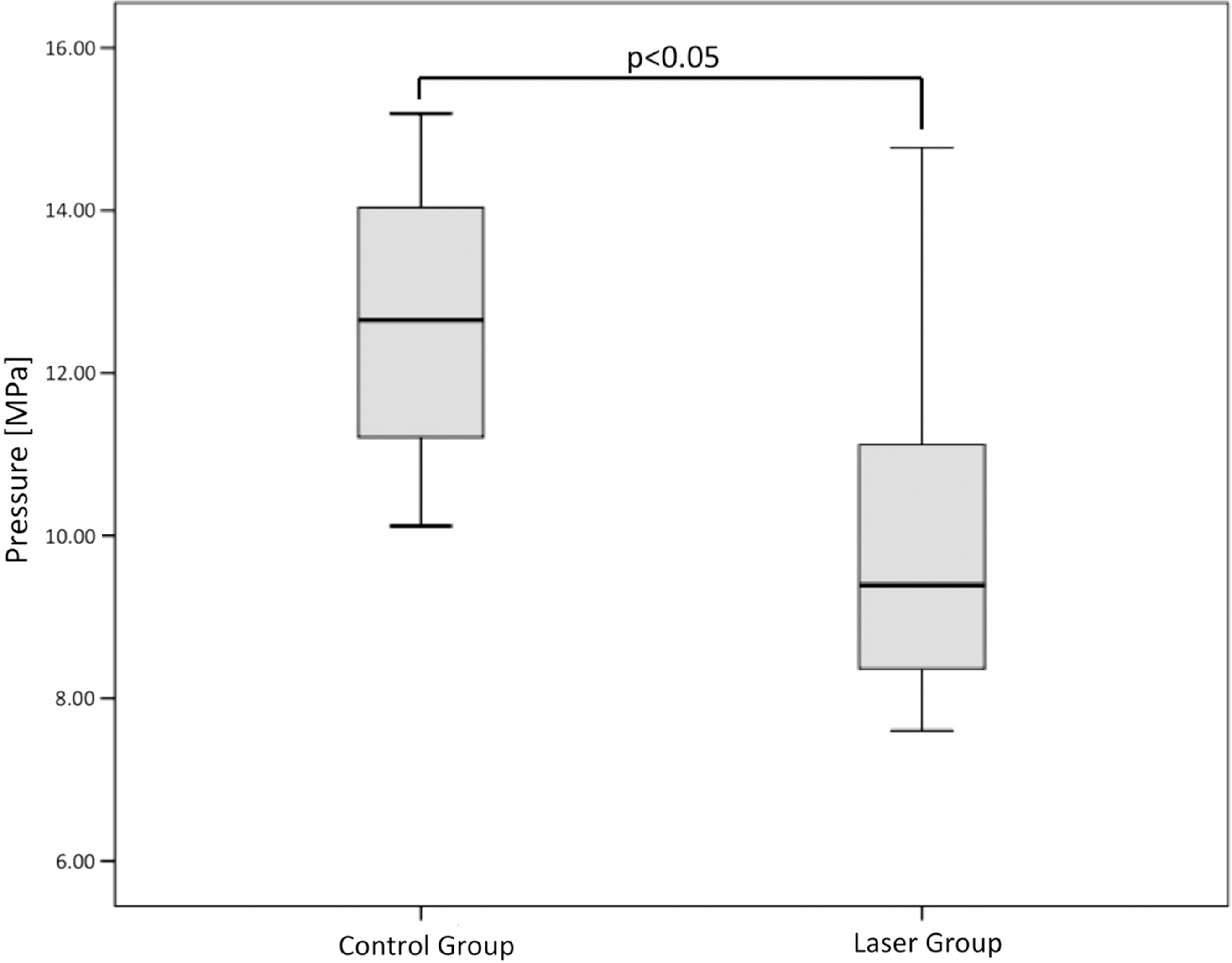
Box plot diagram of shear bond pressure, showing a statistically significant difference between the laser group and the control group.
ARI and photomicrographs
A statistically significant difference (p < 0.05) in the value distribution was observed when the ARI scores in the conventional and laser groups were compared, without and with 10 × magnification. The percentage with an ARI score of 1 was higher in the laser group than in the control group (46.7%; Table 4), while the percentage with an ARI score of 2 was higher in the conventional group than in the laser group (93.4%; Table 4). No enamel fractures were visible even under 10 × magnification in any of the samples (Table 4 and Fig. 4).

Exemplary photomicrograph (10 × magnification) of the enamel surface after laser-assisted bracket debonding.
Frequency and percentage distribution of the adhesive remnant index scores (ARI) detected at 10 × magnification in the control group and laser group.
Enamel and bracket fractures
During the whole bracket debonding procedure, no bracket fractures occurred either in the laser group or in the control group, nor were any enamel fractures identifiable under 10-fold magnification in either group.
Discussion
The aim of this study was to investigate the impact of a novel 445-nm diode laser, before debonding, on the SBS and consequently the risk of enamel and bracket fractures. The results show that the shear bond force needed to debond the brackets was lower in the laser group than in the control group. SBS and pressure values were significantly reduced statistically in the laser group (p < 0.05) (Fig. 3). The laser system used thus led to a reduction in SBS values with the bracket and adhesive system investigated.
An earlier study in which a different diode laser and a different polycrystalline bracket system were used came to the opposite conclusion. 4 A statistically significant reduction in the SBS values was not achieved using a diode laser in the study. However, the results are of no clinical relevance, as the laser system and laser parameters used are not reported in the article, so it is not possible to compare the settings and results. 4 The diode laser used in this study is the first that works at a wavelength of 445 nm. It is not at present clear whether different wavelengths in the laser systems or the bracket system itself may lead to different results, and further research on this is needed.
These findings, based on 10 × magnification, show that the ARI scores are statistically significantly lower in the laser group than in the control group. An ARI score of 2 was achieved in 93.33% of the control group samples (14 of 15; Table 4). An ARI score of 2 was achieved in only 46.66% of the laser group samples (seven of 14), while an ARI score of 1 was noted in seven other samples (Table 4). This confirms the results of an earlier study by our own group, 21 based on almost the same experimental setup and using the same diode laser device. The only difference was the debonding procedure, which was carried out immediately after laser application using bracket removal pliers. The results of both this study and the earlier one 21 differ from the results of other studies with other laser systems, which have reported higher ARI score values in the laser group than in the conventional group. 4,19,24
In general, the literature recommends achieving high ARI values during the bracket removal procedure, as these correspond to the highest possible amount of residual adhesive material on the enamel surface after bracket removal. This should ensure the lowest risk of damage to the enamel, such as fractures. 25 –27 The samples from the two groups examined in this study confirm the results of our own and other recent studies, which did not identify a higher risk of enamel fractures due to smaller ARI scores. 19,21,23 No enamel fractures were found on the enamel surfaces under 10 × magnification. Along with the reduced ARI scores, this suggests that the novel diode laser system led to reduced adhesion and consequently to a reduction in the risk of enamel and bracket fractures. The results thus confirmed the hypothesis on which the study was based.
In an earlier study, the brackets were removed immediately after laser application using bracket removal pliers. An ARI score of 0 was noted for 60% of the laser group samples. 21 As additional removal of residual adhesive material was not necessary, the study mentioned that this procedure might lead to time-saving during bracket debonding. This result was not confirmed in this study, as an ARI score of 0 was not achieved in either group. The difference might be due to the method of force application. Bracket debonding using pliers involves the application of shear, pressure, and tensile forces, while the SBS test only applies a vertical force at right angles to the bracket base.
All the conclusions and results presented in this study are limited to the Transbond XT 3 M Unitek adhesive system and the In-Ovation® C GAC bracket system that were used in this study. The possible effects of the novel 445-nm laser device on other ceramic brackets or adhesive systems are not currently known, and further research will be needed to investigate this.
As mentioned earlier, pigmented tissues or materials have to be present so that energy can be transferred to the adhesive system. It is therefore necessary to blacken the brackets, which are low in pigmentation, before the laser application. Use of an adhesive material enriched with pigments might save time during this step and might simplify the process of ceramic bracket debonding when a diode laser system is used.
Comparing the laser-assisted debonding procedure to the conventional method, the question arises if the difference of the debonding behavior is created by the interaction of the laser radiation with the enamel water content. In this case, we must distinguish between the different laser systems. The Er:YAG laser, for example, gets absorbed by water because of the 2940 nm wavelength and leads to enamel microexplosions. Based on this effect, the Er:YAG laser is able to remove dental hard tissue. Consequently, this interaction is a difference compared to the conventional debonding method. 19,28 In contrast to the Er:YAG laser, the laser radiation of the 445 nm diode laser is not well absorbed by water and the interaction with the enamel water content is nearly negligible. 29
The active self-ligating ability of the brackets used in this study is based on an integrated cobalt chrome flap, which is covered by rhodium. Metal is characterized by a higher thermoconductivity than ceramic material. This leads to the question that the metallic flap could lead to a higher thermal conduction into the pulp. The metallic flap is surrounded by ceramic material with no direct contact to the enamel surface. We assume a subordinate impact of the metallic thermoconductivity. Studies showed that the pulpal temperature increased 1.46°C by utilizing a 980 nm diode laser (2.5 W) for 10 sec in continuous-wave mode during laser-assisted bracket debonding 30 and waterless application of an Er:YAG laser lead to an increase of 4.59°C in the pulp. 28 A preliminary survey evaluating a 445 nm semiconductor laser showed only minor impact of laser irradiation with the used power settings on temperature increase inside the pulp chamber. Moreover, the previously published data on the influence of blood circulation during external laser irradiation suggest that laser application for bracket removal might not exceed the biological tolerable temperature threshold. 31
The enamel surface shows no signs of overheating after the debonding procedure using the 445 nm laser (Fig. 4). The question arises if there is a difference between ceramic brackets or metallic brackets focusing on heat development on the enamel surface by the use of the 445 nm laser during bracket debonding. This question cannot be answered by this study and no literature is available, which investigated the behavior of the novel 445 nm laser during debonding of metallic brackets. Further studies need to follow.
In one study, it was reported that ceramic brackets fell off the tooth immediately after laser irradiation when an Er:YAG laser was used. 18 However, none of the brackets dropped off immediately after laser application in this study. Instead, it might be assumed that the diode laser caused thermal softening of the adhesive system, with the thermal reaction leading to an increase in the temperature of the pulp chamber. However, temperatures were not measured during this study. Further research will therefore be needed to assess possible temperature increases in the dental hard and soft tissues during laser application.
Conclusions
This in vitro study verified that the SBS values needed for bracket debonding can be statistically significantly reduced using a novel 445-nm diode laser device. Micrographs of the enamel surface after bracket removal under 10-fold magnification showed lower ARI scores in the laser group. No enamel fractures were observed. The laser-based method presented in this study might therefore be capable of simplifying bracket debonding, leading to a reduction in possible adhesive remnants and/or tooth damage, and a reduction in the overall treatment time.
Footnotes
Acknowledgments
The authors thank Densply Sirona for providing the laser device.
Author Disclosure Statement
The authors declare that there is no conflict of interests.