
Abstract
P
In a prospective study on a small cohort of superficial BCC, we previously determined the optimal protocol for reducing pain by both 633 nm laser and 570–670 nm red light-emitting diode (LED) light treatment. 7 In this two-step irradiation, most of the PpIX photobleaching took place at a lower irradiance eliminating or markedly reducing pain associated with PDT, similar to earlier findings by our research group. 2 In our current report, we show that the same treatment scheme effectively controls red LED light PDT-induced pain in a larger cohort of patients treated for AK.
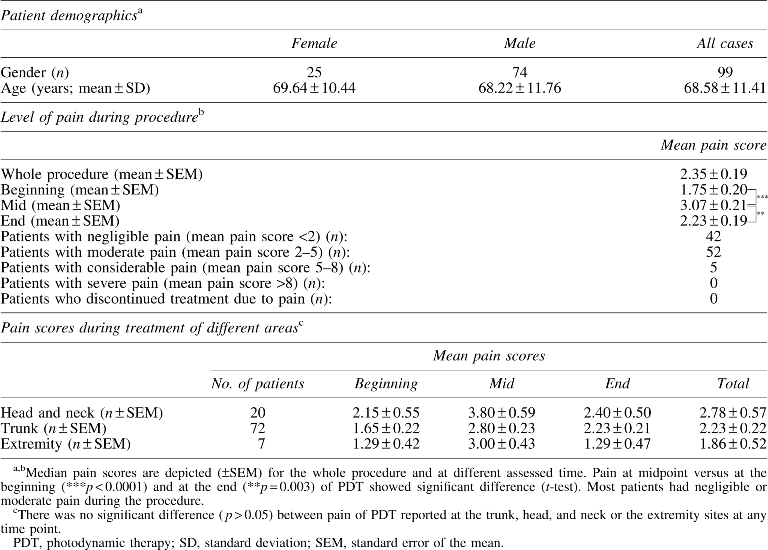
A retrospective chart review to assess level of pain during treatment of AKs was performed. All patients included in the study were treated at a single site. The treated skin areas had over five clinically identifiable AKs. The sites were cleansed and lightly debrided by 3M dot tape (3M, USA) and ALA (DUSA Pharmaceuticals, USA) was applied topically to the whole irradiated skin area. After 1–3 h incubation, the treatment areas were subjected to red LED light (570–670 nm, Aktilite CL128; Galderma Laboratories, USA) treatment. Initially 10 J/cm2 dose was delivered using a natural density filter (Norman ND-10, item NR4350; Calumet Photographic, USA) to reduce intensity to 35 mW/cm2. 7 After the first step of irradiation, the natural density filter was removed and irradiation was continued at 70 mW/cm2 for a total dose of 65 J/cm2. Total irradiation time was 1440 sec (24 min) and total dose was 75 J/cm2. A total of 99 patients were treated between January and November of 2015. Pain level was measured at the start, at midpoint, and at the end of treatment using a 0–10 point (no pain to unbearable pain) visual analog scale. All the pain data reflect pain observed during treatment of a single site. In the limited cases of marked pain during the irradiation, air cooling by fan was used during light delivery, and in few cases of reported considerable pain, light delivery was halted for 1–2 min to help with pain control.
The patient demographics, treatment sites, and the results of the documented pain levels are depicted in Table 1. All the patients tolerated the treatment well and PDT did not have to be discontinued. No significant posttreatment side effects were encountered. Pain was low to moderate in most patients with only five patients reporting considerable pain (Fig. 1). Although the pain was generally low, there was still significantly higher midprocedure pain versus at the beginning (p < 0.0001) and at the end (p = 0.003) of PDT. There was no statistically significant difference between the tolerability of the treatment at the different treatment sites and women and men showed no significant difference in reported pain (Table 1).

Pain during different phases of two-step irradiance red light ALA
Perceived pain and fear of pain are among the most important determinants of patient healthcare perception and factors in noncompliance. 8 Cooling, systemic, topical, and block anesthesia can reduce PDT-induced pain. 9 Medical analgesia has inherent complications, and cooling during PDT has been shown to result in decreased treatment efficacy. 10 Although daylight PDT also results in excellent outcomes with reduced pain, the widespread use of daylight PDT may be limited by geography, temperature variations, and healthcare settings. 5 To address this challenge recently, in-office “painless PDT” protocol with a short incubation time followed by extended blue light activation, simulating daylight PDT, has been shown to be associated with little to no pain. 6 The pain during conventional PDT procedure usually peaks early when around 20 J/cm2 dose is delivered, 2,4 arguing that irradiance during these initial phases of PDT is crucial for controlling pain. Low-level light activation in the initial phase of PDT reduced pain during treatment of BCC by decreasing the amount of available photosensitizer (photobleaching). 2,7
Our current results provide evidence that red light ALA PDT of AKs is remarkably well tolerated with the two-step irradiance light treatment protocol with only negligibly increased treatment times compared with a conventional one irradiance protocol. Prior results showed that two-step irradiance markedly reduced pain during nonmelanoma skin cancer treatment. 2,7 Therefore, a study to directly compare two-step-irradiance and the expectedly more painful conventional single irradiance PDT was ethically unacceptable. During two-step light treatment a slight but significant increase in pain was seen early after switching to higher irradiance, when around 20 J/cm2 dose was delivered (Table 1). This indicated even in the absence of direct comparison to continuous high-dose irradiance that higher irradiance causes higher level of pain during AK treatment.
Our results in light of the very good tolerability of continuous low-dose irradiance PDT also suggests that further fine tuning of the two-step irradiance protocol by extending the low irradiance in the early phase of the PDT, possibly to deliver 20 J/cm2 instead of the currently used 10 J/cm2, may render two-step irradiance PDT pain-free for most patients, while still keeping treatment times reasonably short. 6 Previously, we and others have shown that two-step light treatment does not reduce the efficacy of PDT. 2,7 This taken together with our current work argues that two-step light delivery increases patient comfort at no loss of efficacy, and therefore should be more widely used for treatment of both AKs and BCC. The used natural density filter, and similar ND filters are well characterized and very affordable reusable devices that enable modification of PDT protocols in all offices at negligible cost 7 to provide effective in-office PDT for AK with minimal to no treatment-related pain.
Footnotes
Author Disclosure Statement
No competing financial interests exist.