
Abstract
Introduction
P
Both the trauma and surgical procedure can cause changes in muscle activity, especially in the muscles responsible for the elevation of the mandible, such as the masseter, temporal, and medial pterygoid muscles, the impaired activity of which diminishes the ability to close or elevate the mandible, causing changes in the stomatognathic system. 4
Pain involving the soft and hard tissues of the face is among the most common complaints of victims of facial trauma and can range from mild sensitivity to extreme discomfort because of the trauma and/or surgical procedure. 3 Diminished blood flow and the buildup of metabolites in muscle tissue result in fatigue and pain. The visual analog scale is used in the study of pain because of its fast, easy administration, and low cost. 3,5 However, this assessment tool is often overlooked in randomized clinical trials involving mandibular fractures and most studies fail to describe the specific analgesics employed. 6
In photobiomodulation, reductions in pain and inflammation occur because of the resorption of exudates and the elimination of pain-causing substances. Interference occurs in the electrical message during the transmission of the stimulus, thereby avoiding the depolarization of the cell membrane. 7
Phototherapy is based on athermal reactions between light and tissue, leading to photochemical effects that act on cell organelles and chromophores, thereby inducing an increase in the synthesis of ATP, modifying ionic transport, and inhibiting the appearance of chemotactic factors, such as prostaglandins, in the early stages of inflammation as well as leading to an increase in local circulation and oxygen, with vasodilatation and a reduction in catabolites. 8 Moreover, increases occur in endorphins, dopamine, and serotonin, which are responsible for the increase in analgesia and a reduction in the action of nociceptors. 7 –10
Photobiomodulation can accelerate the healing process and significantly improve muscle regeneration. However, there is a lack of studies employing this therapeutic modality after the surgical treatment of mandibular fractures. Therefore, the aim of this study was to evaluate the effect of photobiomodulation on bite force, facial swelling, mandibular movements, and pain in patients having undergone surgical treatment for mandibular fractures.
Materials and Methods
This pilot study received approval from the Human Research Ethics Committee of University Nove de Julho (São Paulo, Brazil) No. 410.635/13. The study is registered with both the World Health Organization (Universal Trial Number U1111-1176-3098) and Brazilian Registry of Clinical Trials (REQ: 3843). The patients were treated for mandibular fracture at the Dr. Arthur Ribeiro de Saboya Municipal Hospital in São Paulo, Brazil, from January 2013 to January 2014.
The inclusion criteria were healthy patients (negative medical history) between 18 and 40 years old, male, with mandibular fractures, and the presence of at least two molars per hemiarch. Individuals with dentofacial anomalies, having undergone conservative treatment for mandibular fractures, pregnant or breastfeeding women, individuals subjected to radiotherapy of the head and neck, those with systemic or local infection (e.g., abscess), and those with injuries or radiolucent images associated with fractures were excluded. Patients with any complications during surgery (e.g., bleeding, surgical difficulty, and surgery >90 min) were also excluded. A researcher not involved in the study randomly allocated the patients to two groups using Microsoft Excel, 2013 version. Sequentially numbered opaque envelopes containing information on the type of phototherapy to be applied (active or sham) were used for the randomization process. The researcher responsible for phototherapy opened the envelope and performed the procedure written therein. The internal contents were revealed only after the statistical analysis had been performed. The patients were randomly allocated to either Group 1 (active laser) or Group 2 (sham laser—equipment switched off). For ethical reasons, both groups were prescribed corticoids. Figure 1 displays the flowchart of the study.
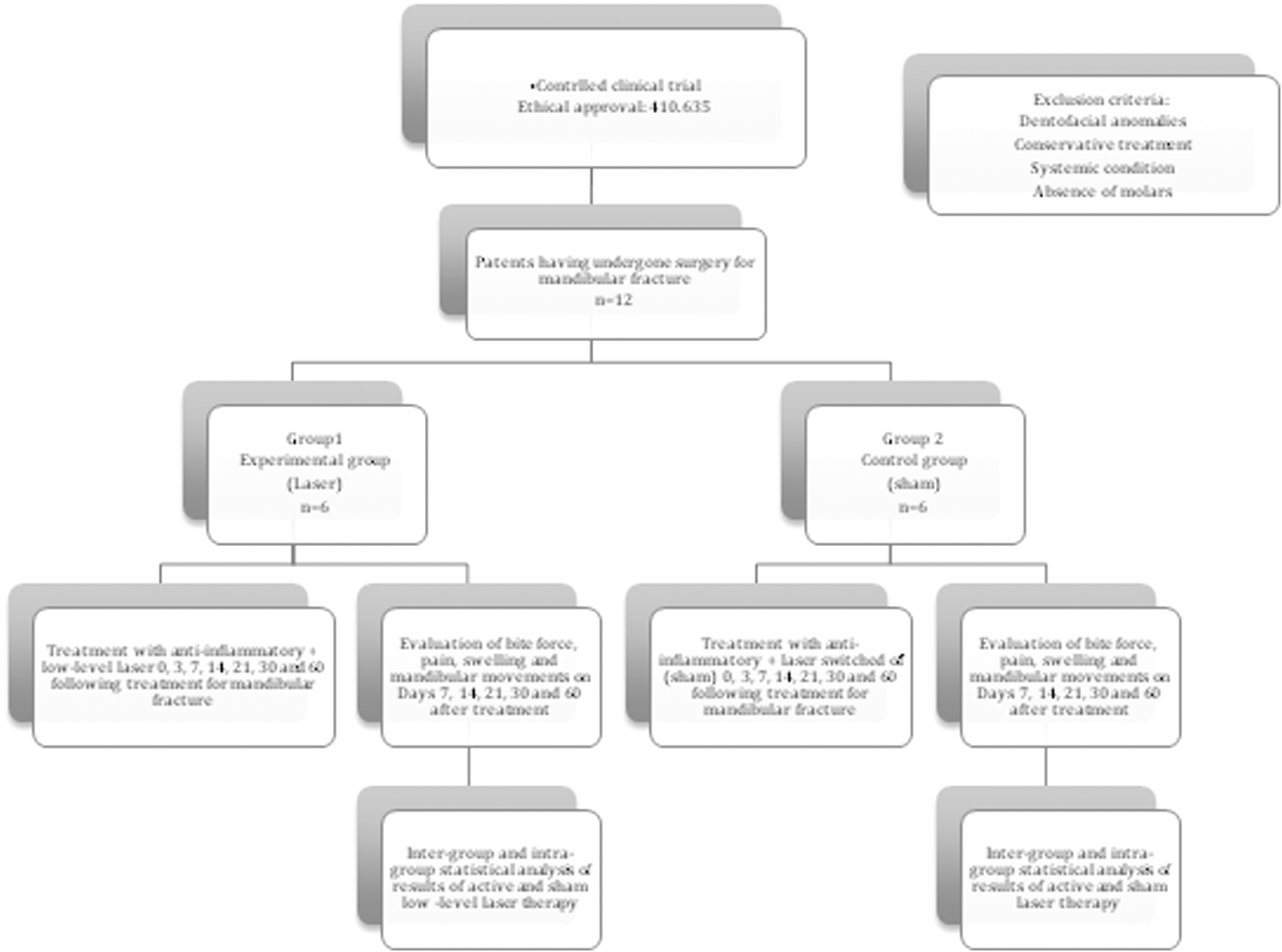
Flowchart of study.
A gallium-aluminum-arsenite (Ga-Al-As) device (Therapy XT®; DMC Equipamentos Ltda) was used for phototherapy. Three sessions were performed in the first week immediately after surgery and three per week after 7, 14, 30, and 60 days (total: 15 sessions). The device was previously calibrated with the parameters listed in Table 1. The active laser group received phototherapy in the region of incision and over the masseter (3 points: superior, medial and inferior) and temporal (anterior region) muscles, with 5 application points on each side, totaling 10 points bilaterally. For the sham laser group, the equipment was switched off without the patient's knowledge. 4,11
FWHM, full width at half maximum.
For the evaluation of the range of mandibular movements, maximum vertical movement from the incisal edge of the maxillary central incisor to the incisal edge of the mandibular central incisor was measured using digital calipers and corrected for overbite. Right and left movements were executed to record lateral excursion (distance between maxillary and mandibular midpoints). For patients with a deviated midline, the marking of the maxillary midline was added to the mandibular incisors and marked with a pencil, which was used as the reference for lateral excursion.
Protrusion was measured as the distance between the palatal face of the maxillary central incisors to the vestibular face of the mandibular incisors and added to the normal overjet of the individual. 12,13 These procedures were performed 7, 14, 21, 30, and 60 days after surgery. Edema was measured as the distances between the corner of the eye and gonion, between the tragus to the lip commissure and between the tragus and pogonium for each patient. 14 –16
Measures were performed using the same flexible ruler by the same researcher. At the end of each phototherapy session, the visual analog scale was used to evaluate the level of pain. This scale consists of a 10-cm line printed on the patient's chart. The patient was instructed to mark a point between 0 (no pain) and 10 (unbearable pain), indicating pain intensity 7, 14, 21, 30, and 60 days after surgery. Instructions on marking were always given by the same examiner. 17
A digital gnathodynamometer (model DMD, Kratos®; Equipamentos Industriais Ltda Cotia, São Paulo, Brazil) was used for the analysis of fatigue in the masticatory muscles. Readings were taken 7, 14, 21, and 30 days after surgery in the first molar region. The patient was asked to occlude the arches with maximum force of the molars on the side of the mandibular fracture and contralateral side. Six 5-sec readings were made (three on each side), alternating sides between readings, with a 1-min rest period between each reading. The means of the three readings on each side were calculated. 18
The Shapiro–Wilk test was used for the analysis of the results and normal distribution was demonstrated. Thus, the Student's t-test was used to determine intergroup differences and repeated measures analysis of variance was used to determine whether significant differences occurred at different times. The level of significance was set to 5% (α = 0.05).
Results
All patients were male (100%). Mean age was 34.5 years, 66.6% were dark skinned, and 33.4% were light skinned. Interpersonal aggression was the main etiology of the mandibular fractures. Addictions were detected in most cases: 58.3% of patients reported alcohol abuse and 25% reported the use of tobacco and illicit drugs. Only 16.7% declared having no addictions. All patients reported symptoms of pain and paresthesia after the trauma. Facial swelling, facial asymmetry, malocclusion, and trismus were found in all cases.
The body and angle of the mandible were the most affected anatomic regions. The most common fracture trace was unfavorable (58.4%) (muscle action displaced bone fragments). Four patients (33.3%) had favorable fractures (muscle action did not displace bone fragments). One patient (8.3%) had a comminuted fracture (multiple intercommunicating traces). Regarding the fixation system, titanium plates with the locking 2.0 mm system were used in 100% of cases. 2,3 The Risdon incision was the surgical access to the fracture region. Antibiotics and anti-inflammatory steroids were the medications of choice in all cases (100%). Analgesic therapy was employed in cases of pain.
A significant intergroup difference favoring the laser group was found regarding the improvement in protrusion (p > 0.05). In the intragroup analysis, the laser group demonstrated a systematic improvement over time, which was statistically significant beginning at 21 days (p = 0.0398), whereas the control group required 60 days to demonstrate a statistically significant improvement (p = 0.0004). These data are shown in Fig. 2. For right excursion, a significant intergroup difference favoring the laser group was found beginning at 14 days (0.0359). In the intragroup analysis, the control group required 21 days to achieve a significant difference in right excursion (p = 0.0148), whereas only 14 days were needed in the laser group (p = 0.0069).

Mandibular dynamics. LLLT, low‐level laser therapy.
For left excursion, the laser group demonstrated a systematic improvement over time, with a statistically significant difference beginning at 21 days (p = 0.011), whereas the control group remained constant (p = 0.8059). In the intergroup analysis, the laser group differed significantly from the control group only at 7 days (p = 0.0474). A systematic but nonsignificant difference between groups was found with regard to maximum voluntary vertical mandibular movement. In the intragroup analysis, maximum vertical movement was significantly different beginning at 21 days in the control group (p = 0.0072), but the laser group required 30 days to achieve a significant difference (p = 0.0257).
A significant difference between groups was found with regard to bite force on the right side at 60 days (p = 0.0146). The laser group demonstrated a significant increase in bite force at 60 days (p = 0.0002). The control group demonstrated significantly less improvement in comparison with the laser group at 14 days (p < 0.0001). No significant intergroup differences were found on the left side at any evaluation time (p > 0.05). In the intragroup analysis, the laser group demonstrated a significant increase in bite force at 30 days (p = 0.0033), whereas the control group required 60 days to demonstrate a significant improvement (p = 0.0382).
The two groups were similar with regard to edema, but significant differences were found in the intragroup analyses. The effect size at 7 days was 0.283 (medium) for the right side and 0.015 (small) for the left side, which suggests that analyzing larger sample would lead to similar conclusions. These data are shown in Fig. 3.
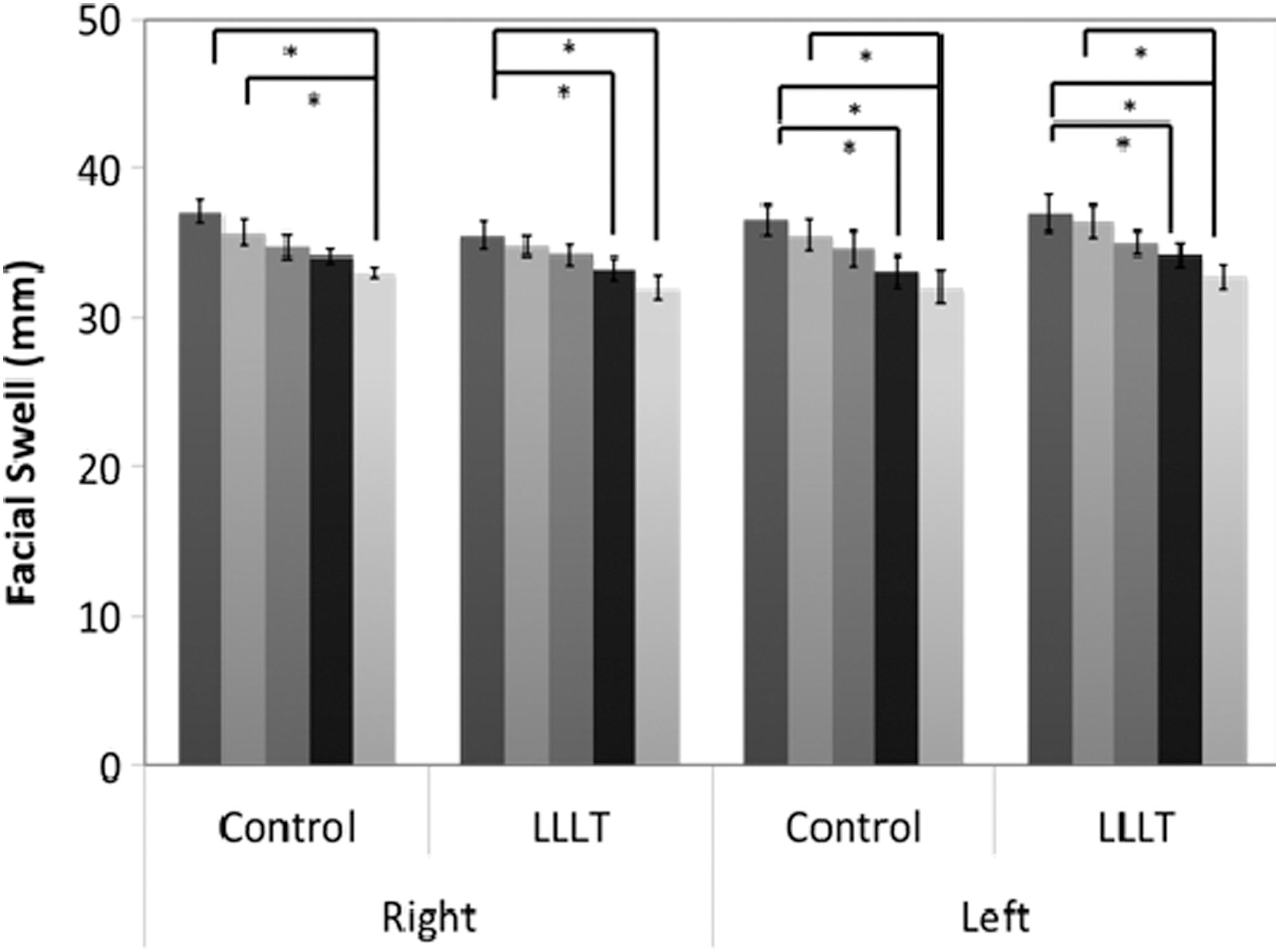
Facial swelling. *Means p < 0.05. LLLT, low‐level laser therapy.
Analyzing the reduction in pain, a systematic but nonsignificant difference was found in the comparison of the two groups. The perception of pain was statistically different in the control group at 21 days (p = 0.0293), whereas the laser group required 30 days to demonstrate a statistically significant difference (p = 0.0435). These data are shown in Fig. 4.

Perception of pain. Measured in VAS. VAS, visual analogue scale.
Discussion
In this study, all participants were male and mean age was 34.5 ± 7 years. Thus, all were in the active period of life. Among the clinical signs, facial swelling, facial asymmetry, malocclusion, trismus, and tooth loss were observed. This period of life coincides with the majority of cases of trauma stemming from traffic accidents, physical aggression, and firearm wounds, as this age group is both more exposed socially and economically active in society. The findings are in agreement with data reported in previous studies, which report the body of the mandible to be the most frequently affected region. 19,20 There was a clear improvement in inflammation and mandibular dynamics in the group treated with phototherapy, indicating a significant earlier gain in the functional return of mandibular motility in comparison with the sham laser group.
The release of vasoactive amines, such as histamine and serotonin, occurs in an inflammatory process. These substances cause the vasodilatation of arterioles and increase venous permeability. To prevent swelling, anti-inflammatory therapies should be performed as early as possible. 17 Once the inflammatory infiltrate is present in extracellular matrix, edema is established. Therefore, early preemptive treatment minimizes the occurrence of edema. 21,22 In this study, the patients began treatment several hours after the trauma and it was, therefore, not possible to intervene preemptively to prevent edema. Thus, the results for this variable were not as substantial. In previous studies, the group that received light therapy demonstrated less swelling than the control group. 14 –16
A significant reduction in the perception of postoperative pain was found in patients treated with phototherapy in comparison with the sham laser group. The first evaluation of pain occurred after three phototherapy sessions in the immediate postoperative period (3–5 days after surgery). Some authors state that the reduction in postoperative pain because of phototherapy 2 and 7 days after the extraction of impacted third molars indicates that a single session of phototherapy does not have a significant effect on this outcome. 23 Different studies describe the increase in the production of ATP as one of the effects of phototherapy and the consequent increase in cell mitosis, which uses light energy for metabolic exchanges, restoring neuronal membranes, and diminishing the transmission of stimuli, thereby diminishing pain.
Phototherapy maintains the membrane potential by avoiding its depolarization because of the increase in the synthesis of ATP. This energy is necessary for the expulsion of Na+ through the sodium and potassium pumping mechanism, which balances the potential of the cell membrane and hinders the transmission of the local pain stimulus. Besides these analgesic effects, the action of phototherapy can be explained by the increase in the synthesis of bradykinin, resulting in a reduction in the activity of afferent C fibers and a change in the pain threshold. Phototherapy inhibits cyclooxygenase and increases the production of B-endorphins, which modulates both the sensation of and response to pain.34–36
The laser group demonstrated a greater improvement and effective gain in bite force on the right side at 60 days in comparison with the control group, which maintained a small gain throughout the evaluation times. The laser group also demonstrated a significantly greater gain in bite force on the left side at 30 days in comparison with the control group. This gain in bite force may be explained by the antiswelling effect of phototherapy, with greater drainage of plasma and lactate from the inflamed region, thereby facilitating the normal physiological functions of the masticatory muscles. 26 –31
Phototherapy modulates local swelling by stimulating microcirculation, which facilitates the drainage of plasma and has fibrinolytic action in the coagulated area of the extravasated plasma. 23 –25 It should be stressed that no isolated effect of phototherapy was found, as all properties of this type of therapy (analgesic, anti-inflammatory, antiswelling, and biostimulating) act jointly on the treated area, thereby enabling the early return of stomatognathic functions as well as the performance of activities of daily living and social activities. However, further studies involving phototherapy, especially controlled clinical trials, are needed.
Conclusions and Summary
Photobiomodulation improves mandibular dynamics, pain, and bite force in patients after surgery for mandibular fracture.
Footnotes
Acknowledgments
The authors gratefully thank Nove de Julho University and Dr. Arthur Ribeiro de Saboya Municipal Hospital for their technological support.
Author Disclosure Statement
No competing financial interests exist.