
Abstract
Introduction
T
The technology was developed to reduce risks encountered with traditional nonfractional ablative or nonablative laser treatments, and has proved its effectiveness and safety in various dermatological conditions, including surgical and acne scars. 7 In this context, we decided to investigate the efficacy of the 1550-nm nonablative laser fractional photothermolysis to treat scars.
Case Report
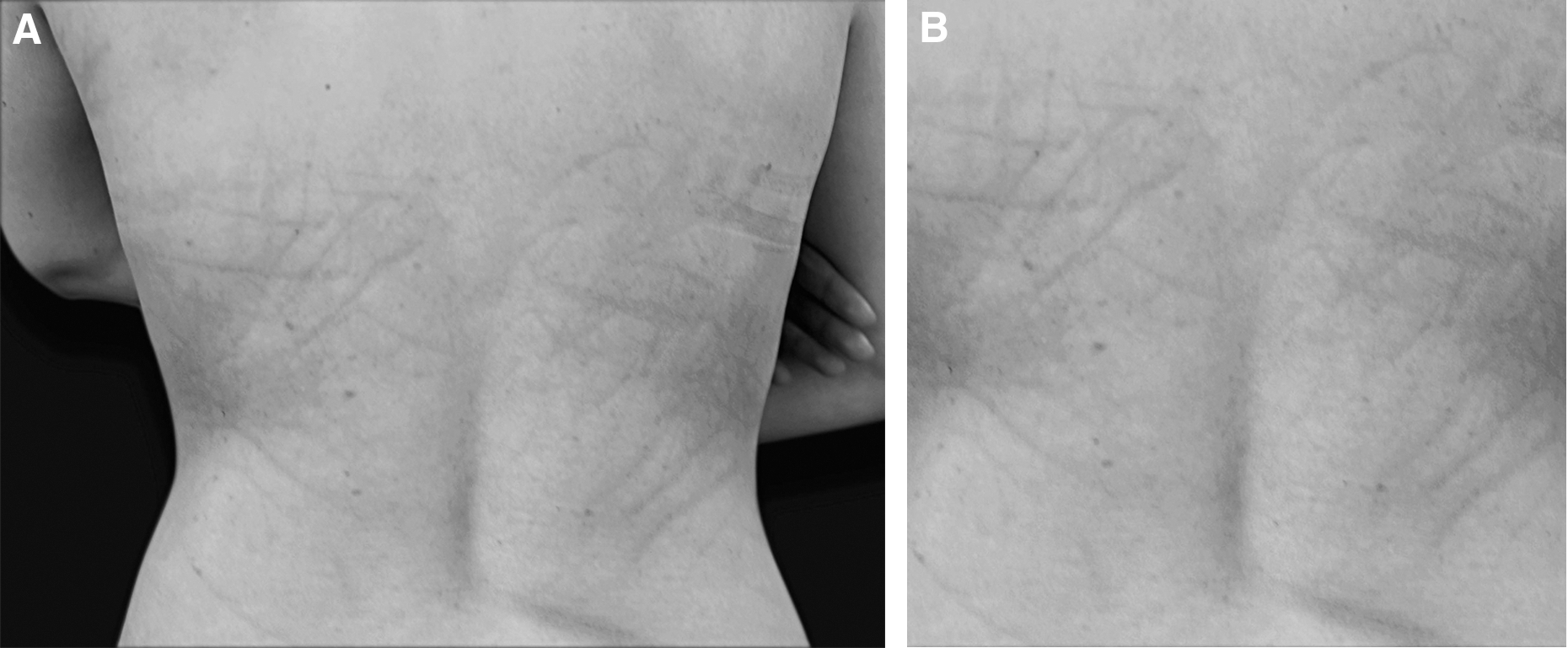
A 27-year-old white woman with multiple scars on her back underwent consultation for laser resurfacing options in our practice (Fig. 1A and B). The woman, with Fitzpatrick skin type II, developed these peculiar scars after getting whipped at an age of 10, and denied any previous treatments.
(
The patient received nonablative fractional resurfacing treatments with a laser device (Fraxel SR1500 RE:Store; Solta Medical, Hayward, CA) after signing informed consent.
Treatment settings had a fluence of 20 mJ/cm2 and 1500 microthermal zones/cm2 density, with full surface area coverage and eight passes. The total laser time for the dorsal area irradiated was about 15–20 min.
The use of patented scanning technique ensures uniformity of treatment zones using an irradiation head/beam diameter in a single handpiece up to 1.4 mm (1400 μm). A 1-month interval was made between treatments. A total of four treatments were administered. A 5% emulsion preparation, containing 2.5% each of lidocaine/prilocaine (Emla® cream; APP Pharmaceuticals), was given as local anesthesia before laser treatments. During treatments, skin was cooled with a skin cooling system (Zimmer cooler).
After treatment, a moisturizer was applied over the area twice daily. Adverse effects included mild swelling for 2 days and erythema for 2–5 days after each session of treatment. Initial reactions to treatment were minimal oedema, which was resolved within 4 days, and small crust formation on the treated areas; she also reported some mild pain and a burning sensation with mild oedema. The microcrust formation typically occurred for 1 week with it disappearing gradually. The patient experienced skin dryness and a sensation of itching, but no additional treatment was required apart from humectants. No postinflammatory hyperpigmentation was observed.
The patient was followed at 3 and 6 months and for a short-term follow-up.
Discussion
Scars are areas of fibrous tissue that replace normal skin after injury. A scar results from the biological process of wound repair in the skin and other tissues of the body, as in the case of our patient, where psychological factors also played important roles. Treatment for scars includes surgical revision, laser treatments, dermabrasion, chemical peelings, and topical treatment with bleaching creams and/or retinoids. Interestingly, comparisons among chemical peels, dermabrasion, and laser resurfacing revealed that laser resurfacing was more easily controlled as a treatment method. Scar treatment with ablative lasers has become increasingly popular. However, ablative technology such as carbon dioxide and Er:YAG lasers is associated with long recovery or “downtime.” 1
Fractional photothermolysis has been recently introduced; the Food and Drug Administration has approved the Fraxel SR Laser System for improvement of skin texture, laxity, treatment of digital cutis laxa, rhinophyma, melasma, pigmentation, acne scarring, and atrophic scars as well as surgical scars and depressed alar scars after surgery. Carbon dioxide (CO2) and Er:YAG ablative lasers were previously considered the gold standard; however, after fractional resurfacing was introduced, fractional lasers became the most used due to decreased recovery time and risk of adverse events. 8 The introduction of fractional lasers offered increased safety while maintaining high efficacy. An additional benefit is that darker Fitzpatrick skin types IV and V could be safely treated. 9,10 This 1550-nm laser creates microthermal zones of “injury” in the skin. Within these areas, localized epidermal necrosis occurs alongside collagen denaturation. Secondary to treatment, necrotic debris is eliminated and new collagen is built. In addition, as this laser treatment is nonablative, the healing process is faster. 1 Considering literature and previous reports that suggest encouraging improvement in atrophic and acne scars, we decided to treat this particular type of scar. To maximize treatment results, when the ideal number of treatments to address scars is unknown, most studies recommend three to five treatments during a month as multiple treatments are often completed. 1
Within this study, there were four treatments chosen for this study protocol.
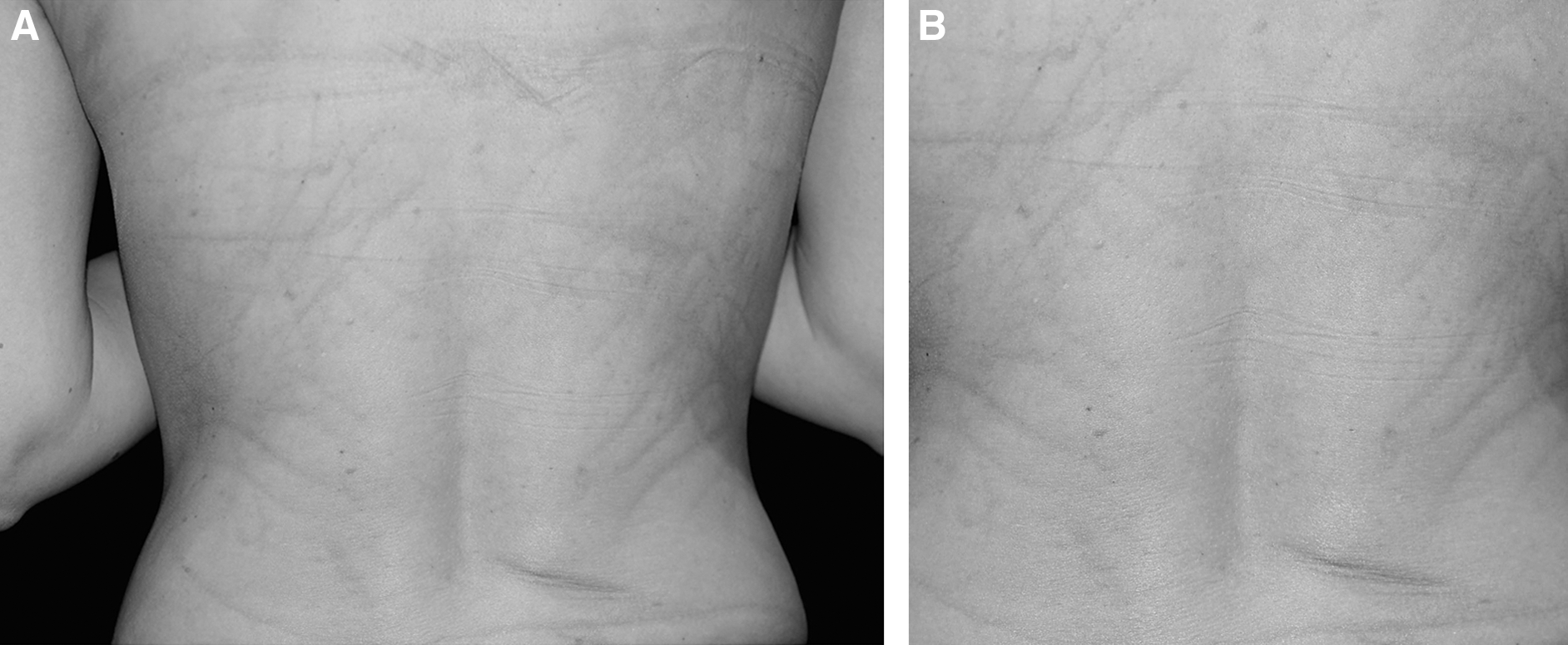
Improvement degree may depend on patients' intrinsic ability to remodel collagen and may be related to factors such as age, skin quality, genetics, and smoking behavior. 7 In this case, after four treatments, significant improvement in color match of the scar and improved aesthetic outcome of the scars were shown (Fig. 2A and B). Although this case can be considered as a first step to assess efficacy of the nonablative laser technique as for scars induced by lacerated and contused wounds, further studies with a large cohort of patients and a longer follow-up period could help in evaluating the long-term benefit of this promising scar treatment.
(
Conclusions
Use of fractional photothermolysis is demonstrated by this preliminary data and suggests improved aesthetic results, through this scar revision technique.
Nonablative fractional photothermolysis may be considered a first-line treatment for cutaneous scars, based on the clinical efficacy and excellent side effect profile in a wide range of skin types. As of this writing, no published reports compare this treatment with traditional ablative lasers or ablative fractional devices.
Footnotes
Author Disclosure Statement
No competing financial interests exist.