
Abstract
Introduction
I
Some methods have been suggested to address these problems, 2 –7 mostly by thermodebonding. However, some studies have not considered pulp damage during thermodebonding, and some were dangerous because they performed the debond while the resin was melting. Tsuruoka et al. 8 and Ryu et al. 9 reported that the bond strength of a chemical cure-type orthodontic adhesive (Orthomite SuperBond; Sun Medical, Moriyama, Japan) containing 40% microcapsules, which expanded 70-fold at 80°C, decreased by 0.2- to 0.3-fold on heating the bonded bracket, and temperature increase in the pulp chamber was <5.5°C, which is a critical point for pulp damage. However, an electric heater at 300°C was used to heat the adhesive containing the microcapsules, which is not safe because of the risk of burning oral soft tissues.
Various laser products have become widely used by dentists for purposes such as a surgical knife for soft and hard tissues, caries removal, pain relief, and bioactivation of tissues, 10 and studies regarding bracket debonding using CO2 lasers have also been reported. 11 –14 The CO2 laser has the heating effects of the irradiated region and is easy to be absorbed to ceramic bracket surfaces due to wavelength. 11,13 Therefore, we chose CO2 laser for bracket heating. In a previous study using a chemical cure-type orthodontic adhesive containing heat-expandable microcapsules and CO2 laser irradiation instead of a heater, bond strength of the bracket significantly reduced with laser irradiation. 15
Light cure-type orthodontic adhesives have recently been used widely instead of the chemical cure type because they can be cured immediately by light irradiation after bracket positioning, 16 enabling more accurate positioning and a shorter bonding time. Thus, the aim of this study was to make it easier to remove ceramic brackets by using a light-cured orthodontic adhesive containing heat-expandable microcapsules and CO2 laser irradiation for heating to reduce debonding time and fractures of the tooth enamel and ceramic brackets.
Materials and Methods
Preparation of a bonding agent containing thermally expandable microcapsules
A proportion (0, 10, 20, 25, and 30 wt%) of heat-expandable microcapsules (Matsumoto Microsphere F-36D; Matsumoto Yushi-Seiyaku, Osaka, Japan), which expand by 70-fold on heating to 80°C, was mixed into a commercially available orthodontic bonding agent (Transbond XT primer; 3M Unitek, Monrovia, CA) in a darkroom environment. Thermal expansion microcapsules contain some expanding agents, which are volatile organic compounds such as isobutene, pentane, petroleum ether, hexane, heptane, low-boiling-point halogenated hydrocarbon solvent, or methylsilane. The capsules are covered with a membrane polymer that consists of thermoplastic resin composed of copolymers such as vinylidene chloride, acrylic acid ester, or methacrylic acid ester. 8
Preparation of bovine tooth specimens and bracket bonding
In total, 60 freshly extracted bovine permanent mandibular incisors were bought from a slaughterhouse. The criteria for tooth selection were intact labial enamel with no cracks and the absence of caries. The teeth were divided randomly into 10 groups of 6 specimens each (the groups of irradiation and no irradiation in 0, 10, 20, 25, and 30 wt% respectively), corresponding to the number of variables tested.
Soft tissues were removed from the teeth with surgical knife. After separating the crown from the root with a diamond band saw (Proxxon Mini band saw; Kiso Power Tool, Osaka, Japan), the pulp was extirpated with dental tweezers and the crown was stored in distilled water until further use. Then, the crown was embedded in self-curing acrylic resin (Tray Resin; Shofu, Kyoto, Japan) to facilitate its placement in the testing machine. The labial surface of each crown was flattened to facilitate the application of shearing force with a trimmer (Model trimmer; Morita, Tokyo, Japan) and polished with waterproof #400 and #600 silicon-carbide papers. The enamel surfaces were rinsed with water and dried with an oil-free air stream.
One operator bonded 60 zirconium ceramic for maxillary central incisor brackets (COBY, Biodent, Tokyo, Japan; the base area was 12.4 mm2) with a 0.018-inch slot as follows: etching was performed to the enamel surface with 35% orthophosphoric acid for 30 sec, followed by rinsing and drying, according to the manufacturer's protocol. Then, bonding agent containing microcapsules (0–30 wt%) was applied to the enamel surface, and a ceramic bracket base with applied adhesive resin composite paste (Transbond XT paste; 3M Unitek) was placed on the enamel surface. After excess paste was carefully removed with a dental probe, each mesial and distal side of the bracket base was exposed to curing light (Optilux 501; Demetron/Kerr) for 10 sec at a 45° irradiation angle. Then, the specimens were immersed in distilled water at 37°C for 24 h.
Measurement of the bracket base temperature after laser irradiation
It was evaluated whether the bracket base temperatures exceeded 80°C after CO2 laser irradiation (Opelaser Pro; Yoshida, Tokyo, Japan). The tip of the CO2 laser head contacted the labial surface of the bracket and the increase in the bracket base temperature was measured using a K-type thermocouple sensor head (0.5-mm diameter; Okazaki Manufacturing, Kobe, Japan) in contact with the bracket base under various irradiation conditions (irradiation output of 5 or 7 W, irradiation mode: continuous mode, irradiation time: 3–6 sec, with or without air cooling during laser irradiation, laser spot size: 0.15 mm diameter, focus point: 3.0 mm from the tip of the laser head, and wavelength: 10.6 μm). The CO2 laser was applied to one point at the center of the bracket surface.
Measurement of temperature increase in the pulp chamber
The temperature increase in the pulp chamber after CO2 laser irradiation under various conditions was evaluated as described for the bracket base temperature. Five fresh human first premolars that had been extracted in orthodontic treatment were used. The protocol for this experiment was reviewed and approved by the Nihon University School of Dentistry Ethics Committee (EP16D008). Brackets were bonded to the teeth with bonding agent containing 25 wt% microcapsules and adhesive paste. Each tooth was drilled with an air turbine at the lingual cemento-enamel junction toward the labial bonded bracket. The 0.5-mm-diameter sensor head of a K-type thermocouple was placed in contact with the inner surface of the pulpal wall, facing the labial surface where the bracket was bonded. The average distance from the labial surface to the pulpal wall was 1.9 ± 0.5 mm. The temperature of the tooth pulp inside wall was measured after irradiation by contacting the bracket with the laser head at room temperature (23.0°C ± 1.0°C); measurements were performed five times.
Measurement of bond strength under shear
Sixty brackets, bonded with paste and bonding agent containing microcapsule contents of 0, 10, 20, 25, and 30 wt%, were irradiated with the CO2 laser. Shear bond strength tests were performed at 10 min after irradiation. Specimens were secured in the lower jaw of a universal testing machine (5567; Instron, Norwood, MA) so that the bonded surface of the specimen was parallel to the direction of the shear force. The specimens were stressed in an occlusogingival direction at a cross-head speed of 1.0 mm/min. The maximum loading at bond failure was determined as the bond strength.
Assessment of residual adhesive
After shear bond strength measurement, each specimen was examined under an optical microscope (SZ-3003; As One, Osaka, Japan) at 15 × magnification to identify the fracture pattern of the bonded surface. The residual adhesive on each tooth was assessed using the adhesive remnant index (ARI) as follows: 0, no adhesive remaining; 1, <50% adhesive remaining; 2, ≥50% adhesive remaining; or 3, all adhesive remaining, with a distinct impression of the bracket base.
Statistical analysis
All data were analyzed statistically; descriptive statistics, including the mean and standard deviation, were calculated for each group using the SPSS software (ver. 16.0; IBM, Chicago, IL). In addition, the Kolmogorov–Smirnov and Levene tests were used to verify normality and homogeneity of variance. If normality was detected, ANOVA followed by the Scheffe test or the Games–Howell test as a post hoc test was used. If normality was not detected, the data were analyzed using the Kruskal–Wallis H-test followed by the Mann–Whitney U test with Bonferroni's correction.
Differences in the distributions of ARI scores were analyzed using the Mann–Whitney U test. p Values <0.05 were considered to indicate statistical significance.
Results
Temperature increases in the bracket base and pulp chamber
Figure 1 shows the temperature increases of the bracket bases with irradiation for 3, 4, 5, and 6 sec at an intensity of 5 W (Fig. 1a, b) or 7 W (Fig. 1c, d) with and without air cooling. Under all irradiation conditions, the temperatures continued to rise after laser irradiation, and they reached the maximum value at a few seconds after irradiation. The laser irradiation conditions under which the temperature exceeded 80°C, the point at which the microcapsules expand, were 5 and 6 sec at 7 W, regardless of air cooling.

The temperature increase in bracket bases after laser irradiation. The condition that exceeded 80°C, at which the microcapsules expand, was 7 W for 5 or 6 sec.
The temperature in the pulp chamber continued to rise for 50 sec after irradiation, and the maximum temperature increases in the pulp chamber temperature with 5- and 6-sec 7 W irradiations were 5.3°C and 5.9°C with air cooling and 6.6°C and 7.4°C without air cooling, respectively (Fig. 2). The only condition under which the temperature rise did not exceed 5.5°C, which has been reported to induce pulp damage, was at 7 W for 5 sec with air cooling. We therefore decided to use 7 W for 5 sec with air cooling as the optimal irradiation condition.
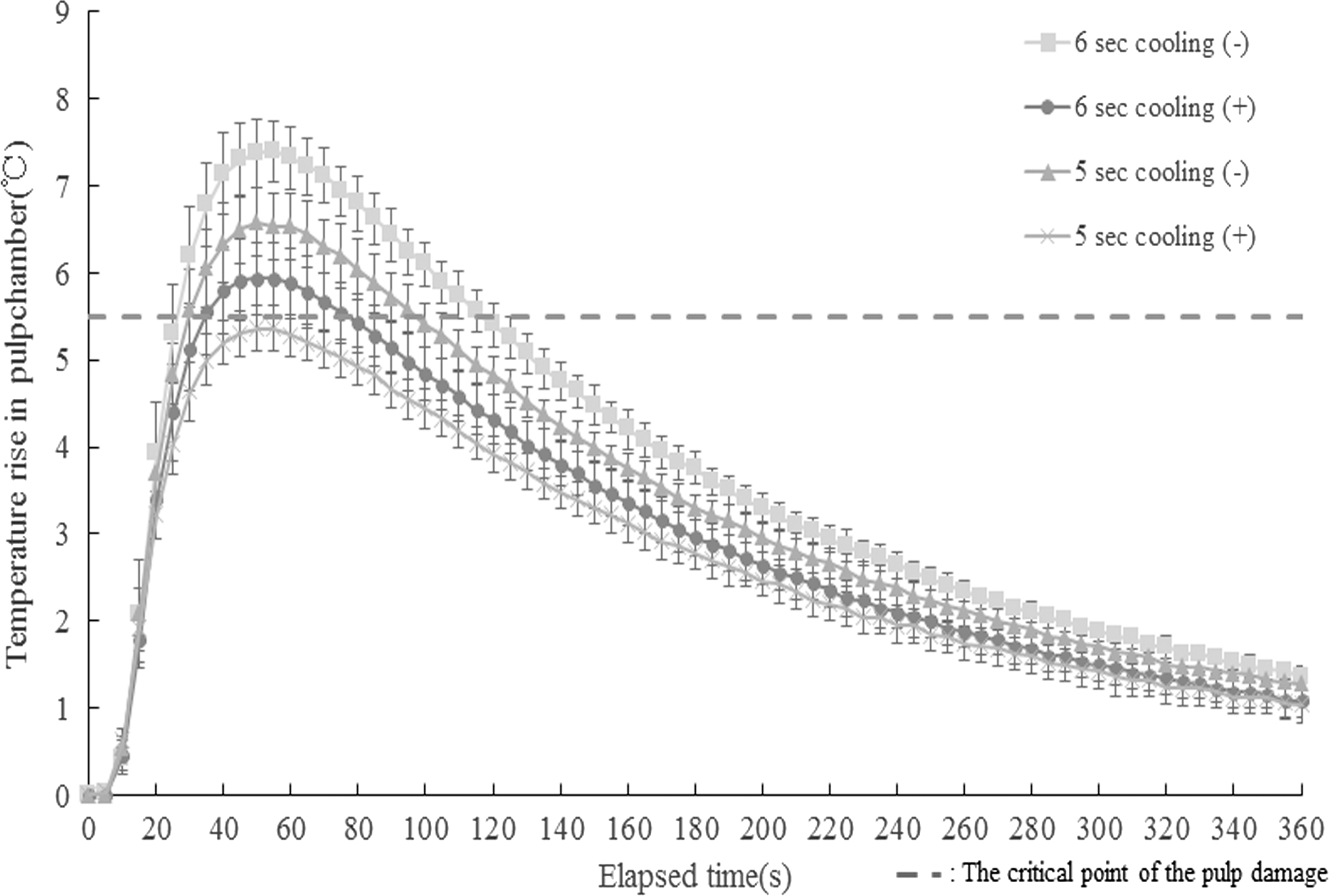
Temperature increase in the pulp chamber after laser irradiation. The temperature in the pulp chamber continued to rise for 50 sec after irradiation, and the maximum temperature increases in the pulp chamber for 5 and 6 sec of 7 W irradiation were 5.3°C and 5.9°C with air cooling and 6.6°C and 7.4°C without air cooling, respectively. It was only at 7 W for 5 sec with air cooling that the temperature increases did not exceed the temperature of pulp damage (5.3°C).
Measurement of bond strength
Shear bond strengths in each group are shown in Fig. 3. In the no-laser groups, there was no significant difference in the bond strength among the 0%, 10%, 20%, and 25% groups, all of which were about 13–17 MPa. However, the bond strength in the 30% group decreased significantly (6.8 MPa) compared with that in the 0% group. In the laser groups, the bond strength in the 0% and 10% microcapsule groups decreased to 0.81- and 0.89-fold with laser irradiation, and they showed no significant differences compared with strengths in the no-laser controls. However, in the 20% and 25% groups, the bond strength decreased significantly, to 0.39- and 0.17-fold, respectively, with laser irradiation compared with the no-laser control.
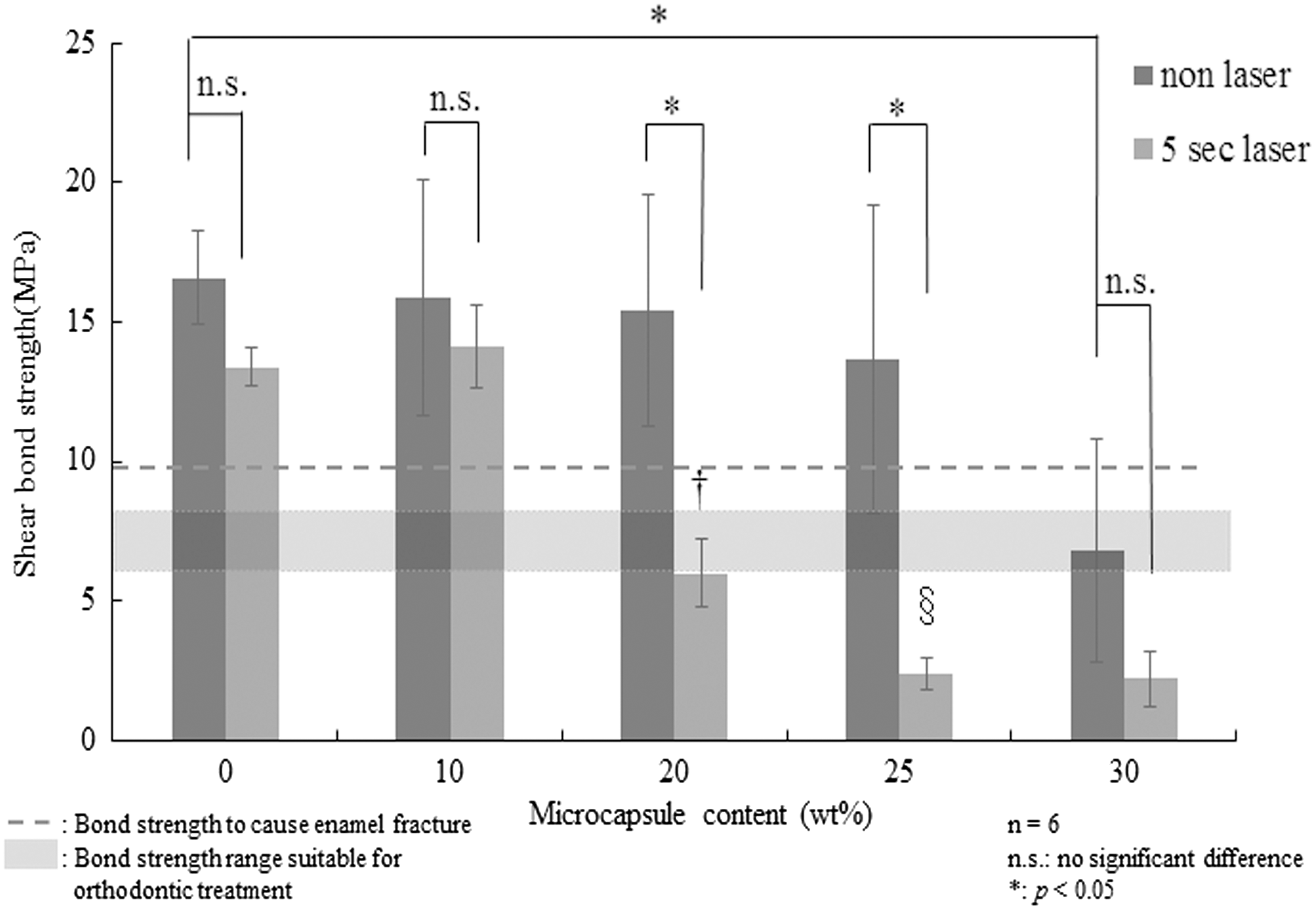
Measurement of shear bond strength. In nonlaser groups, there was no significant difference in the bond strength among 0%, 10%, 20%, and 25% groups; they were all about 13–17 MPa. However, the bond strength in the 30% group decreased significantly (6.8 MPa) compared with that in the 0% group. In the laser groups, the bond strengths in the 0% and 10% microcapsule groups decreased, to 0.81- and 0.89-fold, with laser irradiation, but they were not significantly different from those of the no-laser controls. The bond strengths in the 20% and 25% groups with laser irradiation decreased significantly, to 0.39- and 0.17-fold, compared with the no-laser control. †, Significant difference; V.S. laser group of 0%, 10%, 25%, and 30% groups (p < 0.05). §, Significant difference; V.S. laser group of 0%, 10%, and 20% groups (p < 0.05).
Further, the bond strength of 25% group was significantly lower compared to that of 20% group.
Assessment of residual adhesive
Residual adhesive results after the bond strength test are shown in Table 1. There was no significant difference between laser group and no-laser group, and among 0–30% microcapsule groups.
ARI scores: 0, no adhesive left on tooth surface; 1, <50% of adhesive left on tooth surface; 2, ≥50% of adhesive left on tooth surface; or 3, all adhesive left on the tooth surface.
ARI, adhesive remnant index.
Discussion
In previous study 15 using a chemical cure-type orthodontic adhesive containing heat-expandable microcapsules, the bond strength decreased to 0.40- to 0.48-fold with CO2 laser irradiation, and the mean temperature rise of the pulp chamber was less than that required to induce pulp damage.
Light-cured orthodontic adhesives have recently become common because of their long positioning time and rapid high-strength cure. 16 Thus, according to previous study, we sought to mix microcapsules into the resin composite paste of a light-cured orthodontic adhesive, which has been used widely clinically. However, it was difficult to mix the two uniformly and sufficient bond strength could not be obtained. A light-cured adhesive system has two bonding resin layers (bonding agent layer and resin composite paste layer) between the tooth and bracket. Thus, we mixed the microcapsules with liquid bonding agent instead of composite paste, and a ceramic bracket was bonded using liquid bonding agent containing microcapsules and composite paste. As a result, we could establish a bracket debonding system where the shear bond strength was not decreased during treatment, but was significantly decreased in debonding by CO2 laser irradiation.
We examined the temperature rise >80°C on bracket bases by some CO2 laser irradiation methods because of the need to expand the microcapsules. A temperature increase over 80°C was only seen with 5- and 6-sec irradiation at 7 W. Then, we confirmed the temperature increase in the pulp chamber with laser irradiation using human premolar teeth, on which a ceramic bracket was bonded. It has been reported that because the light of a CO2 laser is readily absorbed by polycrystalline ceramic brackets, the heat produced from the CO2 laser hardly reaches the pulp chamber. 11,17,18 Zach and Cohen 19 reported that, in macaque monkeys, 85% of the tissue in a pulp chamber recovered if the heat stimulation was less than 5.5°C. Thus, we tried to identify irradiation conditions that would not cause an increase exceeding 5.5°C in the pulp chamber. The temperature in the pulp chamber continued to increase even after CO2 laser irradiation, and it reached a maximum temperature 50 sec later. Only irradiation at 7 W for 5 sec with air cooling did not exceed the pulp damage temperature reported by Zach and Cohen (Fig. 2). Because the temperature increase under conditions of 5 sec at 7 W with air cooling was close to the critical point for pulp damage, we examined a water cooling method after irradiation. Because the bracket base temperature reached 80°C about 8 sec after irradiation started (Fig. 1c), cold water (water temperature: 20°C) was dropped on to the bracket 8 sec after laser irradiation, and the temperature rise in the pulp chamber was examined. Results showed that the temperature increase was markedly suppressed; it increased by a maximum of only 3.1°C (Fig. 4). Thus, to suppress pulp damage, water cooling is likely safer.
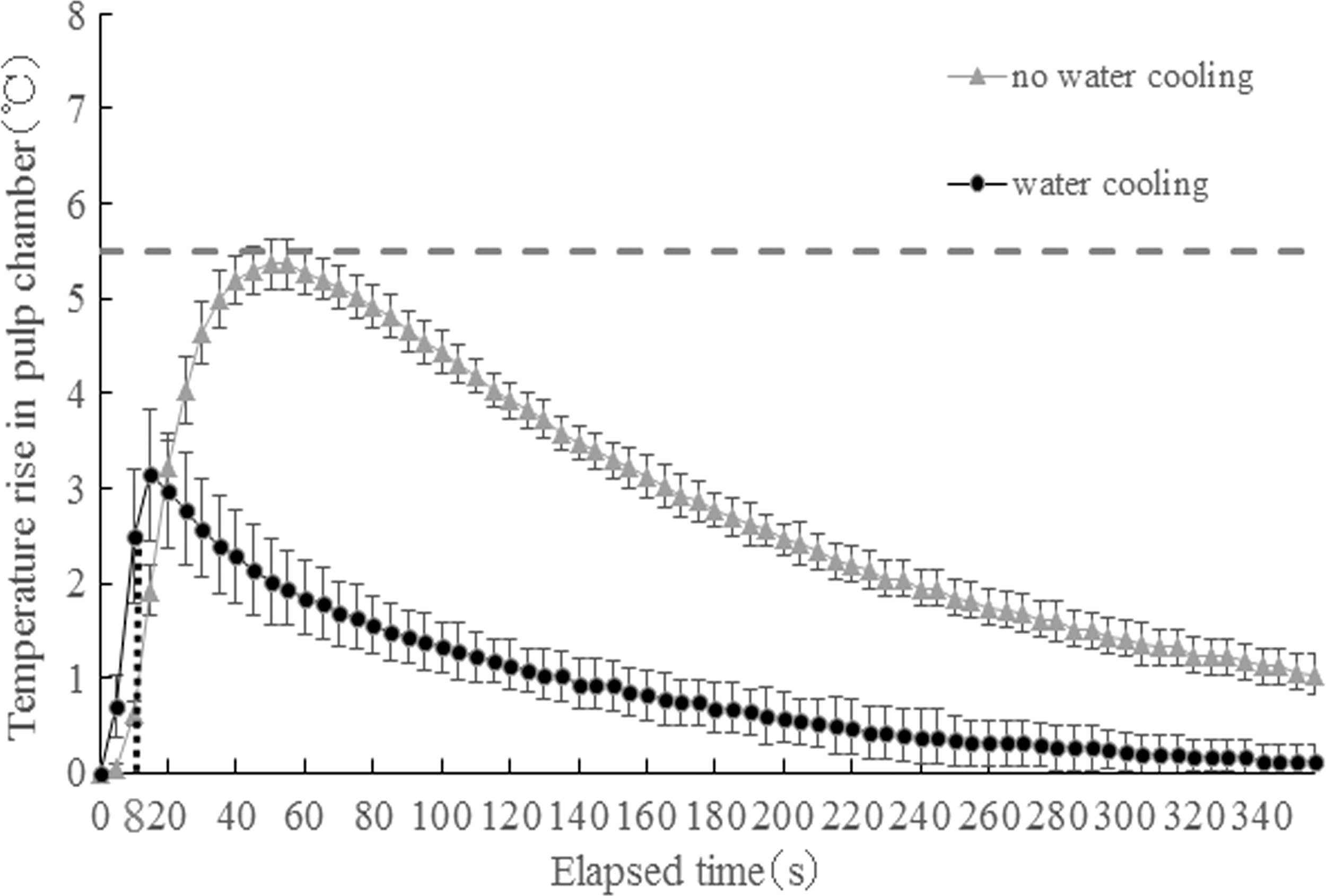
Effect of water cooling on the temperature increase in the pulp chamber. Because the bracket base temperature reached to 80°C at about 8 sec after laser irradiation started (Fig. 1c), cold water (water temperature: 20°C) was dropped onto the bracket 8 sec after irradiation, and the temperature increase in the pulp chamber was examined. The temperature increase was markedly suppressed, increasing by only 3.1°C at the maximum. (---: The critical point of the pulp damage.)
Retief 20 reported that an enamel fracture occurred when the loading during bracket removal exceeded 9.7 MPa. Rix 21 reported increases in enamel fractures by 16% due to high bond strengths of 10.99–20.19 MPa. Reynolds 22 reported that bond strength of 6–8 MPa was suitable for clinical application. In this study, we found that bond strengths with 25% microcapsule contents decreased significantly, to 0.17-fold (2.36 MPa), at 10 min after laser irradiation versus with no-laser irradiation, and the bond strengths were much lower than the thresholds (about 10 MPa) suggested by Retief, Rix, and Reynolds.
A characteristic of the Bis-GMA-type resin used as a light-cured orthodontic adhesive is the property of thermoplasticity; decreased bond strength due to heating recovers soon after cooling. Tozlu et al. 14 reported that the decreased bond strength after laser irradiation increased and recovered in 18 sec. That is, the bracket must be removed while the resin is heated, and this makes the operation extremely dangerous. However, because the bond strength does not recover after the microcapsules expand once, there is a great advantage in that the brackets can be removed at any time after cooling.
In our study, there was no significant difference in the bond strengths of 0% and 10% microcapsule content between before and 10 min after irradiation, which may suggest that the bond strength recovered after laser irradiation. However, the bond strengths of the 20% and 25% microcapsule mixtures decreased significantly after laser irradiation compared with vales before irradiation (Fig. 3). In the 20% and 25% groups, the bond strength was sufficient for clinical use (over the horizontal gray band), but the decrease in bond strength by laser was much greater in the 25% group than in the 20% group. Thus, it seems likely that the orthodontic bonding agent containing 25% microcapsules facilitated removing brackets with light force without inducing fracture of the tooth enamel and ceramic bracket after laser irradiation.
ARI scores were not related to the presence of laser irradiation and microcapsules, because there was no significant difference between the laser group and no-laser group, and among 0–30% microcapsule groups.
By use of the orthodontic adhesive containing the microcapsules in the bonding agent, the bond strength of the bracket during orthodontic treatment can sufficiently withstand the orthodontic force, and at the time of debonding the devices, it was possible to reduce the bond strength to less than 1/5 with the CO2 laser irradiation. This method is likely to be sufficiently applicable to clinical orthodontic treatment.
Conclusions
Within the limitations of this study using a light-cured orthodontic adhesive, the following conclusions can be drawn: (1) Bond strength using the bonding agent containing 25% microcapsules was sufficient for orthodontic treatment (13.69 MPa) and decreased significantly, to 0.17-fold (2.36 MPa), with 5 sec of CO2 laser irradiation compared with the strength before irradiation. (2) The temperature rise in the pulp chamber was less than 5.5°C, that is, the temperature that induces pulp damage, with 5 sec of CO2 laser irradiation.
From these results, it seems likely that the combined use of a light-cured orthodontic bonding agent containing 25% microcapsules and CO2 laser is an easier debonding system for ceramic brackets, with less debonding time and enamel damage.
Footnotes
Acknowledgments
This work was supported, in part, by the Sato Fund, Nihon University School of Dentistry, in 2017.
Author Disclosure Statement
No competing financial interests exist.