
Abstract
Introduction
T
As transurethral resection of the prostate (TURP) is considered the gold standard of surgical treatment of BPH, 3 there are reports of using this method in patients on anticoagulants or antiplatelet drugs. Parr et al. 4 performed TURP on 13 patients on ongoing anticoagulation with coumarin derivatives. There was a need for blood transfusions after the procedure in 30% of patients and for plasma transfusions in over half of the patients. Chakravarti and MacDermott 5 decided to change from anticoagulants to low-molecular-weight heparin (LMWH) 2 days before performing TURP on 11 patients. Despite this, one patient required a blood transfusion and prolonged hematuria appeared in 27% of patients, with some patients requiring rehospitalization. Similar results were found in the study of Dotan et al. 6 who performed TURP on 20 patients after stopping warfarin and using LMWH as a bridging therapy. Four patients (20%) required blood transfusions, and in two patients (10%) there was a need for recatheterization due to hematuria. These observations on rather small groups of patients were confirmed by a multicenter French trial comparing TURP in 206 patients on anticoagulants and antiplatelet drugs, with 406 patients not taking these drugs. 7 In the first group, there was a higher blood transfusion rate (1.9% vs. 1.0%), higher clot retention rate (13% vs. 4.7%), longer hospitalization time (6.4 days vs. 4.7 days), and a higher rate of late hematuria (15% vs. 8.4%).
There is a continuous search for a safer and equally effective procedure to replace TURP. One of the more promising methods is photoselective vaporization of the prostate (PVP) with the use of the GreenLight laser. Its unique hemostatic properties depend on the wavelength of 532 nm, which goes through water without loss of energy and is selectively absorbed by hemoglobin. This virtually bloodless procedure seems to be a perfect modality for patients at a high risk of bleeding, including those on anticoagulation. In this study, we evaluated the safety and effectiveness of PVP in the treatment of patients with BPH on anticoagulant or antiplatelet therapy.
Materials and Methods
A total of 109 patients underwent PVP with the use of the GreenLight HPS 120 W laser between 2009 and 2012. All procedures were performed by two surgeons (G.P. and H.Z.). Sixty-five (59.6%) patients were on anticoagulants or antiplatelet drugs due to cardiac and/or neurological disorders (group A), and 44 (40.4%) patients did not take any of these drugs (group B). In group A, 37 patients took acetylsalicylic acid (ASA 75–150 mg) and 28 patients took acenocoumarol. Acenocoumarol was discontinued 5 days before the procedure and replaced with LMWH until the third day after PVP. ASA was not discontinued.
Indications for anticoagulant/antiplatelet drugs are shown in Table 1.
Some patients had two or more conditions requiring anticoagulants or antiplatelet drugs.
Both groups were comparable according to preoperative clinical parameters: LUTS as described by the International Prostate Syndrome Score (IPSS), Quality of Life (QoL), uroflowmetry parameters—maximum urinary flow rate (Qmax), postvoid residual volume (PVR), and preoperative blood parameters [prostate-specific antigen (PSA), morphology, and biochemistry].
All patients with elevated PSA or suspicion of cancer on digital rectal examinations underwent biopsy—only patients without prostate cancer were included in the study. Only patients with negative urine culture were qualified for surgery. Patients were admitted to the department 1 day before the surgery and underwent routine preoperative evaluations. PVP was carried out with the use of the GreenLight HPS 120 W system (American Medical Systems, Inc., Minnetonka, MN)—532-nm wavelength laser with LBO (lithium triborate) crystal. Side-firing laser fiber (10–2090) was inserted through a separate channel of a continuous flow 21Ch cystoscope (Richard Wolf, Germany) with 0.9% saline for irrigation. We used antibacterial prophylaxis with 200 mg of ciprofloxacin intravenous preoperatively and 500 mg p.o. twice daily for 5 days postoperatively.
During hospitalization, we evaluated the time of the procedure, lasing time, the amount of energy used, the time of catheterization, the time of hospitalization, biochemistry and morphology parameters, and intra- and postoperative complications. Patients were evaluated at 1, 3, 6, 12 months, and 3 and 5 years after hospitalization. During follow-up examinations, an IPSS/QoL questionnaire was completed, uroflowmetry, PSA, and urine tests were performed, and potential complications were evaluated. The follow-up schedule is shown in Table 2.
IPSS, International Prostate Syndrome Score; PSA, prostate-specific antigen; PVP, photoselective vaporization of the prostate; PVR, postvoid residual volume; Qmax, uroflowmetry; QoL, quality of life.
All data were collected in a database and subjected to statistical analysis using Statistica software. Variables were presented as mean ± standard deviation. All pre- and postoperative parameters were analyzed for statistically significant differences using the Mann–Whitney U test. To evaluate the influence of anticoagulant therapy on complications, the risk χ 2 (chi-squared) test was used, and relative risk as well as an odds ratio were determined. A p value of <0.05 was considered statistically significant.
Results
Baseline characteristics of both groups are shown in Table 3. In group A, 8 out of 65 patients (12.3%) and 6 out of 44 patients (13.6%) in group B were catheterized due to acute urinary retention before surgery. No statistical difference was found in any of the preoperative parameters.
IPSS, International Prostate Syndrome Score; PSA, prostate-specific antigen; PVR, postvoid residual volume; Qmax, uroflowmetry; QoL, quality of life.
Operation time was 56.0 ± 10.4 min in group A, and 54.2 ± 13.5 min in group B. (p = 0.217). Lasing time was 30.2 ± 6.7 and 29.3 ± 7.0 min in groups A and B, respectively (p = 0.734). Laser energy used was 196,340 ± 43.9 J in group A, and 191,652 ± 46.2 J in group B (p = 0.708). No statistically significant difference was found in these parameters between both groups.
No intraoperative complication was observed during procedures. There was no significant bleeding in any of the groups.
In the early postoperative period (on the day of the procedure), the blood parameters were evaluated. Hemoglobin concentration was 13.04 ± 0.68 and 13.21 ± 0.62 g/L before the procedure and 12.86 ± 0.75 and 12.94 ± 0.57 g/L after the procedure in groups A and B, respectively, whereas a decrease of hemoglobin was higher in group B (0.27 ± 0.25 vs. 0.17 ± 0.30 g/dL. p = 0.01). There was a statistical difference between the groups, but it was clinically irrelevant as no significant bleeding after the procedure was observed and no patient required a blood transfusion.
Sodium concentration was 139.8 ± 2.49 and 139.7 ± 2.41 mmol/L before the procedure, and 139.63 ± 1.98 and 139.56 ± 2.12 mmol/L after the procedure in groups A and B, respectively. No significant difference was found in this parameter.
Mean catheterization time was 18.49 ± 7.77 h in group A, and 18.29 ± 6.21 h in group B (p = 0.511). In two patients in each group, no catheter was inserted after the procedure. Two patients from group A and one patient from group B needed to be recatheterized after catheter removal because of urinary retention. However, all three patients were discharged without a catheter as there was no significant postvoid residual after the second removal of the catheter. Mean hospitalization time after the procedure was 28.43 ± 7.55 h in group A, and 29.11 ± 7.32 h in group B (p = 0.497). There was no statistically significant difference in the catheterization and hospitalization time between both groups.
Follow-up—effectiveness evaluation
During follow-up examinations, the IPSS/QoL questionnaire was completed, uroflowmetry, PSA, urine tests were performed and potential complications were evaluated.
Improvement of IPSS and QoL scores as well as Qmax and PVR was found in both groups. IPSS values are shown in Table 4 and Fig. 1, QoL values in Table 5 and Fig. 2, Qmax values in Table 6 and Fig. 3, and PVR values in Table 7 and Fig. 4. No statistically significant difference between the groups in these subjective and objective parameters was shown.
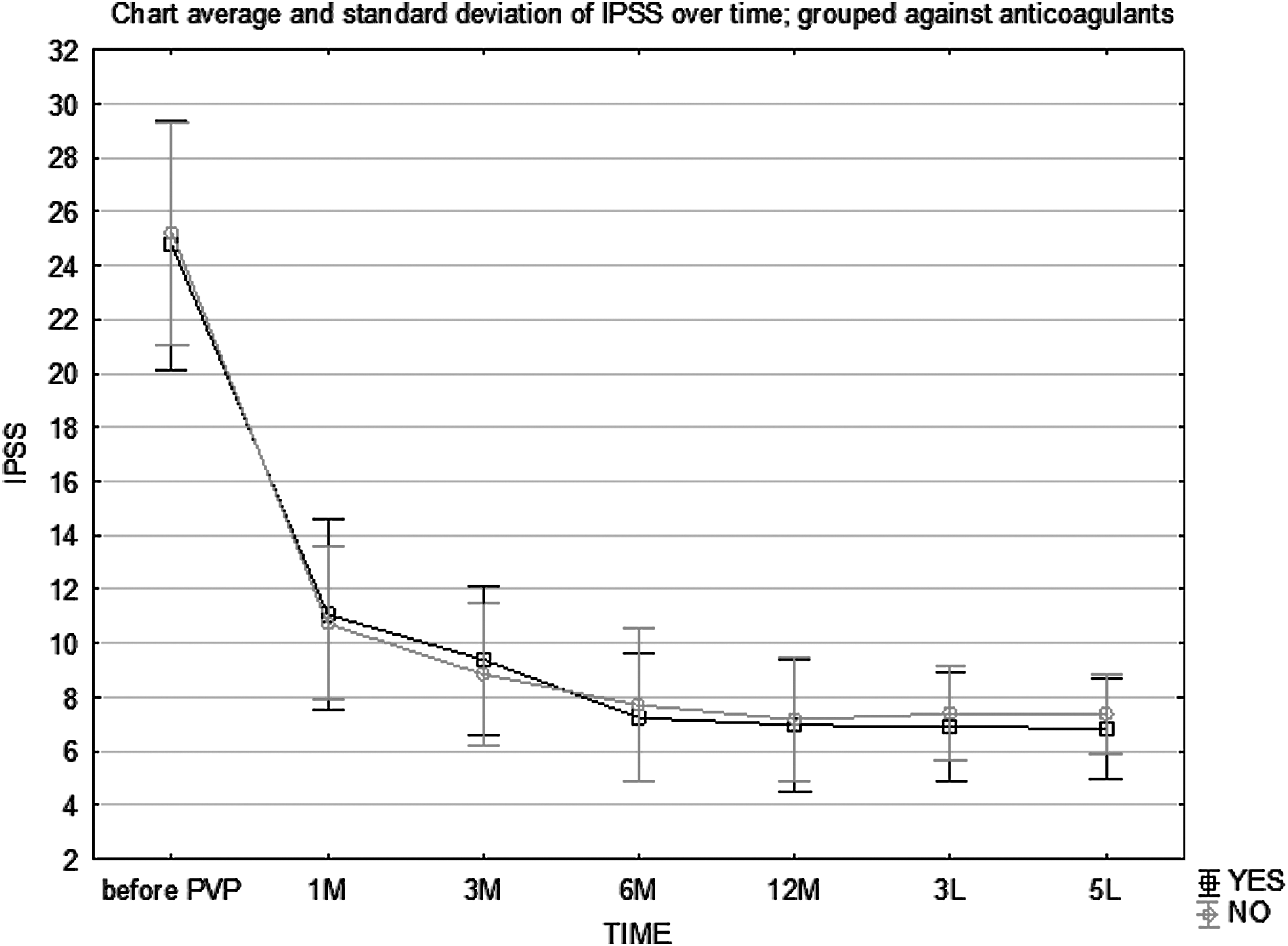
Follow-up—IPSS. IPSS, International Prostate Syndrome Score.
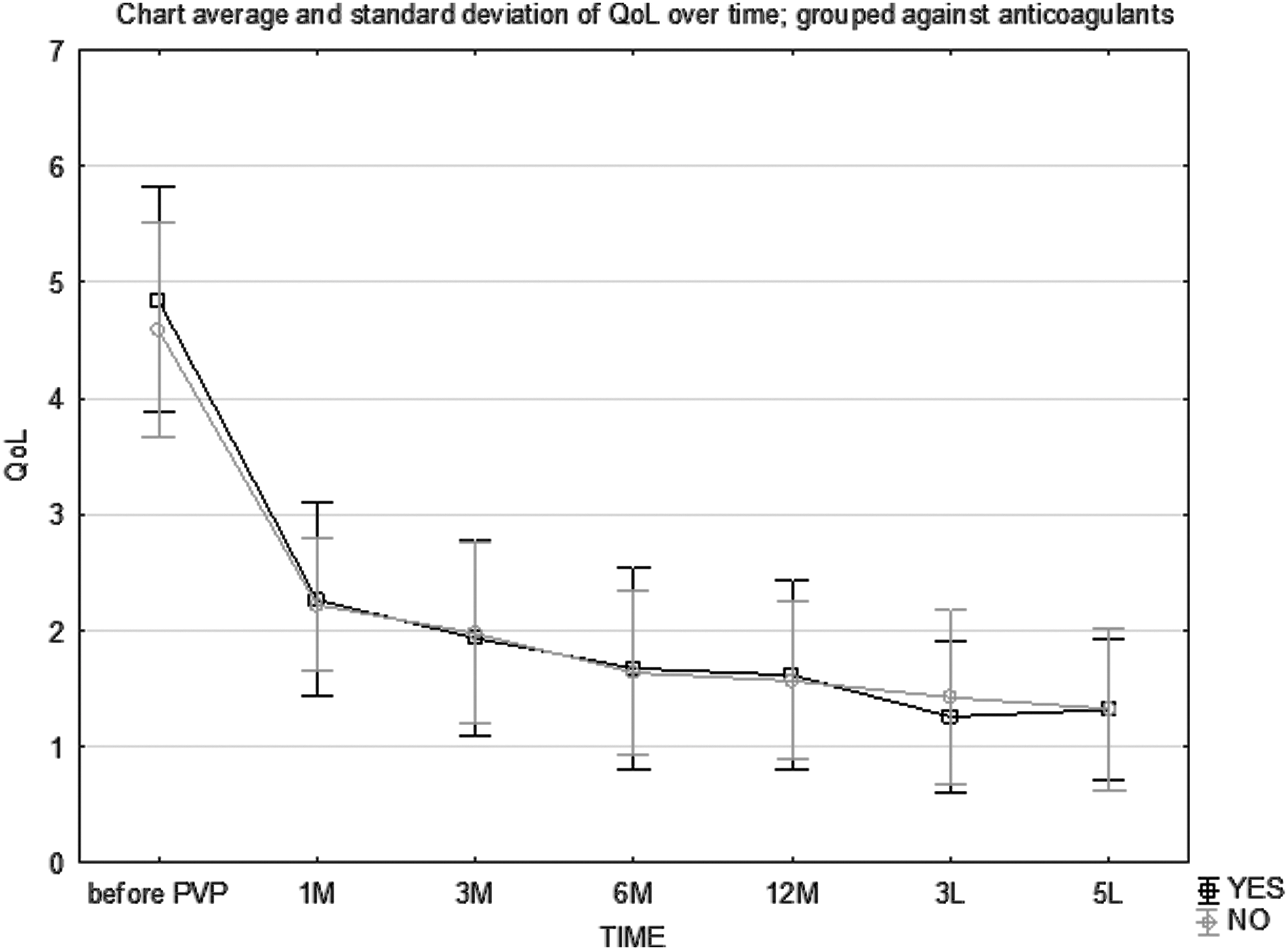
Follow-up—QoL. QoL, quality of life.
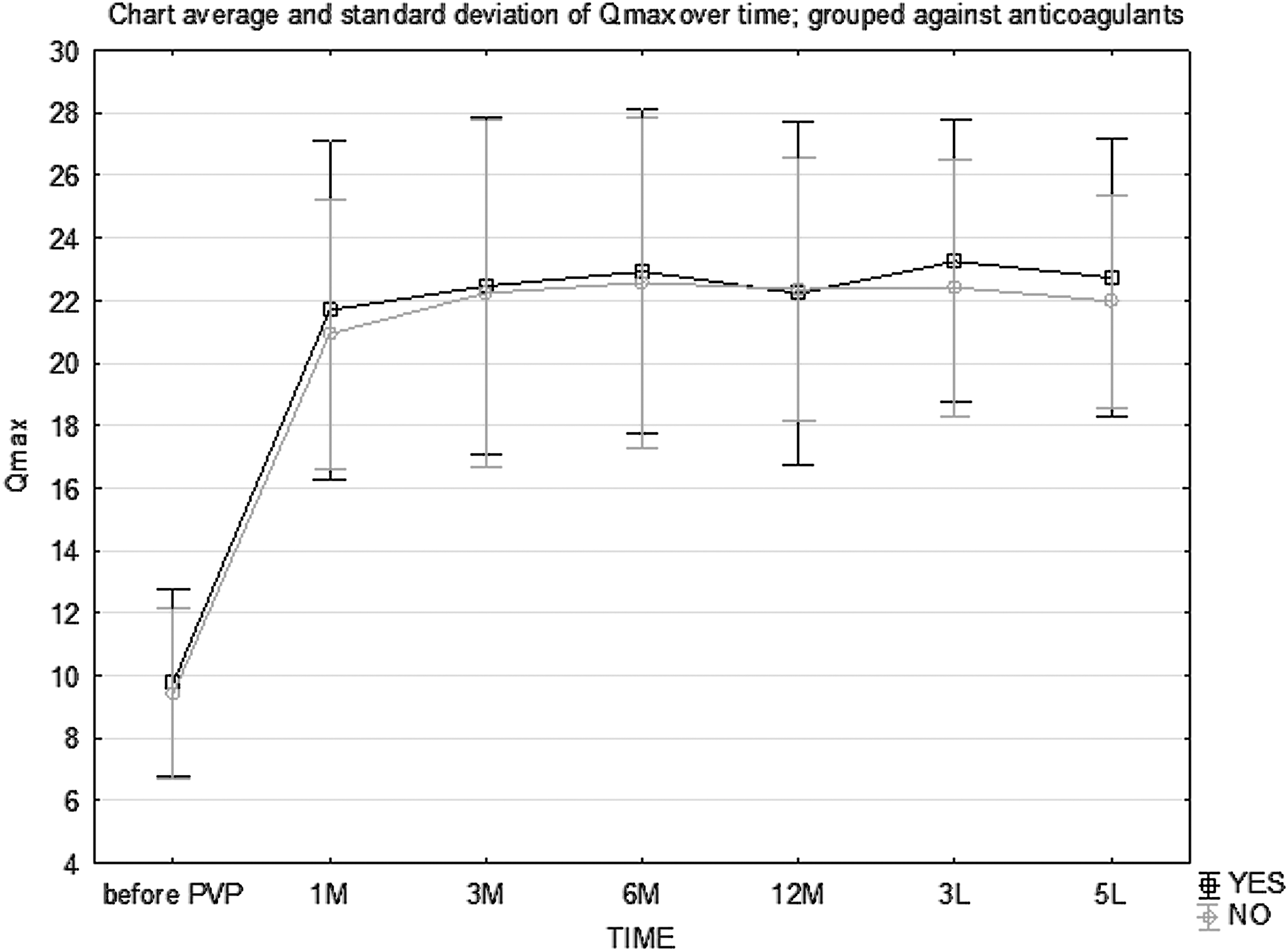
Follow-up—Qmax. Qmax, uroflowmetry parameters—maximum urinary flow rate.
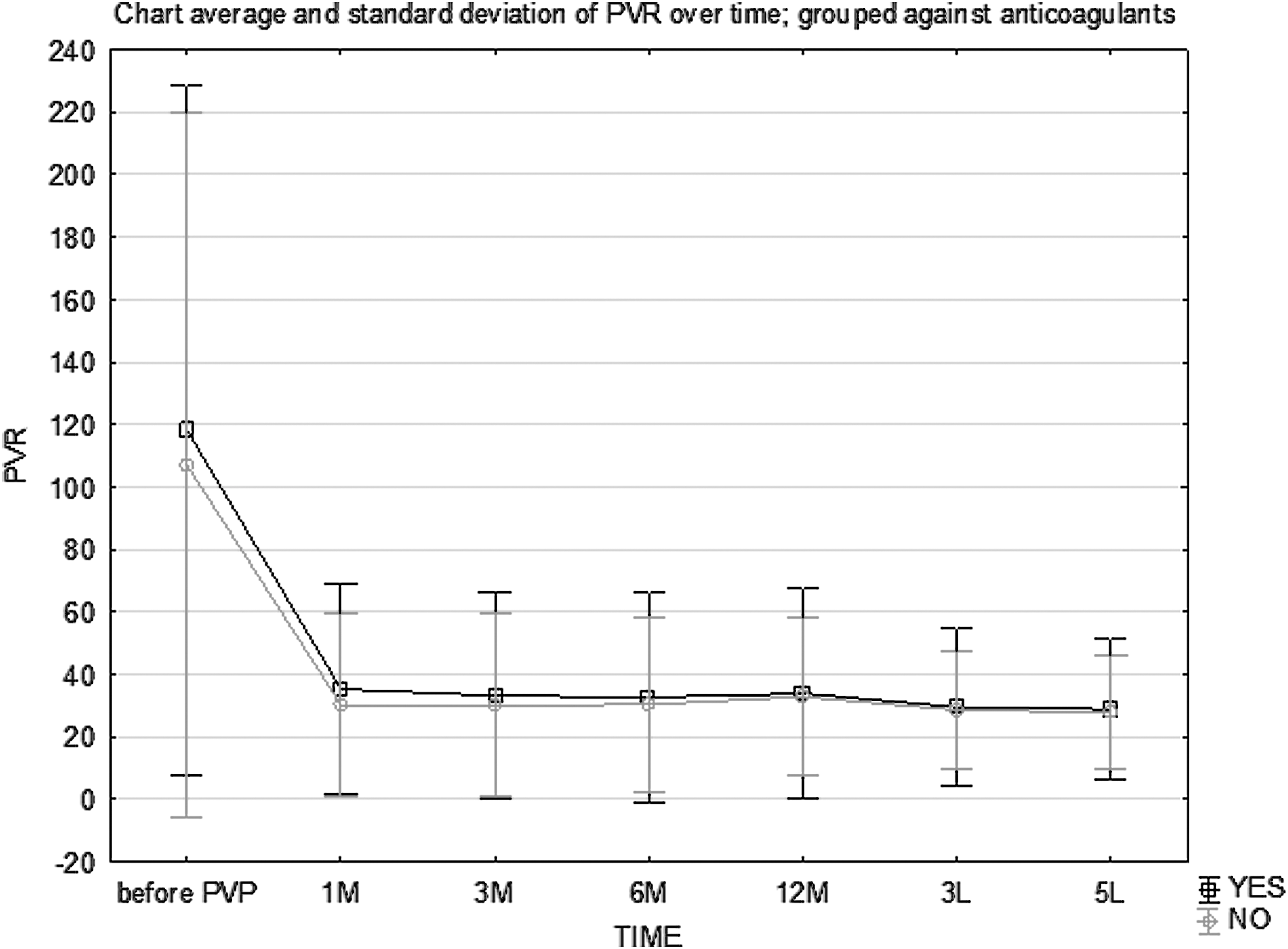
Follow-up—PVR. PVR, postvoid residual volume.
IPSS, International Prostate Syndrome Score; PVP, photoselective vaporization of the prostate.
PVP, photoselective vaporization of the prostate; QoL, quality of life.
PVP, photoselective vaporization of the prostate; Qmax, uroflowmetry.
PVP, photoselective vaporization of the prostate; PVR, postvoid residual volume.
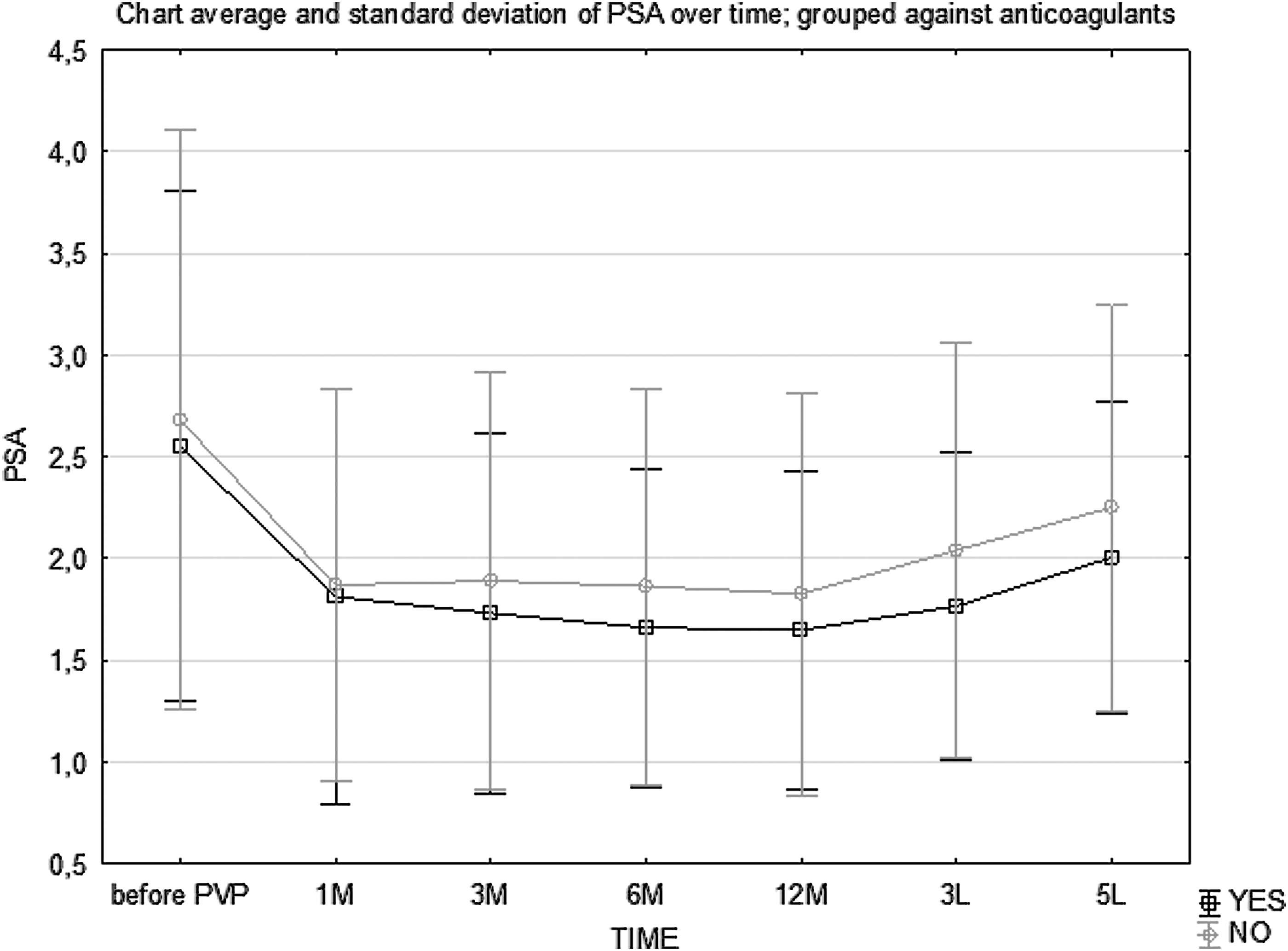
One of the important blood parameters with clinical implications is PSA. Of course, it is of great value in separating the group of patients with prostate cancer, and additionally, in the follow-up period, it may be a good surrogate of the amount of tissue removed during PVP. PSA values are shown in Table 8 and in Fig. 5. In both groups, PSA has decreased over 30% after PVP in the first year of follow-up. In the following years, PSA increase was observed, being 17–22% lower after 5 years compared with preoperative values. No statistically significant difference between the groups in PSA concentration was shown.
Follow-up—PSA. PSA, prostate-specific antigen.
PSA, prostate-specific antigen; PVP, photoselective vaporization of the prostate.
According to the presented results, there was no statistically significant difference in all analyzed efficacy parameters.
Follow-up—complications
In the follow-up period, early and late complication rates in both groups were evaluated. The most frequent complication was retrograde ejaculation. In group A, it was found in 10 out of 26 sexually active patients (38.46%) 1 month after PVP, and in group B, in 9 out of 20 sexually active patients (45%). During the first year of follow-up, the retrograde ejaculation rate showed a slight downward trend, and then it was stable as shown in Table 9. No significant difference between the two groups in the occurrence of retrograde ejaculation was found.
ARR, absolute risk reduction; CI, confidence interval; OR, odds ratio; PVP, photoselective vaporization of the prostate; RR, relative risk.
In most of the patients in the first days after PVP, mild dysuria and hematuria appeared. Only in a few patients these symptoms lasted longer. Hematuria and dysuria rates are shown in Tables 10 and 11.
ARR, absolute risk reduction; CI, confidence interval; OR, odds ratio; PVP, photoselective vaporization of the prostate; RR, relative risk.
ARR, absolute risk reduction; CI, confidence interval; OR, odds ratio; PVP, photoselective vaporization of the prostate; RR, relative risk.
Most of the urine cultures during follow-up were negative. Rates of bacteriologically proven urinary tract infections in both groups are shown in Table 12.
ARR, absolute risk reduction; CI, confidence interval; OR, odds ratio; PVP, photoselective vaporization of the prostate; RR, relative risk.
In one patient in group A, Enterococcus faecalis was detected. In all remaining cases of UTI, the underlying factor was Escherichia coli.
In one patient in group A and in three patients in group B, PSA was found to be elevated during follow-up. These patients underwent biopsy and in three of them no carcinomatous tissue was detected. In one patient in group B, prostate cancer (Gleason 6) was found 3 years after PVP. This patient was qualified for radical prostatectomy and underwent surgical treatment with good results.
In one patient in group A and in one patient in group B, urethral stricture was diagnosed after 11 and 5 months, respectively. Both patients underwent an urethrotomy with no complications. One patient in group A and two patients in group B were qualified for reoperation during follow-up due to recurrent LUTS and bladder outlet obstruction. In group A, one patient's second PVP was performed after 10 months, and in group B, in two patients TURP was performed 1 and 2 years after PVP, respectively. All surgical retreatments are shown in Table 13.
PVP, photoselective vaporization of the prostate; TURP, transurethral resection of the prostate.
During 5 years of follow-up, four patients died, two in each group. Two patients died of heart infarct, one from a brain stroke, and one from colon cancer. None of the deaths was associated with the surgical procedure. Seventy-five out of 109 patients (68.8%) completed the 5-year follow-up.
Based on statistical analysis, no significant difference between the groups in the complication rates was shown.
Discussion
The decision of qualifying a patient with BPH for surgical therapy is nowadays delayed by the use of medical therapy. This is the reason why transurethral procedures are performed in patients with more comorbidities, often requiring anticoagulants or platelet aggregation inhibitors. As ongoing anticoagulant therapy is a contraindication for TURP because of the increased risk of bleeding, 4 bridging therapy with intravenous heparin is the most common strategy in this group of patients. Nevertheless, even this cautious approach does not prevent important bleeding complications. 5,6 Development of the GreenLight laser (KTP/LBO) with its unique hemostatic properties gave hope to avoid these complications in patients who were often disqualified from other methods of surgical treatment of BPH.
The GreenLight HPS laser is a 532-nm wavelength laser, created by passing the 1064-nm (Nd:YAG) laser energy through an LBO (lithium triborate) crystal instead of the previously used 80 W machine KTP (potassium-titanyl-phosphate) crystal. It has a high absorption affinity for oxyhemoglobin and a low absorption affinity for the aqueous irrigant fluid. As a result, it vaporizes adenomatous prostate tissue effectively with only a thin coagulation zone.
Efficacy of PVP was shown in many studies, including all generations of the GreenLight laser (80, 120, and 180 W). 8 –13 The technique was also compared with the “gold standard”—TURP in several randomized controlled trials. 14 –18 All of the studies confirmed the similar efficacy of these two methods with lower complication rates in favor of PVP.
Some authors focused on the group of high-risk patients, including those on anticoagulant or antiplatelet therapy. Early experience with the 80 W KTP laser was presented by Reich et al. 19 who performed PVP in 66 high-risk patients (26 on anticoagulants, 3 with bleeding disorders). There was no important intra- and postoperative complications with satisfactory objective and subjective results. This was subsequently confirmed by Sandhu et al. 20 in the group of 24 patients taking warfarin, clopidogrel, and ASA, and by Ruszat et al. in the group of 116 patients on coumarin derivatives, clopidogrel, and ASA. 21 A large series of 162 patients on oral anticoagulation undergoing PVP using 80 and 120 W lasers with 2 years of follow-up presented by Chung at al. 22 included patients on two or more anticoagulation agents. They found no significant complication, but delayed bleeding in six (4%) patients, three of which required a blood transfusion.
In our study, we tried to evaluate the long-term efficacy and safety of PVP with the 120 W GreenLight laser in patients on anticoagulation and antiplatelet therapy. To our knowledge, our study is one of few with such a long observation period in this special group of patients, as every one of them had a chance to complete a 5-year follow-up schedule.
In both groups, the procedure was performed safely as no intraoperative complications occurred. One could expect a greater chance of bleeding in the anticoagulated patients but we did not find any difference between the groups in bleeding rates. Surprisingly, a change of hemoglobin level was higher in the no-anticoagulant group, but it was clinically insignificant as it decreased only by 0.27 g/L and no patient required a blood transfusion. Hemostatic properties of 532 nm wavelength reduce the risk of bleeding even in patients on anticoagulants as it was reported before. 22 –24
We found no evidence of electrolyte disorders, thus no TUR syndrome occurred in any of the groups. It is the use of 0.9% saline solution for irrigation that decreases the risk of this life-threatening complication. Operative times as well as other preoperative parameters were similar in both groups and most of our patients were discharged on the next day after the procedure. Some authors, including one of the inventors of the procedure, Malek et al., 8 performed PVP on an outpatient basis. We believe this is possible only in patients without comorbidities and sometimes is related to the local financial policies, rather than medical indications.
Mild hematuria is often found after urologic endoscopic procedures. After PVP, it was reported by 0–12% patients 15,16,22 –24 and rarely required intervention. In our patients mild hematuria occurred in most cases during the first days after the procedure, but it was transient and not clinically significant. After 1 month it was reported by 16–17% patients and after 3 months by 3–5%, with no difference between the studied groups. The incidence of hematuria was higher in our patients, but it was not clinically significant as none of them required intervention or a blood transfusion. In our experience, delayed bleeding is most often found in patients who did not obey postdischarge indications and undertook heavy physical activity too early.
The other common symptom immediately after surgery was dysuria but, just like hematuria, it was mild, temporary, and did not influence the QoL significantly. The rates of dysuria after 1 month were similar between the groups, and they were reported by 10–11% of patients. Three months after the procedure, these symptoms were found in less than 5% of patients, and in the longer follow-up they were scarce.
The most frequent complication was retrograde ejaculation. It was reported by 38–45% of sexually active patients in the early postoperative period and diminished during the follow-up down to 20–25% after 3–5 years. The incidence of retrograde ejaculation in previous studies differs from 8 up to 70%, 8,25 –28 and it is less when compared with TURP. The reason for the ejaculation preserving the character of PVP is not well explained. Malek et al. 8 suggested that the regeneration of muscular fibers of the bladder neck plays a role in this phenomenon, but it was not proven until now.
One of the major issues in our study was the long-term outcomes. Both of the studied groups revealed promising early results which were sustained during the follow-up period. Both objective and subjective voiding parameters (IPSS, QoL, Qmax, and PVR) remained favorable after 5 years. This confirms Malek et al.'s observation in 94 patients treated by 60 and 80 W lasers 8 as well as Cho et al.'s results in 68 patients operated with the use of 120 W. 11
An interesting observation is the relationship between efficacy parameters and PSA level. In our study, we decided not to measure prostate volume and instead use PSA as a surrogate. The nadir of mean PSA in both our groups was noted 12 months after the procedure (36% reduction in the group on anticoagulants, 32% in the other group). Then we observed an upward trend of the mean PSA during the next years of follow-up. Most of the previous studies on PVP with a 120 W laser reported a similar reduction of PSA values. Al-Ansari et al. showed PSA reduction of 40% after 1 month and 50% after 6 months after the procedure. Then the PSA increased, being 60% of the baseline value after 3 years. 14 There was an interesting finding in Tasci et al.'s study 10 as there was a decrease of the PSA by 25% 12 months after PVP, and it returned to the baseline values after the following year. Even still, objective and subjective efficacy parameters remained favorable. This confirms our conclusion that regardless of prostate size and PSA values, the most important outcome is described by functional parameters.
Obviously, the development of the more powerful GreenLight XPS (180 W) laser made faster tissue vaporization possible and the results of the GOLIATH trial revealed greater reductions of PSA in the follow-up period: after 2 years the mean PSA level was 50% lower than the baseline value. 29 Longer follow-up is needed to evaluate the influence of laser power on the durability of functional results.
The need for repeated interventions in patients after PVP is an issue often raised. In the first long-term observation study of 94 patients presented by Malek et al., 8 no patient required reoperation during the follow-up period, apart from two patients with soft bladder neck contractures treated by simple dilation. These encouraging results may be biased by the small baseline prostate volume (mean 45 mL). In the larger series of 246 patients treated by the 80 W laser published by Hai, 9 there was an 8.9% retreatment rate in 5 years, mainly due to regrowth of the adenoma and bladder neck contracture.
In the following trials with the next-generation laser of the GreenLight laser (120 W), 10,14,30 even higher reintervention rates (10–18%) were reported. Gained experience and encouraging results led urologists to operate on patients with larger prostates, even over 80–100 mL, making higher risks of adenoma regrowth inevitable. 10 Our study revealed an overall surgical retreatment rate of 5% during the 5-year follow-up, and we found no significant difference between the studied groups. Regrowth of adenoma was the indication for the repeated surgery in three patients, and urethral stricture, in two. No bladder neck contraction was diagnosed. In the GOLIATH study with the 180 W XPS laser, a 2-year reintervention rate of 9% was reported. 29 The authors anticipate, based on previous reports, that beneficial clinical outcomes will be prevalent after following years of observation.
Since the introduction of the GreenLight laser, some authors have stated that a potential drawback of PVP could be the absence of tissue for pathologic analysis. 31 However, in the PSA era, the detection rate of incidental cancer in surgical treatment for BPH has lowered and clinically significant diseases are found very rarely. 32 In our group, there was only one patient diagnosed with prostate cancer during the follow-up period and he was successfully treated by radical prostatectomy. This confirms previous observations 8 that a careful postoperative follow-up regimen is sufficient for not overlooking clinically significant prostate cancer.
The EAU Guidelines Panel 3 approves the position of laser vaporization as the best treatment option for patients on anticoagulant therapy. Our results also confirmed the efficacy and safety of the PVP with the GreenLight laser in this group of patients.
We are aware of the certain limitations of our study. One of these limitations is that it was nonrandomized in nature. Moreover, it has not included patients on other anticoagulant and antiplatelet medications (e.g., warfarin, clopidogrel, rivaroxaban, and dabigatran) as they were not as popular during the time of the study as they are now. In addition, the sexual function was not methodically assessed, only data on retrograde ejaculation were collected.
Conclusions
Our results demonstrate that high-power (120 W) photoselective laser vaporization is an effective and safe option of surgical treatment for bladder outlet obstruction due to BPH in patients on anticoagulation and antiplatelet therapy. The risk of early and late complications is acceptable, and good functional results are sustained during long-term follow-up. As the procedure is still developing, not only by the introduction of the more powerful (180 W) XPS laser together with more durable fiber (Moxy), but also by the implementation of different operative techniques such as vapo-enucleation, more clinical trials are needed to evaluate this procedure.
Footnotes
Author Disclosure Statement
No competing financial interests exist.