
Abstract
Introduction
T
Image visualization of oral tissue autofluorescence (or endogenous fluorescence) is due to the presence of molecules. These molecules are called fluorophores and are related to cellular metabolism and tissue structure. Some fluorophore examples are the reduced form of nicotinamide adenine dinucleotide (NADH), flavin adenine dinucleotide (FAD), elastin, collagen, and keratin. 2,3,5 However, autofluorescence is influenced by absorption, reflection, refraction, and scattering, both during emission and excitation modify the penetration depth of light in the tissue, intensity, and spectral distribution of the detected fluorescence. 2,3
Thus, applying the basic knowledge of biophotonics about oral tissue autofluorescence may lead to new clinical applications for the use of technology and not only topics related to oral cancer. Consequently, in this case, we present the location of an intraosseous firearm projectile in the maxillary tuberosity using wide-field optical fluorescence.
Materials and Methods
The used protocol involved the accomplishment of oral conventional clinical examination under visible light complemented by the clinical approach of wide-field optical fluorescence, obtaining images related to these examinations.
Intraoral camera model DP6 Scope® (RF System Lab., Almere, Netherlands) coupled to a computer was used to get the images from the regular oral clinical examination under visible light. The Evince® device (MMOptics, São Carlos, Brazil) was used to carry out the wide-field optical fluorescence complimentary examination. The device has a high-power light-emitting diode with emission centered at (400 ± 10) nm, maximum irradiance of (0.040 ± 0.008) W/cm2, and an optical filter that allows the visualization of the fluorescence, whereas a digital microscope model Deluxe Handheld Digital Microscope® (Celestron LLC, Torrance, CA) was used coupled to Evince and a computer to obtain the optical fluorescence imaging.
Case Report
The 58-year-old female patient, Caucasian, attended the dental appointment for preventive purposes without any complaint or oral symptomatology. In the anamnesis, she reported a recent history of treatment for thyroid cancer, not reporting any general or systemic symptomatology, but mentioning only a medical recommendation, in this sense, that would avoid performing radiography.
Regular oral clinical examination
The images of Fig. 1 refer to the oral mucosa of the maxillary tuberosity region on the left side where both in the buccal (Fig. 1A) and occlusal (Fig. 1B) and in the palatal views (Fig. 1C) no tissue abnormality is observed. A pale pink color is visualized, which is the standard pattern of the oral mucosa.

Aspect under visible light of the oral mucosa of the left maxillary tuberosity in
Wide-field optical fluorescence complimentary examination
Under fluorescence, a darkened, circular, uniform, and unilateral image was observed in the oral mucosa region of the left maxillary tuberosity. The darkened image was about 5 mm in diameter and was located about 8 mm posteriorly to the distal of left upper second molar (Fig. 2). The darkened aspect of the oral mucosa under fluorescence, which is due to the loss of fluorescence, can be observed both in a palatal view (Fig. 2A) and a vision with an occlusal tendency (Fig. 2B).
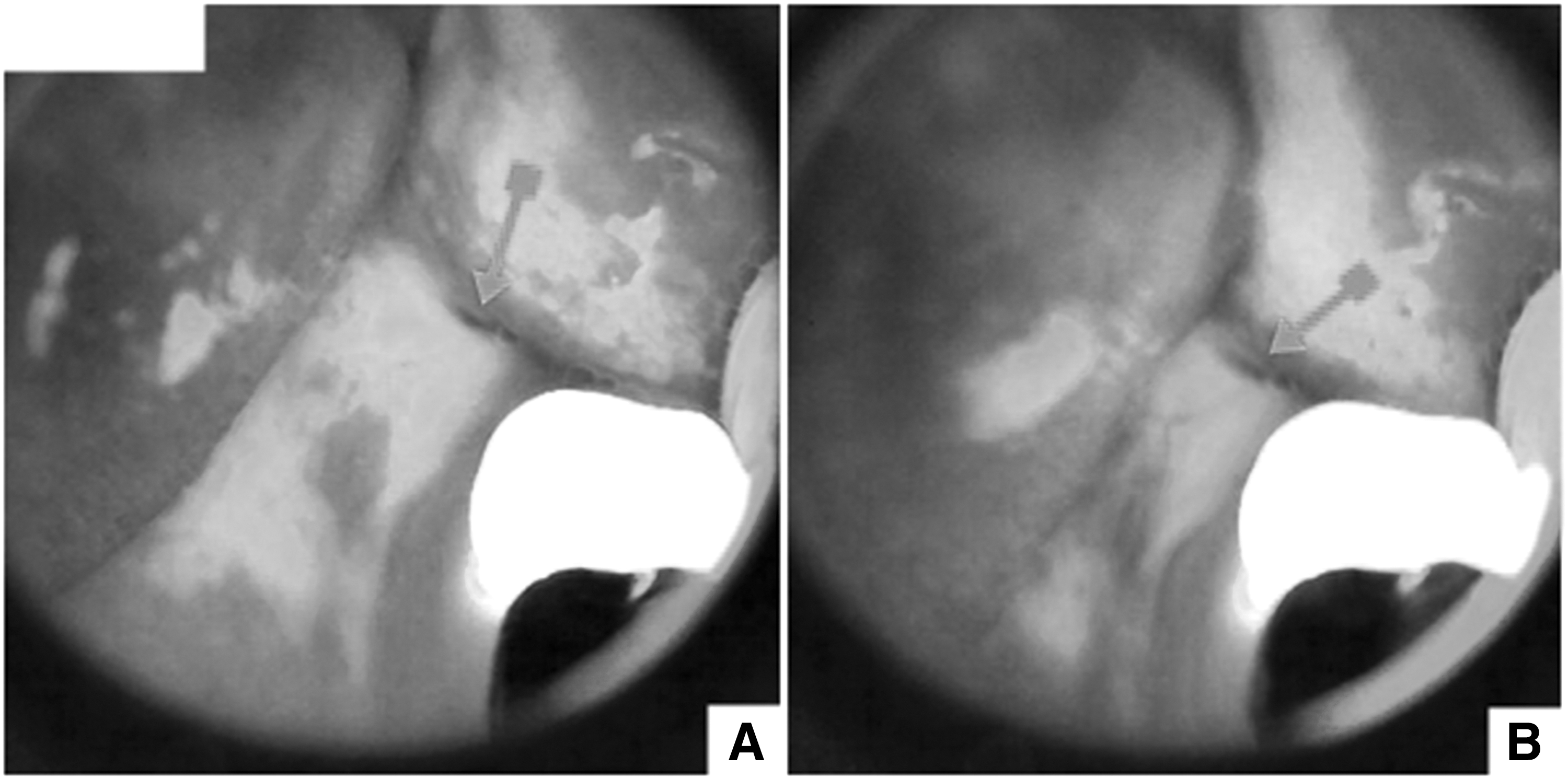
Aspect under wide-field optical fluorescence of the oral mucosa of the left maxillary tuberosity in the
Due to this fluorescence image, the patient was questioned about a fact related to that region, such as surgery or extraction of teeth, and the answer was negative. Thus, the patient was informed about the need for a local radiograph for a correct diagnosis.
Radiographic examination
Periapical radiography showed the presence of an intraosseous firearm projectile in the left maxillary tuberosity (Fig. 3). The approximate dimensions of the projectile are 5 mm in diameter and 7 mm in height. The projectile is lodged, about 8 mm posterior to the left upper second molar and, with its most superficial part, about 4 mm below the most superficial layer of the epithelium.
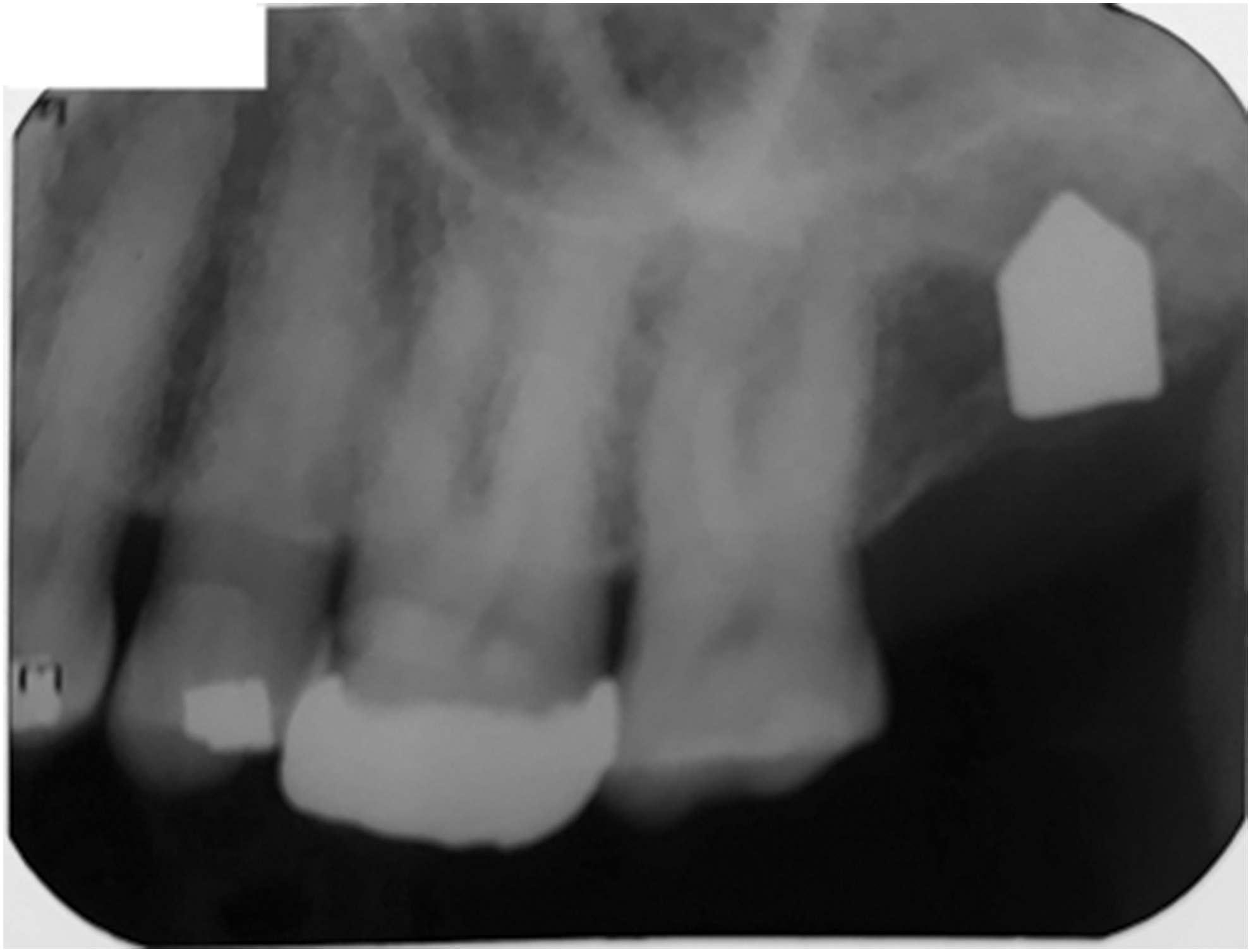
Periapical radiographic image of the firearm projectile lodged in the left maxillary tuberosity.
Results
The images obtained by wide-field optical fluorescence are showed in Fig. 2. Moreover, periapical radiography (Fig. 3) showed compatibility on the diameter of the projectile (about 5 mm) and the location in the anteroposterior direction of the projectile about the distal face of the left upper second molar which was about 8 mm. Otherwise, the presence of the firearm projectile was imperceptible by standard clinical examination under visible light (Fig. 1).
There is a discrepancy between the depth at which the most superficial part of the projectile lies in relation to the most superficial layer of the epithelium, which is about 4 mm, and the depth of tissue penetration of the light at the wavelength of 400 ± 10 nm, cited in literature, 3 which is about 0.5 mm. This discrepancy implies the need for some component of the projectile being released, reaching the most superficial tissue layers to absorb light, producing the loss of fluorescence, and consequently the dark appearance of the image (Fig. 4).
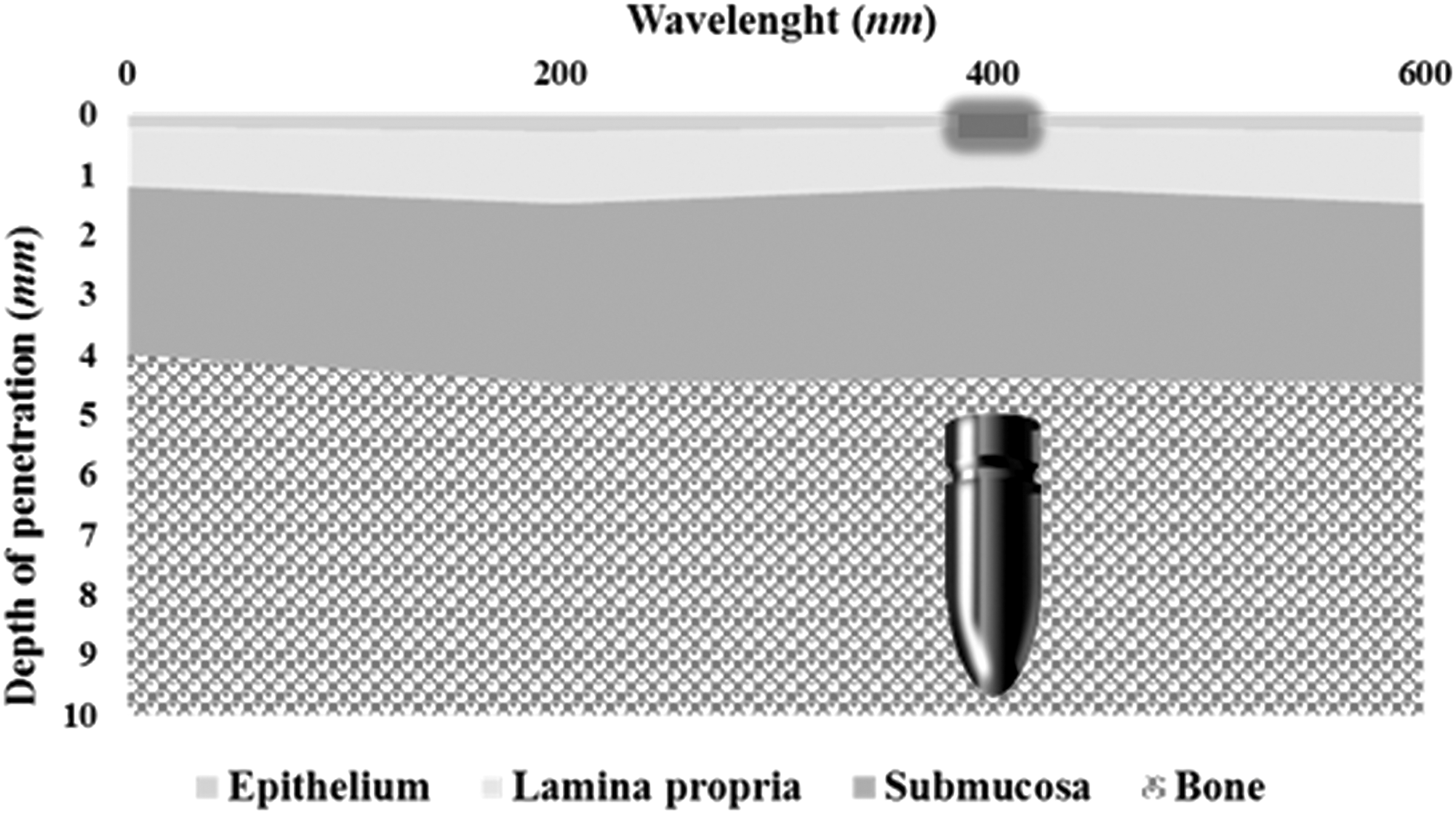
Illustration of the penetration depth of violet light (400 nm) comparing with the depth where the projectile is lodged.
The patient was informed of the presence of the projectile of firearm lodged in her maxillary tuberosity; she reported a firearm accident that occurred 46 years ago. The medical surgeon of head and neck who accompanied the patient decided not to remove the projectile because of the time elapsed since the accident reported by the patient without any intercurrence and because the patient did not present any clinical evidence or systemic symptoms related specifically to a possible systemic lead poisoning (saturnism or plumbism). Thus, the patient will maintain medical follow-up.
Discussion
In this case, in a routine medical appointment, with the use of wide-field optical fluorescence, a darkened image was observed unilaterally in the mucosal region of the left maxillary tuberosity. The appearance of a dark image in the area is considered outside the normal pattern and, therefore, indicates that something is happening in the area and should be investigated. Thus, as under visible light, the appearance was normal; only a periapical radiograph of the area was used, in which the presence of the firearm projectile, previously located by the fluorescence, was verified. The use of wide-field optical fluorescence allowed, in this case, an examination of the entire oral cavity, fast, painless, noninvasive, and with real-time results. 6 In addition, wide-field optical fluorescence is a safe technique for the patient by not using ionizing radiation.
The localization of the projectile by fluorescence is quite different from the traditional approach to a firearm projectile injury. The traditional approach to locating a firearm projectile, as cited by Sonkhya et al., using the radiographic image and computed tomography, is that the use of magnetic resonance imaging is not routine because of the risk of dislocation of the ferromagnetic body inside the adjacent tissue worsening the injury. 7 The previous location of the region of the firearm projectile by optical fluorescence, in this case, avoided the use of panoramic radiography or computed tomography. Use of a single periapical radiograph has the advantage of reducing the dose of ionizing radiation, as explained by Okano and Sur, compared to the traditional approach using panoramic radiography and computed tomography. 8 The periapical radiograph, utilized in this case, according to Bahlis et al., allows better results than computed tomography and panoramic radiography for vertical measurements (depth). 9 In turn, Sonick et al., demonstrated a degree of distortion for periapical radiographs averaged 14%, with a mean discrepancy of 1.9 mm at the location of the mandibular canal. 10 Based on this, in the case of a possible removal of the projectile, the radiographic distortion would not have significance for correct positioning of the surgical flap. Further, wide-field optical fluorescence would allow the marking of the exact location of the projectile in real time, trans-surgically, allowing a less invasive surgical flap, which could result in less trauma and, consequently, a better postoperative.
What makes this case extremely rare is based on the depth of penetration of light into tissues at the wavelength of 400 nm, which according to Keereweer et al. 3 is about 0.5 mm. As the projectile is lodged at least 4 mm below the surface layer of the mucosa, a discrepancy is established on the depth of penetration in the tissue of violet light (0.5 mm). Therefore, it is necessary that some component of the projectile be reaching the superficial layers of the oral mucosa to absorb the light emitted by the device causing the darkened appearance visualized in the area. This understanding is supported by both, Keereweer et al. and Lane et al., which shows the influence of absorption and scattering by the tissue components in the intensity of the detected fluorescence, in this case, producing a darkening of the visualized image in the region of the projectile. 2,3
The understanding of the histopathology of lead, the principal component of the projectile, explains the loss of fluorescence and the consequent visualization of the darkened image in the oral mucosa where the projectile is lodged. Thus, according to Greenberg, there may be a slow process of loss of lead ions from the surface of the projectile, which would be solubilized by the interstitial fluid and carried to other parts of the body through the circulation. 11 In turn, the presence of chronic inflammatory cells and lead-laden macrophages in the proximal stroma where the projectile is lodged is shown by Viegas and Calhoun. 12 Accordingly, Linden et al., suggest phagocytosis of lead in the form of lead dioxide by macrophages. 13 Therefore, the lead was being loaded into the more superficial layers of the oral mucosa, either by interstitial fluid or macrophages, where it would produce the absorption of fluorescence that would result in the visualization of the image darkened by the loss of fluorescence.
In conclusion, it is evidenced that the use of wide-field optical fluorescence, within a clinical routine, can provide relevant images and data, in a noninvasive way, painless, with immediate result and, without the use of ionizing radiation, enabling an efficient oral diagnosis. In this article, we report the location of a firearm projectile, intraosseous, in the maxillary tuberosity, using wide-field optical fluorescence.
Ethical approval
This study has been approved by the Ethics Committee of Federal University of São João del-Rei, Campus Centro-Oeste Dona Lindu (Approval number: 1.756.617).
Footnotes
Acknowledgments
The authors thank FAPESP (São Paulo Research Foundation) (grant number: 2013/07276-1; 2014/50857-8), CNPQ, and CAPES for financial support and fellowships.
Author Disclosure Statement
No competing financial interests exist.