
Abstract
Introduction
T
In recent decades, there has been an increase in the incidence of tendinous lesions partly due to increased participation in recreational and competitive exercise. 3 –5 Tendon lesions represent 30–50% of sports-related injuries, and Achilles tendinopathy represents 55–65% of total tendon injuries. 6 Risk factors include gender, ageing, obesity, comorbid musculoskeletal conditions, 6,7 and antibiotics, especially Quinolones 8 and corticosteroids. 9
Tendon injury is followed by an inflammatory phase with edema, leukocyte infiltration, phagocytosis of dead tissue, and the production of humoral mediators. Hereafter, a proliferative phase with production of type III collagen follows, and a remodeling phase with decreasing inflammation and scar tissue formation, with gradual maturation and reorganization of tissue. This remodeling and maturation phase can last up to 1 year, which can hinder return to physical activities. 10
Andres and Murrell 11 conducted a literature review and concluded that nonsteroidal anti-inflammatory drugs (NSAIDs) should be the first-line treatment for Achilles tendinopathy in the short term, followed by physiotherapy if symptoms persist. However, studies investigating the effects of anti-inflammatory drugs in animal models of tendon injury are conflicting. 12 –16 Recently, we demonstrated that the NSAID diclofenac increased the risk of sudden ruptures, decreased tendon elasticity, and caused deleterious effects in tendon morphology. 17
Glucocorticoid steroids (GCS) are also used to treat acute musculoskeletal injuries, although long-term benefits have been questioned because they may reduce tensile strength by interfering with the fiber repair process. 17,18 Wong et al. 19 found that GCS reduced the proliferation of cultured human tendon fibroblasts and the synthesis of extracellular matrix. Thus, some commentators believe that GCS should be used as a last resort in treatment of tendinopathy. 20
Low-level laser therapy (LLLT) has been used to treat tissue damage and inflammatory processes since the 1960s, although the first reports of beneficial effects on tendon injuries following physical activity were not published until the 1980s. Since then, clinical studies have consistently shown positive outcomes from LLLT on musculoskeletal and neuropathic conditions, including tendon injuries. 21 Beneficial effects have been attributed to a modulatory effect on the dose-dependent metabolism of fibroblasts and collagen deposition, and/or attenuation of inflammation by inhibiting the enzyme cyclooxygenase-2 reducing formation of prostaglandin E2 (PGE2), in a manner similar to anti-inflammatory drugs. 17,22 Enwemeka, 23 found that laser irradiation at certain doses stimulates fibroblast proliferation and promotes the release of fibroblast growth factor (FGF), which can improve the balance between degradation and production, culminating in the healing of the injured tendon.
Bjordal et al. 22 found that a LLLT dose of 5.4 J per treatment point reduced the concentration of PGE2 and increased pain threshold in tendons of individuals with Achilles tendinopathy. Stergioulas et al. 24 found that LLLT combined with an eccentric exercise program for 12 weeks reduced pain and crepitus during palpation and increased ankle joint dorsiflexion, accelerating patient recovery. In a systematic review with meta-analysis of randomized controlled clinical trials on the efficacy of LLLT for tendinopathy, Tumilty et al. 25 found that studies using doses recommended by the World Association for Laser Therapy (WALT) tended to report efficacy for LLLT.
The aim of this study was to evaluate the effects of LLLT, diclofenac, and dexamethasone on inflammation, tissue reorganization, and repair processes in Achilles tendinopathy induced by injection of collagenase in rats.
Materials and Methods
Animals
Two hundred five female Wistar rats 8–10 weeks of age, each weighing 200–250 g (central animal house of the Institute of Biomedical Sciences, University of São Paulo) were used and maintained under standard conditions (temperature = 22°C–24°C, humidity 40–60%, 12-h light–12-h dark cycle, and food and water ad libitum). Experimental protocols were approved by the Ethics Committee on Animal Experimentation of the Institute of Biomedical Sciences, University of São Paulo (Record No. 144/sheet 78/book 02).
Experimental groups and procedure
Animals were allocated to one of the following groups: healthy control (control); injury+no-treatment control (NT); injury+LLLT (LLLT); injury+diclofenac (NSAID); and injury+dexamethasone (GCS). Animals in the “injury groups” were anesthetized (intraperitoneal) with a mixture of ketamine and xylazine (90 and 10 mg/kg, respectively; König, Avellaneda, Argentina) and administered 100 μg of collagenase (Sigma Chemical Co., St. Louis, MO) diluted in 100 μL of sterile saline (0.9%) by percutaneous injection into both hindlegs in the area of the Achilles tendon. Animals were kept warm until closure of the anesthetic effect thereby avoiding accidental death resulting from hypothermia caused by anesthetic. After injection of collagenase, animals were treated according to group allocation and then five animals from each group were sacrificed by halothane overdose at each of the following time points after the induction of injury: 12, 24, 48, 72 h, 5, 7, 14, 21, 28, and 60 days.
Healthy control (control group)
Five animals were administered 100 μL of sterile saline (0.9%, i.e., the vehicle) injected into the peritendinous region of both legs and were not subjected to any other procedure.
Injury+no-treatment control (NT group)
Animals in this group were not subjected to any treatment after collagenase injection.
Injury+LLLT (LLLT group)
One hour after collagenase injection, animals were treated with LLLT administered at a single point in contact over the region of injection of both tendons. A DMC Laser (São Carlos, SP, Brazil), was administered once a day for 7 days as follows: Irradiation time = 30 sec; wavelength = 810 nm; mode = continuous; power = 100 mW; spot area = 0.0028 cm2. The energy dose was 3 J based on the findings of a dose–response study conducted in our laboratory. 18
Injury+diclofenac (NSAID group)
After collagenase injection, the animals were treated with diclofenac (Novartis SA Campinas, Brazil) administered orally at a dose of 1.1 mg/kg. Diclofenac was administered 1 h after injury and twice daily for 7 days postinjury.
Injury+dexamethasone (GCS group)
After collagenase injection, the animals were treated with dexamethasone disodium phosphate (Ache Laboratory, Brazil) at a dose of 0.02 mg/kg. Dexamethasone was administered through intramuscular injection 1 h after induction and once a day for 7 days.
Preparation of tissue samples
After animals were sacrificed, whole tendons were removed from the injected legs and fixed in 10% formalin for a period of 72 h. The tendons were then dehydrated and subjected to a series of graded alcohol baths, starting with 50% and progressing to 100% absolute alcohol. Tendons were diaphonized with Xylene (Labsynth, Diadema, SP, Brazil) for impregnation (soaking) and placed in aluminum containers fused with Paraplast® (Leica Microsystems Wetzlar GmbH, Nussloch, Germany) for 4 h. After impregnation, tendons were placed in a small container covered with molten paraffin and allowed to harden, forming a block containing tendon tissue. Longitudinal samples (5 mm thick) were taken using a Leica® microtome (model RM2125 RT; Leica Microsystems Wetzlar GmbH) and placed in a water bath. Each sample was divided into three segments, mounted, and divided into five slices taken from each segment. The most representative slices were stained with Hematoxylin and Eosin, one slice was stained with Picrosirius Red, and one slice was unstained.
Each slice was analyzed using microphotography at 100 × and 400 × magnification (Nikon® optical microscope, Eclipse model E-200; Nikon Corporation, Japan; Dino-Lite Digital Microscope® DinoEye AM423X; Anmo Electronics Corp., Hsinchu, Taiwan; connected to an Apple® MacBook Pro, model MB990BZ/A; Apple, Inc., Cupertino, CA). A collection of photographs were taken for each slice. Tissue samples were prepared by a technician and analyzed by a researcher, both blinded to group allocation throughout analysis.
Histological analysis
Samples of epitendon and paratendon tissues were stained with Hematoxylin and Eosin, and semiquantitative histological data were collected by viewing the sample at 400 × magnification. The status of neutrophils, lymphocytes, plasma leakage, and hemorrhage was classified on a four-point scale from absent to mild, moderate, or intense. The average of three fields of observation for each tendon sample (15 fields per group) was used as a summary measure of outcome.
Analysis of collagen amount
Picrosirius Red staining was used to obtain semiquantitative data reflecting the relative collagen amount present in the intratendinous region, using a protocol adapted from Cohen et al. 26 Microphotography images (100 × magnification) were converted into 8 bits and standard gray tint and analyzed using ImageJ software (version 1.43u). The relative collagen amount (arbitrary units) was determined using the mean value of pixels in a brightness (gray) scale from 0 (no collagen) to 255 (maximum amount of collagen).
Analysis of structural organization of collagen fibers
Unstained tendon samples were used to analyze the structural organization and aggregation of collagen fibrils. Unstained histological slides from each group were immersed in distilled water (refractive index 1.333) for 30 min, then placed on slides and covered with coverslips containing distilled water between the surfaces of slide and coverslip. Birefringence is the optical property whereby a material has two indices of refraction causing light to penetrate and spread into the material in different directions and speed, such as ordinary ray (no) and extraordinary ray (ne). Optical retardation is the difference between these two rays. 27 Polarizing light microscopy 27 was used to measure optical retardation using a Leica model DMRX Leica microscope (10 × objective Pol/0.22, 0.9 condenser Sénarmont compensator λ/4, monochromatic light λ = 546 nm) and interference filter under the guidance of Prof. Dr. Nivaldo Antonio Parisotto (Department of Materials Engineering [LAMAV], Federal University of São Carlos, Brazil), using specifications suggested by Vidal. 28
Measurements were taken with the tendon axis at 45° with respect to microscope filters (polarizer and analyzer). At this angle collagen fibers exhibit the greatest glow birefringence, and hence a high value of optical delays, because most of the collagen fibers are oriented in the long axis of the tendon. 27 An increase in the amount of birefringence is related to increased crosslinking between the collagen fibrils, increasing the crystallinity and ordered aggregation of collagen type I. 28 Ten measurements of birefringence, two for each tendon, were taken randomly for each sample.
Statistical analysis
Data are expressed as mean ± standard error of the mean (SEM), and ANOVA (analysis of variance) with Tukey's posttest for multiple comparisons was used to determine differences between groups. p Values <0.05 were considered statistically significant.
Results
Histological analysis
The histological appearance of injured Achilles tendons 12 h after injection of collagenase for each of the treatment groups are presented in Fig. 1. Scores for neutrophils, lymphocytes, plasma leakage, and hemorrhage from the different groups at the measurement time points are presented in Table 1. Healthy control is not included due to absent markers on all time points. Total scores are presented in Fig. 2.
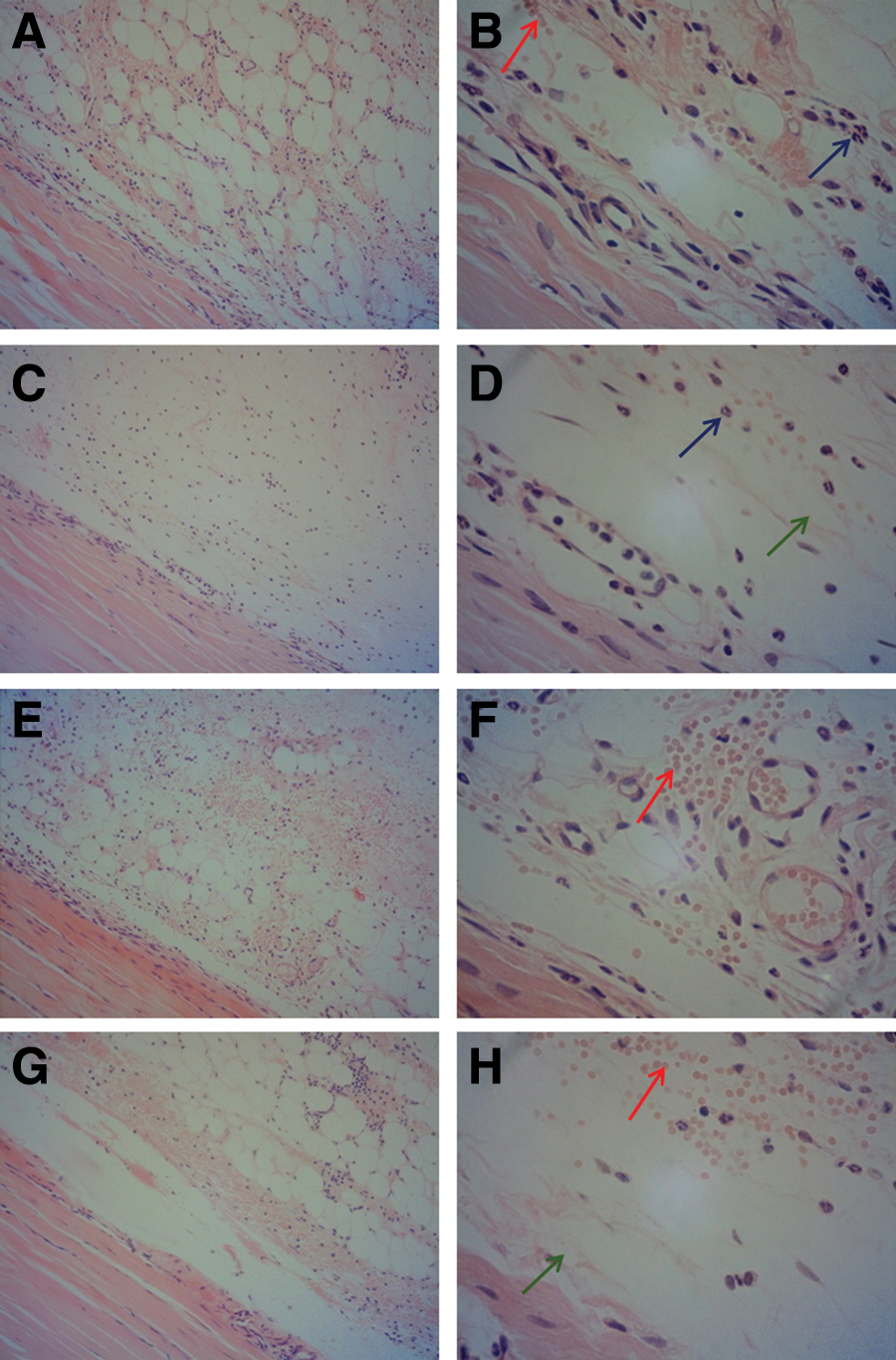
Histological appearance of rat Achilles tendon tissue samples stained with Hematoxylin and Eosin 12 h after collagenase injection. Left column exhibits 100 × magnification, right column exhibits 400 × magnification of the same sample.
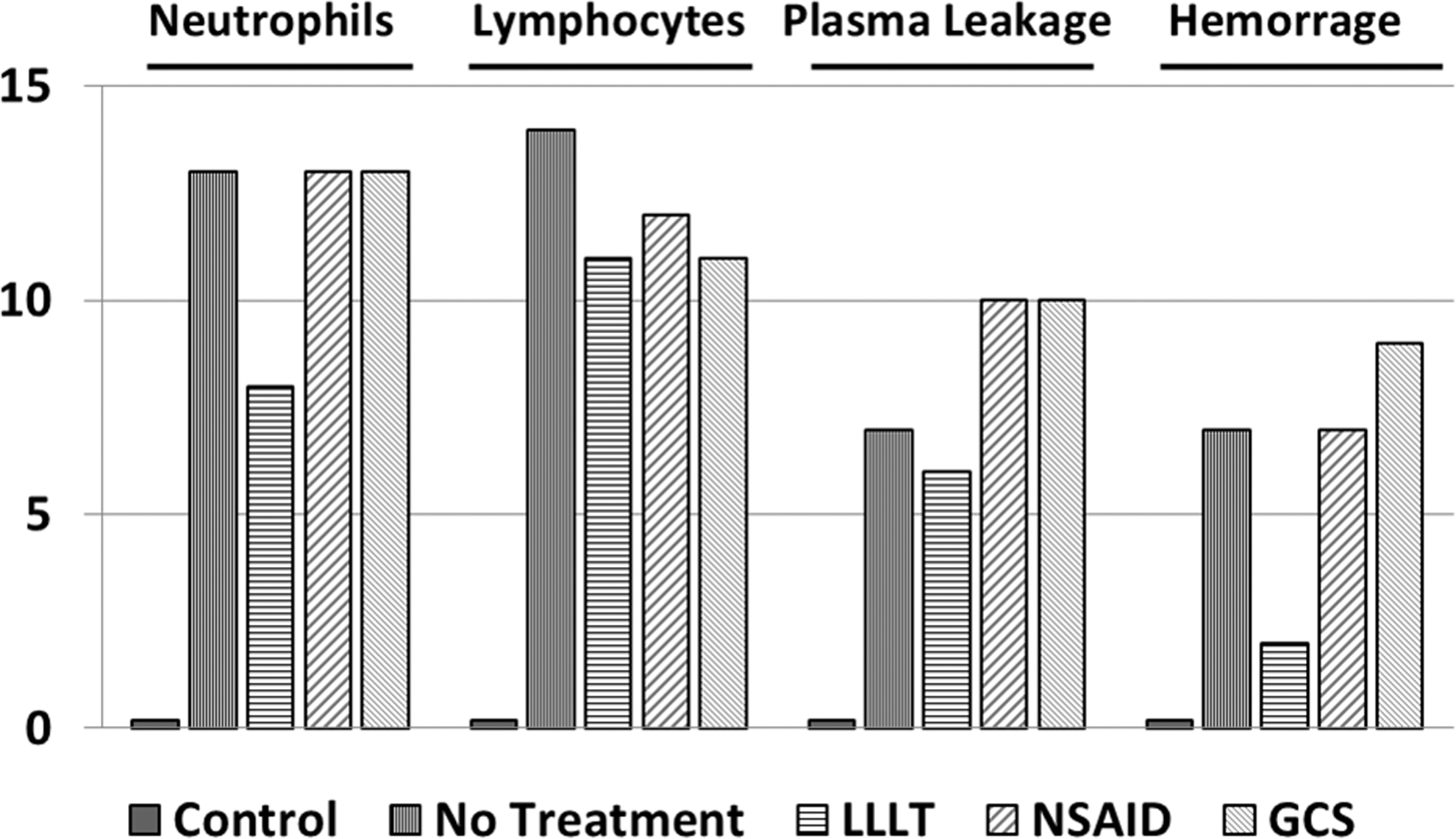
Total score of the histological analysis of healthy control (control), injury+no-treatment control (NT), injury+LLLT 3 J (LLLT), injury+diclofenac 1.1 mg/kg (NSAID), and injury+dexamethasone 0.02 mg/kg (GCS). GCS, glucocorticoid steroids; NSAID, nonsteroidal anti-inflammatory drug.
Representative symbol and rating: − = absent, + = mild, ++ = moderate, +++ = intense.
GCS, glucocorticoid steroids; LLLT, low-level laser therapy; NSAID, nonsteroidal anti-inflammatory drug; NT, no-treatment control.
Analysis of the amount of collagen I
Mean ± SEM values for the relative amount of collagen I in each group at 12, 24, 48, and 72 h is presented in Fig. 3. The amount of collagen I was lower in injured groups compared with the healthy control group at 12 h (NT = 86 ± 2.8, LLLT = 95 ± 3.9, NSAID = 88 ± 6.1, GCS = 71 ± 2.6, control = 132 ± 5.8, p < 0.001) and at 24 h (NT = 82 ± 3.1, LLLT = 94 ± 4.2, NSAID = 78 ± 8.4, GCS = 64 ± 2.2, control = 132 ± 5.8, all comparisons p < 0.001). The relative amount of collagen I was significantly higher in the LLLT group compared with the GCS group (p < 0.01) at both 12 and 24 h. At 48 h the relative amount of collagen I was lower in injured groups compared with the healthy control group [control = 132 ± 5.8, NT = 106 ± 7.5 (p < 0.05), LLLT = 104 ± 6 (p < 0.05), GSC = 95 ± 4.2 (p < 0.01)]. There were no statistically significant differences in the relative amount of collagen I between groups at any of the other measurement time points (72 h and 5, 7, 14, 21, 28, and 60 days).
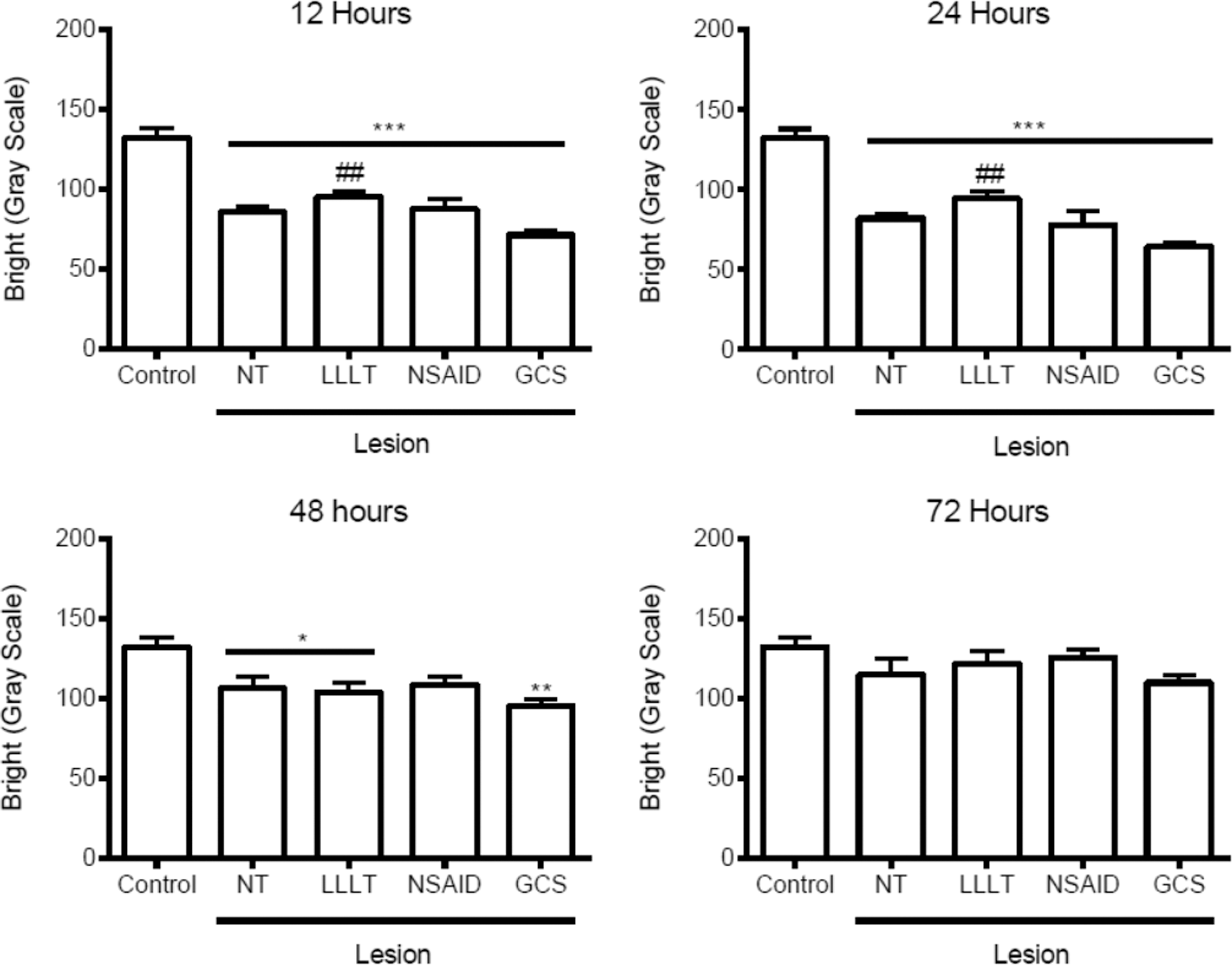
Mean ± SEM collagen amount in Achilles tendon samples 12, 24, 48, and 72 h after collagenase injection, healthy control (control), injury+no-treatment control (NT), injury+LLLT 3 J (LLLT), injury+diclofenac 1.1 mg/kg (NSAID), and injury+dexamethasone 0.02 mg/kg (GCS). N = 5 per group at each time point, ANOVA with post hoc Tukey's; *p < 0.05 versus healthy, **p < 0.01 versus healthy, ***p < 0.001 versus healthy, ## p < 0.01 versus dexamethasone (GCS). ANOVA, analysis of variance; SEM, standard error of the mean.
Analysis of birefringence
Mean ± SEM values for birefringence measurements in each group at time points up until 21 days is presented in Fig. 4. At 12 h, values for birefringence were higher for LLLT (69 ± 1.4), NSAID (61 ± 1.1), and GCS (50 ± 1.4) groups compared with NT (38 ± 1.2, all comparisons p < 0.001). There were higher values for birefringence for the LLLT group compared with the other treatment groups (p < 0.001). At 24 h, values for birefringence were higher for LLLT (67 ± 1.3), NSAID (58 ± 1.5), and GCS (56 ± 1.4) compared with NT (40 ± 2.5, all comparisons, p < 0.001). There were higher values for birefringence for the LLLT compared with NSAID (p < 0.01) and GCS (p < 0.001). At 48 h, values for birefringence were higher for LLLT (66 ± 1.1) and NSAID (61 ± 1.2) compared with NT (54 ± 1.4, p < 0.01), with values for birefringence higher for LLLT and NSAID (66 ± 3 and 62 ± 5, p < 0.05) compared with GCS (56 ± 1.1, p < 0.001 and p < 0.005, respectively). GCS was not significantly different from NT. At 72 h, values for birefringence were higher for LLLT (65 ± 1.3, p < 0.001) and NSAID (60 ± 1.2, p < 0.05) compared with NT (54 ± 1.4). Values for birefringence were higher for LLLT compared with GCS (p < 0.001).
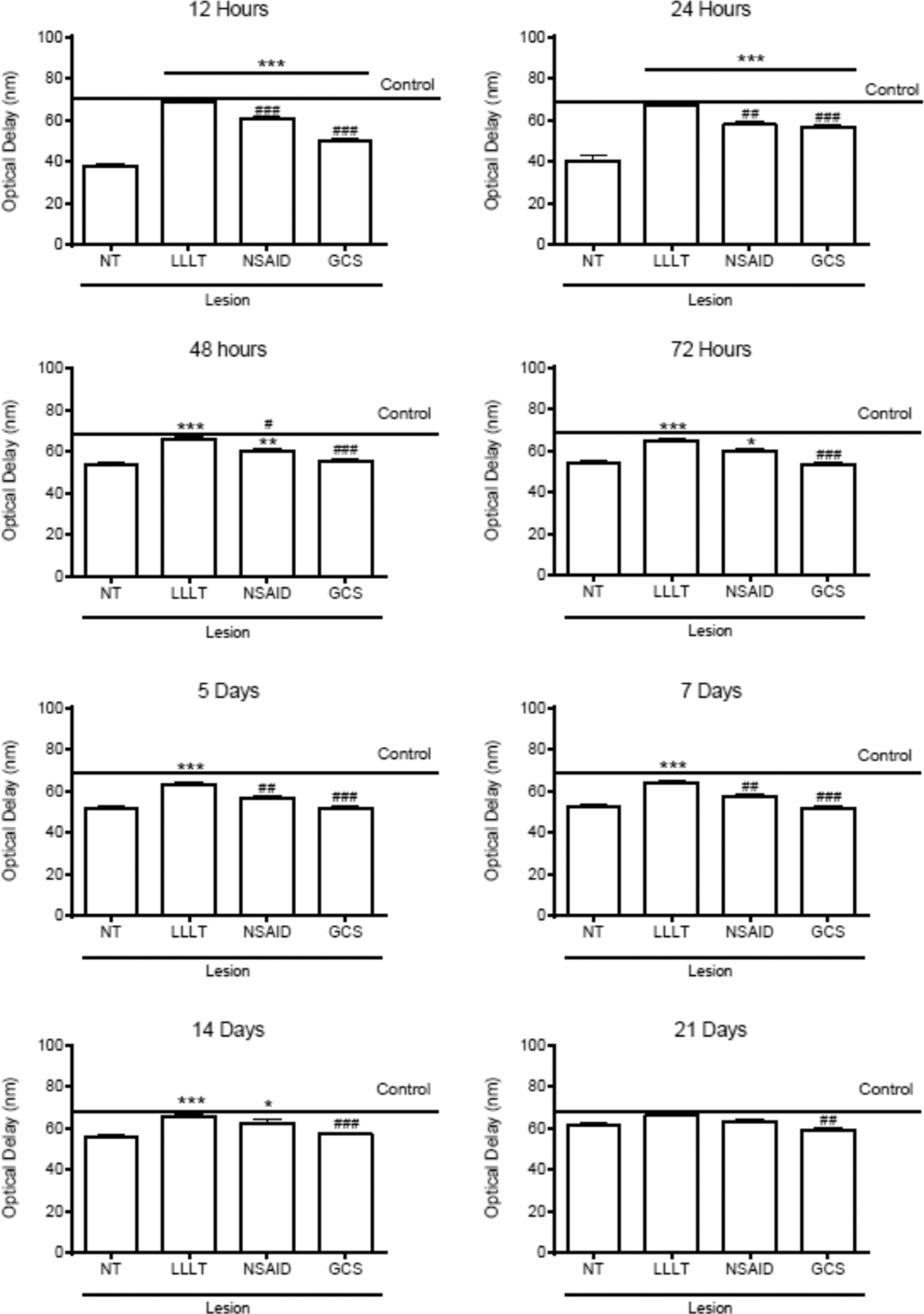
Results of the birefringence analysis. Mean ± SEM of optical delay representing collagen fiber organization in rat Achilles tendon tissue samples at 12, 24, 48, and 72 h and at 5, 7, 14, and 21 days after collagenase injection. N = 5 per group at each time point, ANOVA with post hoc Tukey's; *p < 0.05, **p < 0.01, and ***p < 0.001 all versus no-treatment control (NT). # p < 0.5, ## p < 0.01, and ### p < 0.001 LLLT 3 J (LLLT) versus diclofenac 1.1 mg/kg (NSAID) or dexamethasone 0.02 mg/kg (GCS). The mean results of optical delay of the healthy control group are shown as a horizontal line (control).
At 5 days, values for birefringence were higher for LLLT (63 ± 1.2) compared with NT (52 ± 1.6, p < 0.001), NSAID (57 ± 1.2, p < 0.01), and GCS (52 ± 1.0, p < 0.001). At 7 days, values for birefringence were higher for LLLT (64 ± 1.0) than NT (52 ± 1.7, p < 0.001), NSAID (57 ± 1.4, p < 0.01), and GCS (52 ± 1.6, p < 0.001). At 14 days, values for birefringence were higher for LLLT (66 ± 1.2) compared with NT (56 ± 1.1, p < 0.001) and GCS (57 ± 1.2, p < 0.001). At 21 days, values for birefringence were higher for NT (62 ± 1.1), LLLT (66 ± 1.4, p < 0.05), and NSAID (63 ± 1.5) compared with GCS (59 ± 0.7). At 28 days, there were no significant differences between the groups. At 60 days, there was a significant difference between GCS (64 ± 1.2, p < 0.05) and the healthy control group (69 ± 1.5). None of the other groups was significantly different from the healthy control group at 60 days; LLLT (69 ± 1.2), NSAID (68 ± 1.4), and NT (67 ± 1.3).
Discussion
In this experiment we have studied the process of repair and tissue organization in a model of acute collagenase-induced Achilles tendinitis. The model resulted in physiological responses consistent with acute inflammation; including local vasodilation of small vessels, increased vascular permeability, and leukocyte emigration. This is consistent with findings in studies by Marsolais et al. 29 and Dahlgren et al. 30 and suggests a credible model. In our findings, there was an increase in the number of polymorphonuclear cells in all groups at 12, 24, and 48 h after injury. It has been established that neutrophils are the first cells to arrive at the site of injury, 31 and other inflammatory cells, including macrophages, 32 migrate to the injury site through chemotaxis 29,32 with an increase in local levels of cytokines, reactive oxygen species, 29 and proteases. 31 Interestingly, our findings suggested a slight reduction in the quantity of lymphocytes at the earliest time points for treatment groups with small differences between them.
The most surprising finding in our study was the lack of beneficial effects on plasma extravasation from the groups treated with diclofenac and dexamethasone. Leakage of proteinaceous macromolecules from the plasma into the interstitium was observed in all experimentally injured groups at 12, 24, 48, and 72 h, but neither diclofenac nor dexamethasone reduced the amount of plasma leakage during the first hours and days, with signs persisting 2 days longer than the groups receiving no treatment or LLLT.
Another important finding was that LLLT minimized and resolved hemorrhage faster than diclofenac, dexamethasone, and no-treatment groups. This finding for LLLT is consistent with the results of Aimbire et al. 33 on hemorrhagic lesions induced by immune complex in a high perfusion organ (rat lung), although drugs performed better in the lung injury model than in this study. 33 In the present study, using a collagenase-induced tendinitis model in a low-perfusion organ (tendon), diclofenac, and dexamethasone performed poorly and slightly worse than no treatment. One possible reason for this may have been the dosing regimen. Repeated daily injections for 1 week was used in the collagenase-induced tendinitis model compared with a single injection of dexamethasone in the lung injury model, with effects only measured 24 h after treatment.
Future studies should investigate factors that may influence outcome, including single versus repeated injections, differences in the timing of outcome measures, the slow and largely anaerobic metabolism of the tendons, and the collagenase compound itself.
We found that diclofenac- and dexamethasone-treated groups had higher levels of inflammatory cells, plasma extravasation, and minor bleeding than the LLLT group. Our histological findings were similar to previous studies. Elwakil 34 found improvement in tissue organization and alignment of collagen fibers after a mild inflammatory reaction in tenotomized Achilles tendons in rabbits treated with LLLT. In the injured control group, samples showed bands of unaligned collagen and intense cellular infiltrate and granulomatous reaction. Bertolini et al. 35 reported that LLLT of mechanically damaged rat tendons, reduced pain and swelling in the affected area resulting in improvements in limb function. Fillipin et al. 36 used the same model of injury and found no abnormalities in the tendinous tissue after 14 days of LLLT, whereas there were changes in the tissue architecture, inflammation, and vasodilation in the injured group that received no treatment. These findings in animal models appear to translate to humans. A randomized placebo-controlled clinical trial conducted by our research team 22 found that LLLT reduced PGE2 production by the symptomatic Achilles tendon.
There is inconsistency in the findings of previous studies investigating the effects of NSAIDs on damaged tissue, with some studies reporting that NSAIDs were detrimental to tendon repair 37 or had no effect on tendon repair. 38 Marsolais et al. 39 found that NSAIDs reduced the concentration of neutrophils in the peritendinous region by 59% 1 day after injury when compared with placebo. NSAIDs reduced edema by ∼35% on day 3, although there was no reduction in the volume of plasma extravasation between day 3 and 14 after injury. The authors concluded that NSAIDs did not improve regeneration of the tendon. In the present study, we found that diclofenac reduced the volume of plasma extravasation and the number of inflammatory cells, with possible mechanisms being the inhibition of the aggregation of polymorphonuclear cells, 40 reduction in prostaglandin synthesis, and a reduction in the amount of adhesion molecules thereby inhibiting cell locomotion. 41
The largest difference in effect was observed for the prevention of hemorrhage, where the LLLT group presented with only a mild degree of hemorrhage detected at one time point (12 h after injury). Previous studies have found that LLLT reduces hemorrhage. 42,43 In the present study, we found that hemorrhage subsided within 24 h in the LLLT group and persisted in the dexamethasone group more than the nontreatment group for over 5 days. Our findings are consistent with previous studies, which found that GCS did not reduce hemorrhage after lung contusion injury. 44 Our study provides evidence that dexamethasone produced the least beneficial effects of the three treatment options evaluated, with findings similar to the no-treatment group after 72 h and 14 days.
Evidence to support the use of corticosteroids in tendinopathy is weak and evidence to support the use of NSAIDs is conflicting, although in most studies, authors report the presence of deleterious effects from NSAID use. 19,45,46 It has been reported that parecoxib and indomethacin reduced the tensile strength of tenotomized and sutured supraspinatus tendons at 2 weeks. 37,38 We have previously reported the findings of two experimental studies in which treatment with NSAIDs reduced the ultimate tensile strength and the elasticity of Achilles tendons of rats, seriously compromising the biomechanical properties of the tendon. 17,47 However, animals treated with LLLT had similar biomechanical tendon properties as healthy controls.
In the present study, we found a statistically significant reduction in the amount of collagen present in tissue samples from all groups compared with control animals at 12, 24, and 48 h postinjury, except for the diclofenac group at 48 h. There was a higher amount of collagen following LLLT compared with dexamethasone at 12 and 24 h, which is consistent with the results of several studies that have also found that LLLT stimulates the synthesis of collagen. 23,34,48,49 The mechanism by which LLLT stimulates collagen production during the regenerative process is unclear, but may include change in gene regulation and/or modulation of the action of enzymes involved in metabolism of collagen. 50
Our study found that neither diclofenac nor dexamethasone altered collagen deposition in the injured area when compared with the no-treatment control. Cohen et al. 26 found that indomethacin and celecoxib reduced tensile strength when subjected to an ultimate tensile strength test in rats 60 days after a rotator cuff injury. They also found that NSAIDs inhibited the formation and maturation of collagen in the distal region of the tendon. 51 Methodological differences may account for the discrepancies in findings, including the agent causing the injuries, the concentration of collagenase used, the duration of treatment, the NSAID drugs used, and/or the method of analysis.
We found no differences in the amount of collagen between groups 72 h after injury. This may be due to several factors, including the release of growth factors (TGF-β, IGF-I) and fibroblast proliferation beyond the expected time of the regeneration process, promoting balance in the amount of collagen observed later in the healing process. 23,51 The analysis of birefringence of fibrils/collagen fibers provides information about the alignment of collagen fibers, which provides tensile strength to the tendon allowing it to resist daily activities. 49 We found that there were higher optical delays for LLLT, and this suggests that LLLT stimulated and/or shielded collagen fibers. Wood et al. 49 observed an increase in optical delays after 6 days of laser irradiation compared with a no-treatment control group. Likewise, Oliveira et al. 51 found higher optical values after 7 days of laser irradiation compared with an untreated injury group.
It is claimed that laser acts on photoreceptor molecules (chromophores) of cytochrome c oxidase complex (Complex IV, cytochrome c oxidase), which is a transmembrane protein found in the mitochondria, playing an important role in energy metabolism. 52 –54 LLLT may stimulate the respiratory chain activity of cytochrome c oxidase, leading to an increase in oxygen consumption and ATP production, with the potential of modifying a variety of biological processes. 52 –54 Hayworth et al. 55 found a 30% increase in the activity of cytochrome c oxidase in the temporal muscle of healthy rats 24 h after a single irradiation of LLLT compared with a control group. Importantly, irradiation occurred in a healthy tissue, so values found after irradiation were higher than actual levels. It is possible that this mechanism observed in muscles also may be responsible for the protection of collagen fibers, although further studies are needed to confirm or refute our hypothesis. It is also plausible that LLLT stimulated the release of FGF, contributing to increased collagen deposition and reorganization of the damaged fibers. 23
Optical retardation data indicated better organization of collagen fibers in the diclofenac group compared with the untreated group, suggesting that diclofenac was effective in maintaining the structure of the tendon tissue in the first hours after injury, although at lower levels than LLLT. The effect of NSAIDs on the organization of collagen fibers through tissue birefringence has only been investigated in one study, 26 which found that indomethacin and celecoxib delayed the reorganization of collagen fibers after injury when compared with a no-treatment control. The untreated group showed the lowest optical delays until day 14, indicating structural disorganization at all of the preceding measurement time points. By day 21 collagen fibers were organized in the untreated group, and there were no differences when compared with treatment groups. It took 28 days for the collagen fibers of untreated tendons to reach similar levels to those observed for of the healthy group (i.e., full recovery of structural architecture).
Conclusions
We conclude that collagenase-induced tendinitis is a credible experimental model to produce tissue changes relevant to tendon injury, including plasma extravasation, inflammatory cell migration, and disorganization of tendon morphology. Our study demonstrates for the first time that a long period of time is required for collagen fibers of an untreated group to reorganize following injury of the Achilles tendon, and that diclofenac and dexamethasone delayed reorganization of collagen fibers. Our results show that 810 nm LLLT at a dose of 3 J was more effective than diclofenac and dexamethasone in reducing early inflammatory markers. LLLT promoted an increase in the amount of collagen in the early stages of the repair process, and protected the organization of the collagen fibers in the injured area, suggesting it is the better treatment option for tendinitis. LLLT is a low-cost and noninvasive modality without any serious side effects.
Footnotes
Acknowledgments
The authors would like to thank MSc Patrícia Almeida Silva for technical assistance. The authors would like to thank FAPESP—Fundação de Amparo à Pesquisa do Estado de São Paulo Grants 2011/18330-1. I.F.N. is a PhD candidate at the Department of Global Public Health and Primary Care at the University of Bergen, funded by the The Norwegian Fund for Postgraduate Training in Physiotherapy.
Author Disclosure Statement
No competing financial interests exist.