
Abstract
Introduction
P
Pulsed dye laser (PDL) is at present the gold standard for the treatment of PWS according to the principle of selective photothermolysis to ablate the PWS vessels. 4,5 It has been shown that PDL with shorter treatment intervals may provide more effective therapy for PWS. 6 –8 East Asians, compared with Caucasians, have more melanin in their skin, causing more light absorption in the epidermis, resulting in slower recovery of epidermal change and more pigmentation postlaser treatment. 9 However, no study of the optimal PDL treatment intervals for East Asians with PWS has been reported to date.
This study aims to perform a side-by-side comparison to investigate the safety and effectiveness of the PDL treatments at 3- and 6-week intervals in East Asian patients with PWS.
This study was approved by the investigational review board of the Shanghai Ninth People's Hospital. All patients, minors and adults, gave their informed verbal and written consent or assent before study enrolment.
Method
Patients
We prospectively investigated 39 East Asian patients with untreated PWS. Half of the PWS lesions was randomly allocated to be treated at 3 weeks and the other half at 6 weeks. Both halves of the PWS were treated three times in total. The facial and neck area were subdivided into eight areas (upper cutaneous lip, nose, lateral aspect of the cheek, medial aspect of the cheek, periorbital, temple/forehead, chin, and neck) (Fig. 1). Two test treatment sites (3- and 6-week interval sites) on each patient were divided into the same subanatomical area. 10 –12
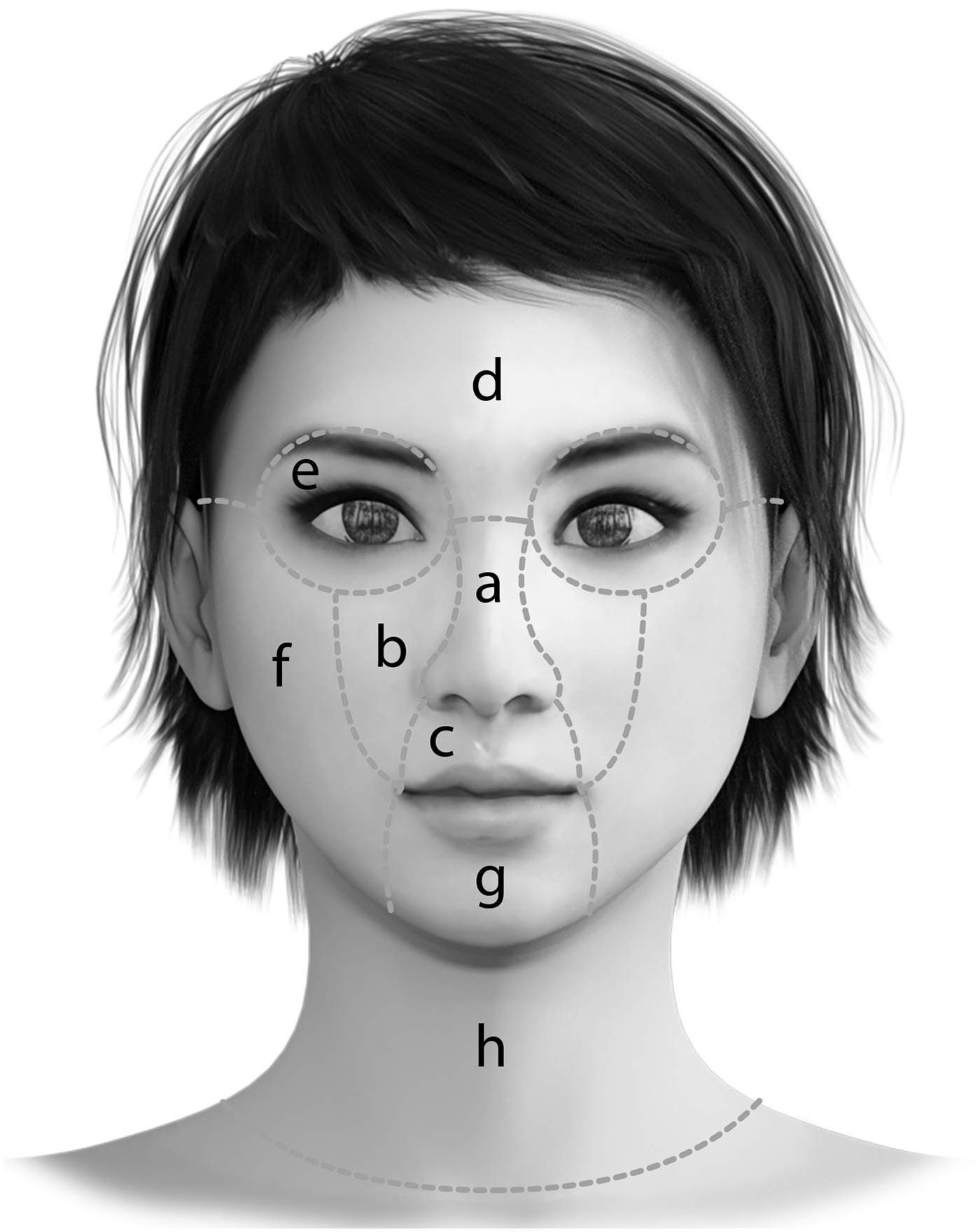
Facial and neck anatomic locations were subdivided into eight regions according to Renfro and Geronemus
10
: nose
The sites for treatment using PDL at 3-week intervals and PDL at 6-week intervals were selected by randomization (Fig. 2): A software program was used (
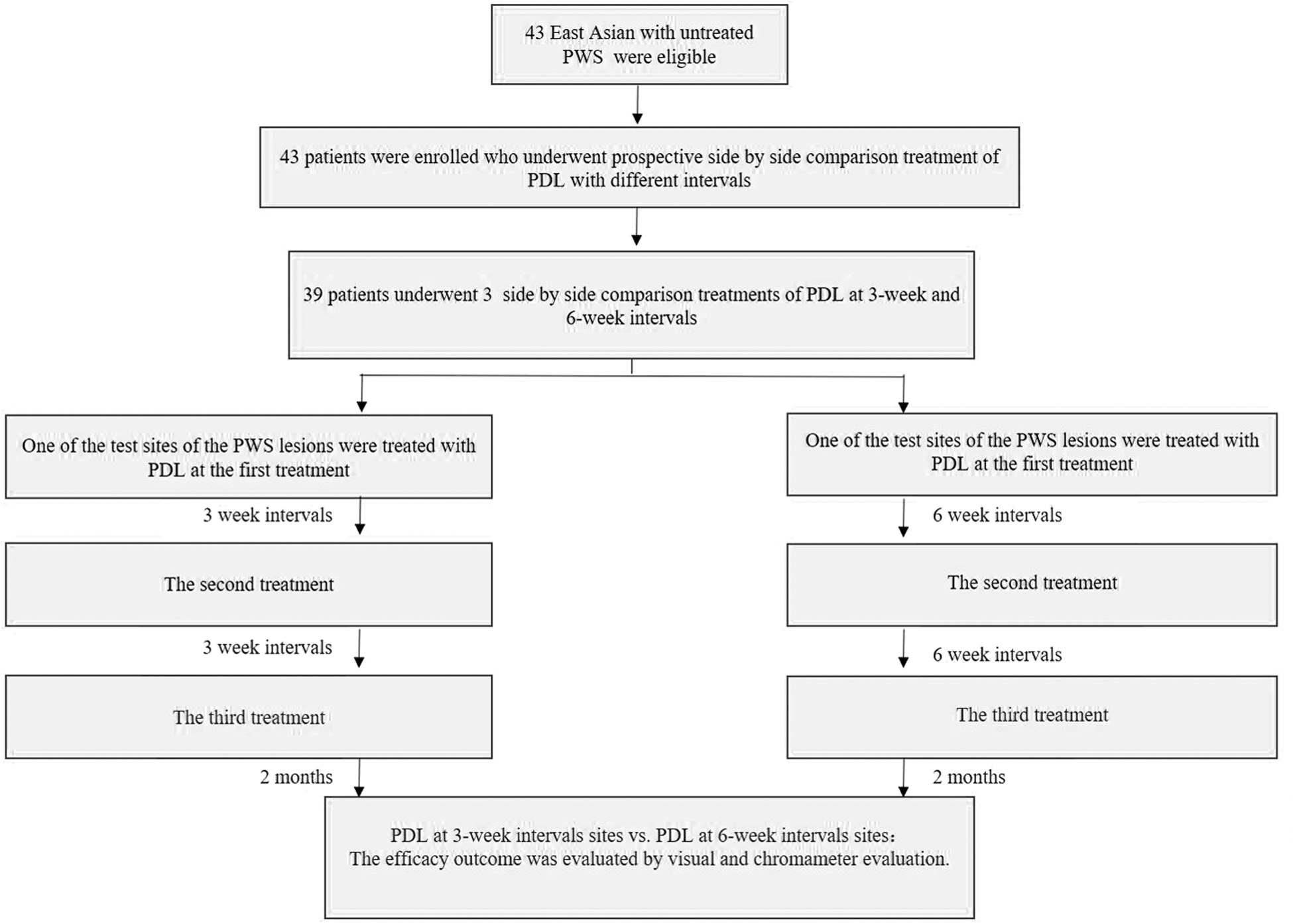
Participant enrollment, randomization, and analysis.
The efficacy outcome was compared and assessed by visual and chromameter evaluation before the treatment and 2 months after the final treatment. The chromameter optical equations used were those reported in previous studies, 12 whereas the complete blind visual evaluation was performed by four plastic surgeons, who had no knowledge of the laser treatment settings or outcomes. In addition, color improvement was graded using the following scale 13 : grade 1: no improvement, 0%; grade 2: mild improvement, 1–25%; grade 3: moderate improvement, 26–50%; grade 4: marked improvement, 51–75%; and grade 5: near total clearance, clearance >75%. The side effects and adverse reactions were followed up.
Laser
All patients were treated with a 595-nm Vbeam PDL (Candela Corp.), with cryogen spray cooling (40 ms of cooling with a 20 ms delay), radiant exposure of 9 J/cm2, 0.45 ms pulse duration, and 10 mm spot size. Overlapping was 20% for the last spot size.
Statistical analysis
Two test sites were analyzed and compared using GraphPad Prism 5 (GraphPad Software, Inc.) and SPSS19.0 (IBM Corp.), and data of the visual and chromameter assessment were compared by the Wilcoxon matched-pair signed-rank nonparametric tests. Spearman's rank correlation coefficients were used for the comparison of therapeutic outcomes from the visual and chromameter evaluation for the 3- and 6-week treatment interval sites. A p-value ≤0.05 suggested that the difference was statistically significant.
Results
Patient demographics
A total of 39 East Asian (21 females and 18 males) patients with untreated PWS were enrolled in this study. Patients' information is presented in Table 1. The age of the patients ranged from 2 months to 38 years (mean age 8 years). Fitzpatrick skin type III and type IV were identified in 14 (36%) and 25 (64%) patients, respectively. Thirty-one patients (79%) had PWS in the facial area, one patient had PWS on the trunk, and seven had PWS on the extremities. All patients were followed up to 2 months after three treatments finished.
Efficacy
Chromameter assessment (ΔE, blanching rate)
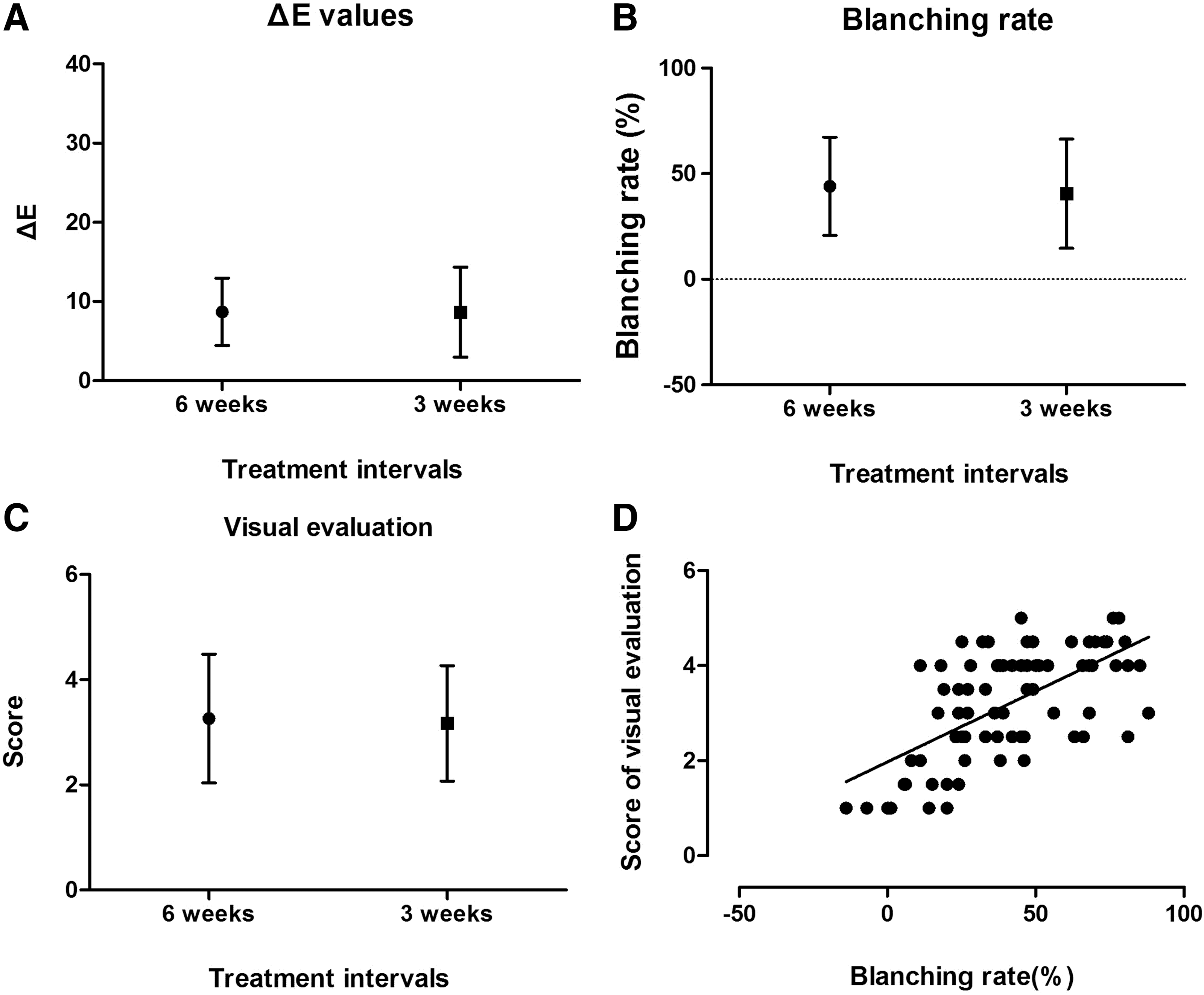
The average ΔE for the 3- and 6-week treatment interval sites was 8.66 ± 5.67 and 8.69 ± 4.25, respectively, (p > 0.05) (Fig. 3A). The blanching rate for the 3- and 6-week treatment interval sites was 40.27% ± 26.31% and 44.17% ± 23.35%, respectively, (p > 0.05) (Fig. 3B), which indicates that the PDL therapy at 3- and 6-week intervals has similar efficacy after three treatment sessions.
ΔE (color improvement) was measured before treatment and 2 months after treatment. The average ΔE for the 3- and 6-week treatment interval sites was 8.66 ± 5.67 and 8.69 ± 4.25, respectively (p > 0.05)
Visual assessment
Visual assessment at 2 months after the final treatment revealed that the average score for color improvement was 3.19 ± 1.09 and 3.28 ± 1.21 for the 3- and 6-week interval sites, respectively (p > 0.05) (Fig. 3C), which suggests that after final treatment, the efficacy of the response was similar for the 3- and 6-week intervals.
Comparison of visual and chromameter assessment
The Spearman's rank correlation coefficient for the comparison of therapeutic outcomes from the visual and chromameter evaluation was 0.608 (p < 0.001) (Fig. 3D), which indicates no difference between the visual and chromameter assessment for the PDL treatments at 3- and 6-week intervals.
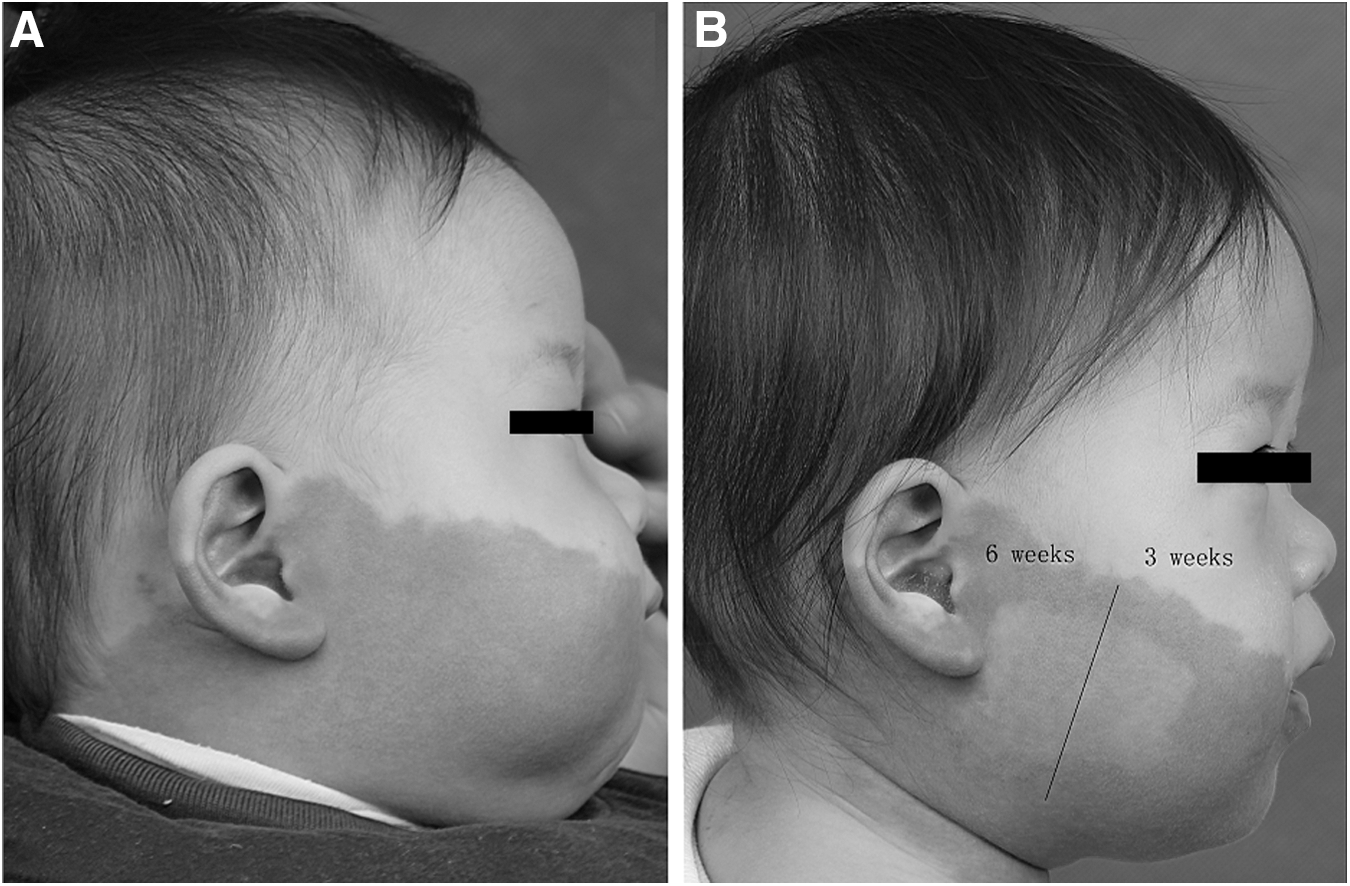
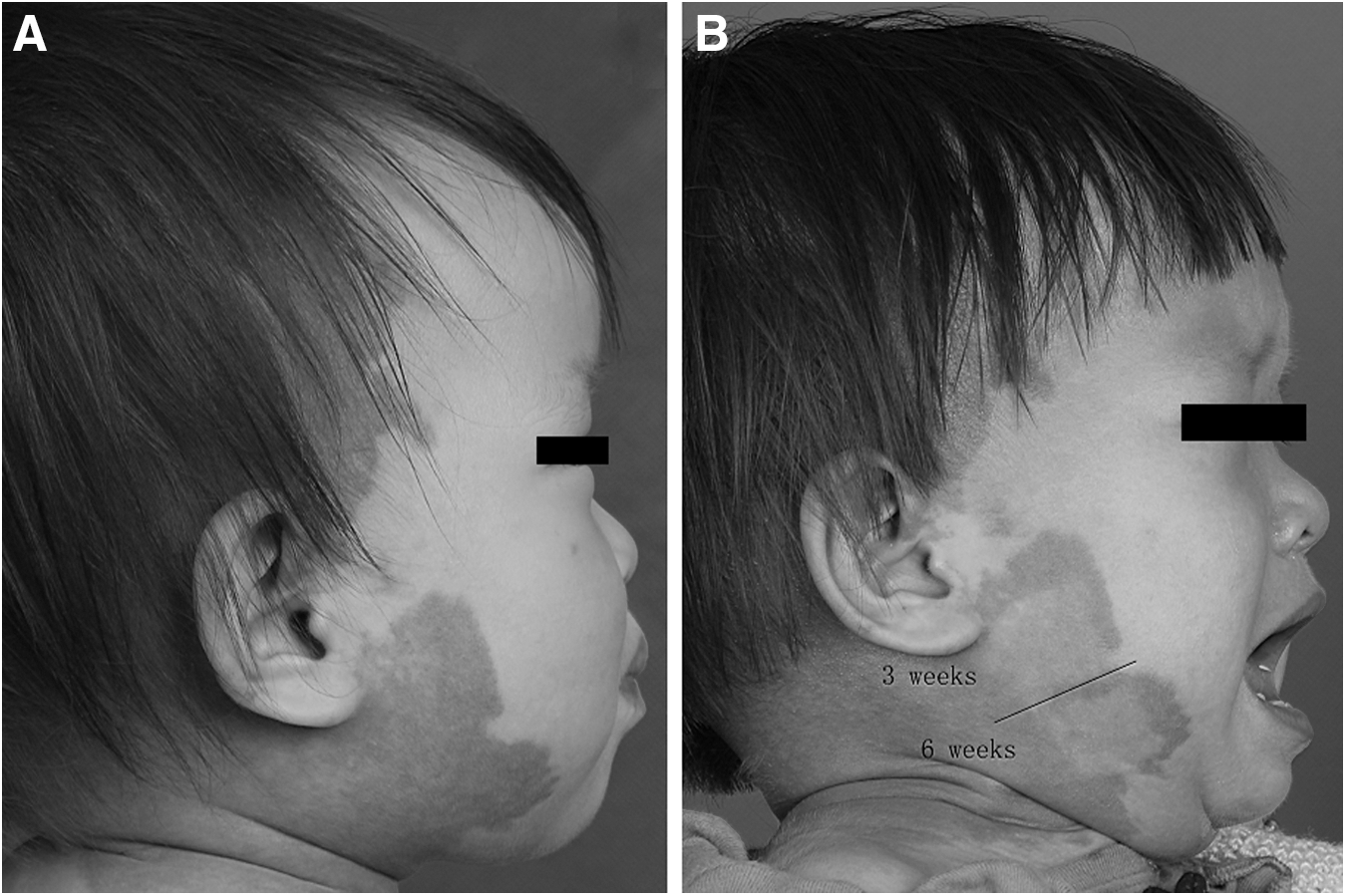
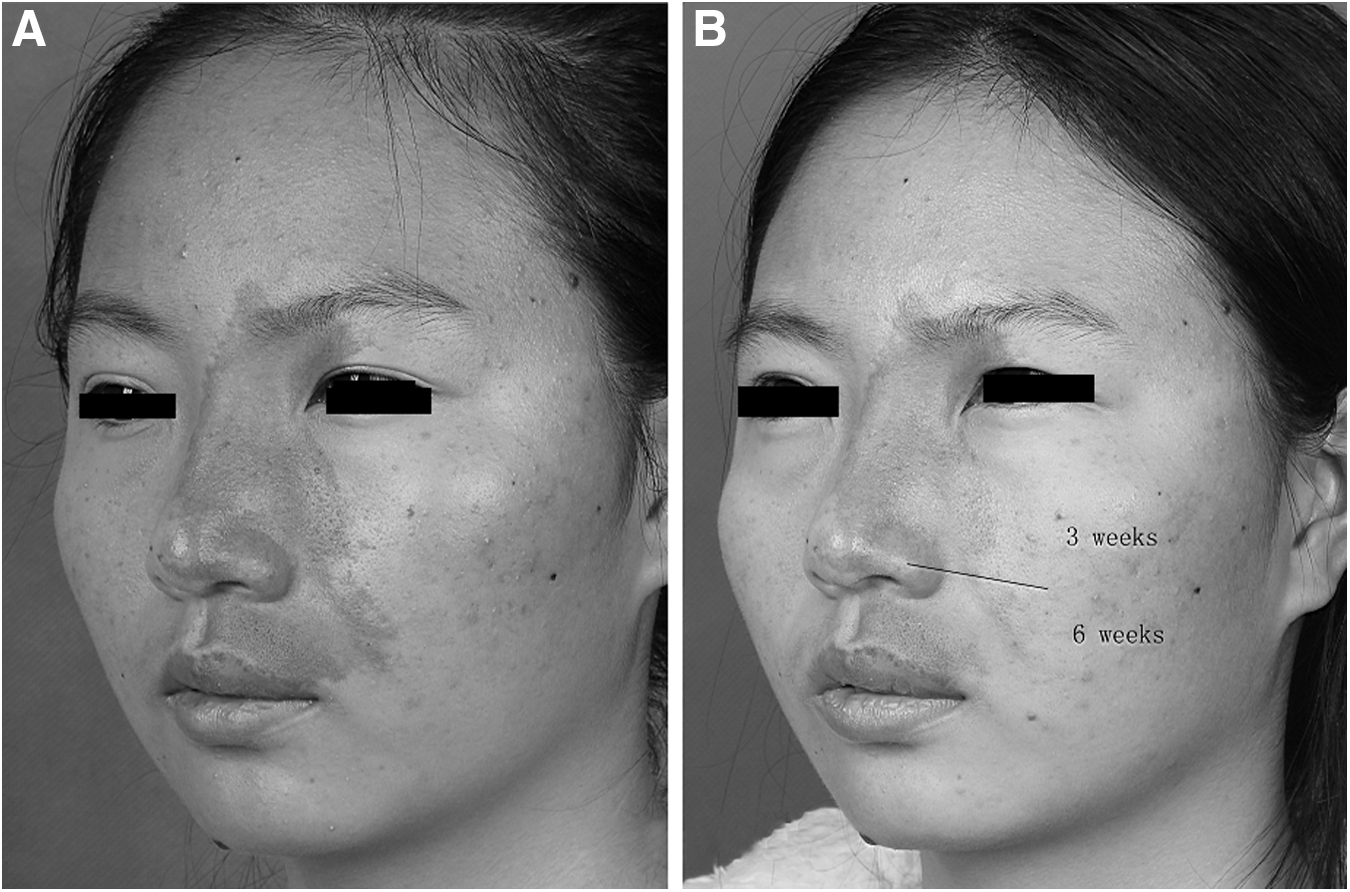
The results in Figs. 4 –8 showed the facial PWS treated by both PDL at 3- and 6-week intervals, before treatment, and 2 months after the final treatment.
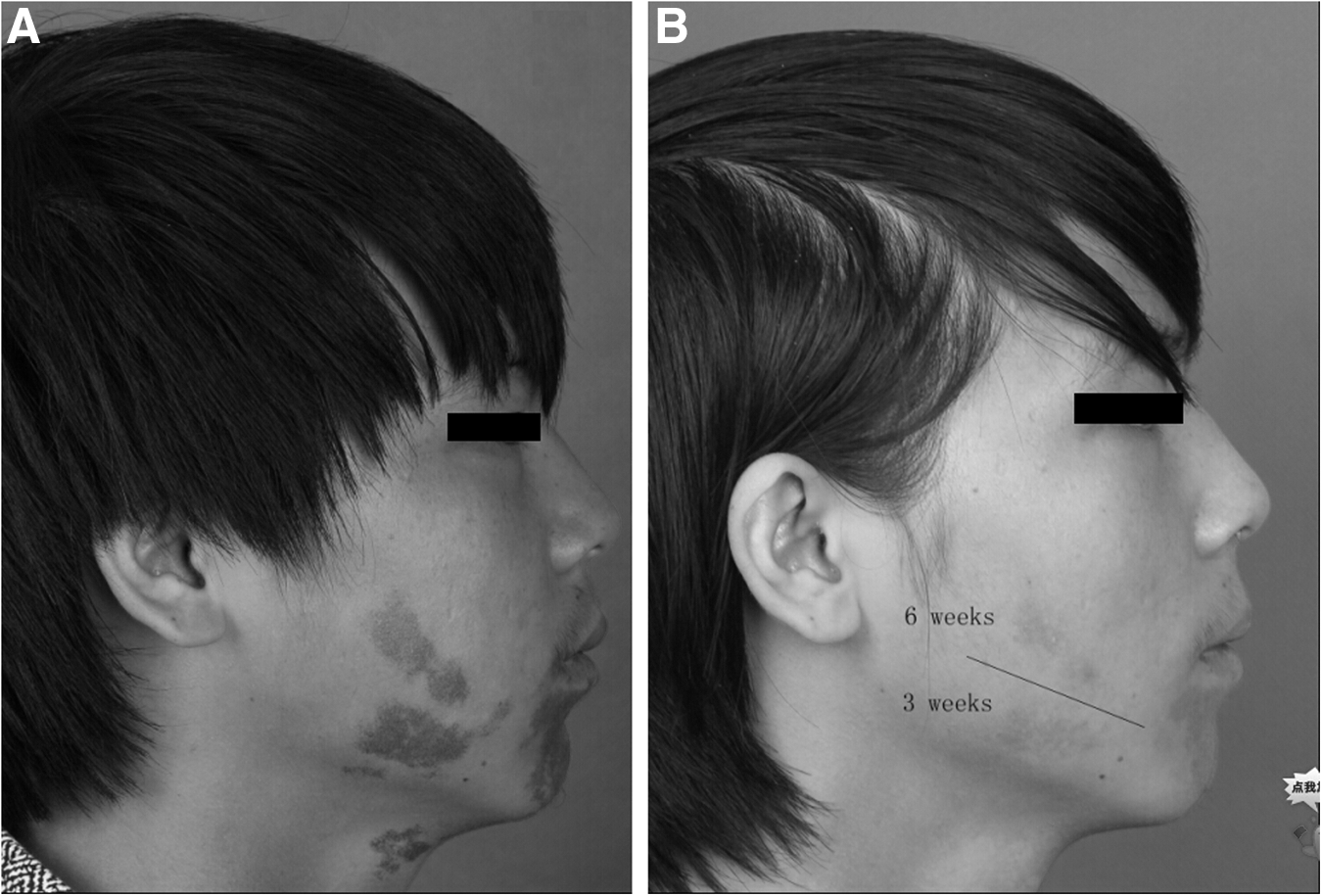
Patients with untreated facial PWS
Patients with untreated facial PWS

Patients with untreated facial PWS
Patients with untreated facial PWS
Patients with untreated facial PWS
Safety
The side effects included edema, erythema, and purpura. Additionally, short-term postinflammatory pigmentation change was present in two of the 39 patients, in both the 3- and 6-week interval groups. In addition, eight patients developed blisters in both interval sites. No permanence of pigmentation change, scarring, or infection were observed in both sites.
Discussion
PDL is the gold standard for the treatment of PWS. Usually, multiple treatments are necessary, with standard treatment intervals ranging from 6 to 12 weeks. 6 In recent years, the benefits of more frequent treatment intervals were proposed in previous studies. 6 –8 Tomson et al. compared the efficacy outcome from 16 patients with PWS, which were treated by PDL at 2- and 6-week intervals at adjacent sites in each patient and both sites of the PWS lesions underwent PDL treatment twice. They found that the 2-week interval treatment resulted in more significant reduction in color compared with the 6-week interval treatment (p < 0.01). 6 Moreover, Anolik et al. reported a retrospective chart review of 24 infants with facial PWS who underwent at least five treatments with the PDL at 2-, 3-, and 4-week intervals; the results showed that in the 2- and 3-week interval groups, the complete or near-complete clearance was seen in six of eight (75%) and seven of eight (87.5%) patients, respectively, compared with three of eight (37.5%) patients in the 4-week interval group, and no patient developed hypopigmentation, infection, or scarring. 7
Currently, the East Asian population around the world is estimated to be 1.6 billion, accounting for a quarter of the population of the world. According to the epidemiology, about 8 million newborns are diagnosed with
To explore whether PDL treatment at shorter intervals is safe and effective for East Asians with PWS, we treated 39 East Asian PWS patients with PDL at 3- and 6-week treatment intervals and compared the outcomes in each patient.
PWS consists of lesions with various diameter and vessel depth. Previous study considered that the residual blood vessels may cause postoperative vascular regeneration between individual laser treatments, which can influence the efficacy of PDL. Thus, it was also thought that shorter treatment intervals may damage these residual vessels before vascular regeneration. 14
The strategy of “treat early and treat often” has been widely proposed for the treatment of PWS, therefore, early intervention of PWS has potential advantage for the efficacy of the PDL treatments. 7,15 –20 Furthermore, the epidermis of patients is thinnest with least melanin and collagen in the first 6 months after birth, leading to the best penetration of the laser. Although our preliminary data showed similar color improvement for the two test sites, shorter intervals make it possible to maximize the number of sessions in the most responsive period.
In terms of safety, visual and chromameter assessment (subjective and objective evaluation) suggested that the treatment of PWS with PDL at 3-week interval is safe and well tolerated by East Asians with PWS. The test sites treated in 3-week intervals experienced no increase in side effects compared with the 6-week interval, which is largely attributed to the dynamic cooling device (DCD). 21 The cooling system is essential to reduce the side effects of the PDL treatment, such as skin damage caused by the heating of the epidermis during laser treatment, especially treated with PDL at shorter intervals. 22,23 Cryogen spray cooling, as a DCD, is a reliable cooling technique that can selectively cool down the perivascular tissue and epidermis while having minimal impact on the temperature of the underlying blood vessel. 24 With the aid of cryogen spray cooling, less side effects and pain would be experienced at higher fluences. 5,23,25 Thus, it is safe and effective for the PDL to treat at shorter intervals.
The limitations of this study include the following: this was a protocol including 3 treatments with PDL at 3- and 6-week intervals for each East Asian patient with PWS. Protocols with multiple treatments at different treatment intervals have no comparison in this study.
In conclusion, this study provided the preliminary data indicating that PDL treatments at 3-week intervals were well tolerated by East Asians with no significant difference in the blanching rate of PWS compared with the 6-week interval under the same number of times of laser treatment. For East Asians with PWS treated by PDL with cryogen spray cooling, we believe that a shorter treatment interval is safe and effective and could shorten the total course of treatment.
Footnotes
Acknowledgments
This study was supported by a grant from the Shanghai Health System Important Disease Joint Research Project (2013ZYJB0014).
Author Disclosure Statement
The authors declare that they have no conflicts of interest to disclose.