
Abstract
Introduction
P
During root canal treatment and prosthetic post placement, preparation with rotary instruments leads to the formation of smear layer and its interaction with cementing agents has been extensively discussed. 12,13 The presence of a smear layer can cause the dentin tubules obliteration and, consequently, a decrease on the cement adhesion to the dentin 11,12,14 and its removal is a controversial concern for both final endodontic sealing and prosthetic procedures. 2,14 –21 Clinical procedures may also leave residues or contaminants that interfere on the bond strength, such as cement excess from previous root canal treatments, acrylic resin and lubricants inside the root conduct used for post molding, temporary cement and reminiscent post material, and salivary contamination, among others. 9,22 The maximum removal of these residues or contaminants from the root canal before the post placement considerably enhances its retention. 11 –13,15 –17 Thus, a debridement procedure of the post-prepared cavity should be performed before cementation. 15,21
Another important issue is the presence of bacterial contamination during the post placement. If there is a mature biofilm within the root canal it may be trapped between the resin cement and the dental root canal impairing the post retention. 22,23
The comparison of pressure alterations device, 24 ultrasonic systems, 18,24 and laser devices 25,26 for cleaning the root canals have been explored and, among these, the laser presented the best performance on debris removal. 11,27 –30 The use of Er:YAG (@ 2940 nm) and Nd:YAG (@ 1064 nm) lasers increase the bond strength of cements to dentin. 11 Moreover, these lasers show the capability to remove the smear layer without heating the surrounding tissues. 31 –33 Irradiation with Nd:YAG and Er:YAG has optimized the results of endodontic therapy, particularly in acting on microorganisms resistant to the conventional antimicrobial agents, 28,34 thereby reducing the risk of undesirable refractory infections. High-intensity lasers at infrared spectral range can lead to microbial reduction due to the high temperatures generated by laser absorption in the inner surface of the intracanal dentine. 28,34,35 While Er:YAG and Er,Cr:YSGG cause ablation, Nd:YAG and high-intensity diode lasers can melt the dentine, leading to the microbial reduction and apical marginal sealing, enabling the tooth to properly return to its specific functions after endodontic and prosthodontic treatments. 28,34 –37 Unlike the increase on bond strength of adhesive cements to dentin when the intracanal irradiation with high-intensity lasers, such as Nd:YAG and Er:YAG lasers, were used, the association of the zinc phosphate cement with the laser irradiation had no influence on the retention of cast metal posts. 38
Semiconductor diode lasers with a wavelength emission between 805 and 980 nm have also assumed an outstanding place in endodontics due to their antimicrobial action. 28,34 –36 The antimicrobial effect reached by diode lasers is comparable to that achieved by the high-intensity lasers. 35,39
Diode laser radiation emitting at 830 nm are poorly absorbed by water and hydroxyapatite leading to an increased thermal diffusivity and an increase of dental and adjacent tissue temperature, which may cause thermal damage. 40
However, with the correct choice of the laser irradiation parameters, considering safe doses for the periodontal tissue, it is possible to provide a high rate of microbial decontamination on dentin of the root canal 28 without damaging it. 34
The association of diode laser irradiation with conventional endodontic treatment has an effectiveness on sites that are not completely accessible to mechanical and chemical treatments. 29,41,42
To the best of our knowledge, no study analyzed the influence of high-intensity diode lasers emitting at 830 nm on the retention of metal and fiber posts to the dentin root canal, 43 which mainly explored the effect of 980 nm wavelength diode lasers. 41,44 From a clinical point of view, the use of this diode laser to improve post retention is very promising, since its thermal effect and periodontal safety parameters are well known from previous studies 23,35 The present work analyzed the effect of root canal irradiation with high-intensity diode laser, emitting at 830 nm and operating in continuous or pulsed mode, on the retention of metal or fiber posts, cemented with self-etching resin cement or zinc phosphate cement.
Materials and Methods
After the protocol approval by an Ethics Committee (CEP FOUSP #177/10) in accordance with technical specification at ISO TS 11405, the coronal portion of ninety recently extracted single-rooted human teeth, with a minimum root canal length of 14 mm, were removed at the cement enamel junction (CEJ). The endodontic treated roots were then randomized into nine groups comprised of different combination of cements (zinc phosphate cement and Panavia F resin cement), diode laser radiation operation mode (continuous and pulsed mode) and post material (metal and prefabricated fiber post), and the control group (Table 1). The bond strengths were measured by mechanical push-out test for all groups as described in the following sections. The statistical analysis determines the effect of diode laser irradiation on bond strength.
Teeth preparation
To remove all soft tissue within the root canal, teeth were cleaned with a file number 40 (K-file 40; Maillefer, Dentsply, USA) and irrigated with 10 mL of sodium hypochlorite 0.5% solution delivered by a 10-mL BD disposable syringe aided by a magnification lens.
While each sample was endodontically treated by means of Nickel–Titanium rotary instruments (NiTi Protaper Universal; Dentsply, USA) at 350 RPM, according to the manufacturer's recommendations, until the diameter corresponded to file 40, the remaining root samples were submerged into saline solution to maintain their humidity.
During the chemical–mechanical treatments with rotary instruments, irrigation with 15 mL of sodium hypochlorite 1% was used, associated to polyethylene glycol paste as needed. At the end of the instrumentation a final irrigation was performed with 15 mL of EDTA-T 17% followed by 15 mL of sodium hypochlorite 1%. This solution was aspirated with a metallic cannula and root canal was dried with sterile absorbent paper points (Roeko; Coltène/Whaledent, Langenau, Germany). Filling was performed with gutta percha (Dentsply, USA) and AH Plus sealer (Dentsply, Germany). After the endodontic treatment, the filling was removed from 10 mm of the root length from the cervical region, and the canal was shaped with Gates-Glidden bur numbers 1, 2, and 3 of increasing diameters. The roots were then randomly divided into nine groups, as previously described, for intracanal laser irradiation and post cementation according to the treatment group.
Laser irradiation
The diode laser Opus 10 (OpusDent, Yokneam–Israel) emitting at 830 nm with a bandwidth of 5 nm operating in continuous wave mode (CW) or pulsed mode (PL) was used to irradiate the root canal employing a 300 μm optical fiber. The laser optical fiber was inserted into the entire extension of the root canal and irradiated from apical to cervical axis in spiral movements at a ratio of 2 mm/sec, with canal irrigated with 2.5% NaOCl. Five cycles of irradiation with 20 sec time intervals between cycles were performed, allowing cooling the roots between the cycles. This time interval was established in a previous thermal diffusivity study using infrared thermography. 35,40 The average power density of the laser at CW was 1989 W/cm2. A useful duty cycle of 50% (50/50 msec activated/deactivated) was set to PL with an average power density of 994 W/cm2.
Post fixation
Prefabricated fiber posts (Ivoclar/Vivadent, Schaan, Lichenstein) and cast silver–palladium alloy metal posts (Pratalloy; Dentsply, RJ, Brazil), both with compatible size to the previously performed endodontic preparation, were used in this study. For the control group, the posts were cemented without previous laser irradiation of the root canal. The metal posts were manufactured by a prosthetic laboratory in a standardized metal casting of the post. For the treatment groups, laser irradiation was performed, as described previously to the selected post cementation with the respective cementing agent. The zinc phosphate cement (SS White, Brazil) was manipulated with a flexible metal spatula on a glass plate, in accordance with the proportions recommended by the manufacturer. The Panavia F cement (Kuraray Medical, Okayama, Japan) paste A and B (ED primer) were mixed in equal parts for 20 sec. Panavia F was applied into the root canal with a Lentulo file (Maillefer, USA) and on the post with a microbrush to placement. The surplus was removed after 30 sec to allow the initial self-cure of the material. A layer of Oxigard II (Kuraray Medical, Okayama-Japan) was applied to avoid oxygen contact during the self-curing total chemical reaction, following the manufacturer's recommendations.
Preparation of the specimen for push-out test
Each root was sectioned in six slices perpendicular to the post axis (two cervical, two medial, and two apical thirds) using a cutting machine (Accutom 5; Struers, Cleveland, OH). Each slice was 1 mm thick measured with a digital caliper rule (Mitutoyo, Japan).
The bond surface area (A) of the post in each slice was calculated according to the conical section
The samples were positioned into a universal testing machine (Instron 5567, Norwood, MA) within a centralizing plate to ensure the load application at the post center. The load was applied from apical to cervical, due to the post conical shape, with a crosshead speed of 0.5 mm/min until obtaining the maximum failure load. The push-out strength (∂), expressed in Mega Pascals (MPa), is obtained by the expression ∂ = F/A, where F is the force load at failure expressed in Newton (N) and A is the conical surface area expressed in mm2.
Statistical analyses
The randomized groups were previously coded to allow the blind statistical analysis of the data. The push-out bond strength data normality was tested by Ryan-Joiner test. Considering three different independent variables (laser irradiation mode, cement, and post material) influencing the bond strength, a three-way ANOVA test was applied following a Tukey's pairwise comparison with a significance level of p = 0.05. All statistical analyses were performed for each third of the tooth separately due to their biological characteristics, using Minitab Statistical Software 17 (Minitab, Inc.).
Results
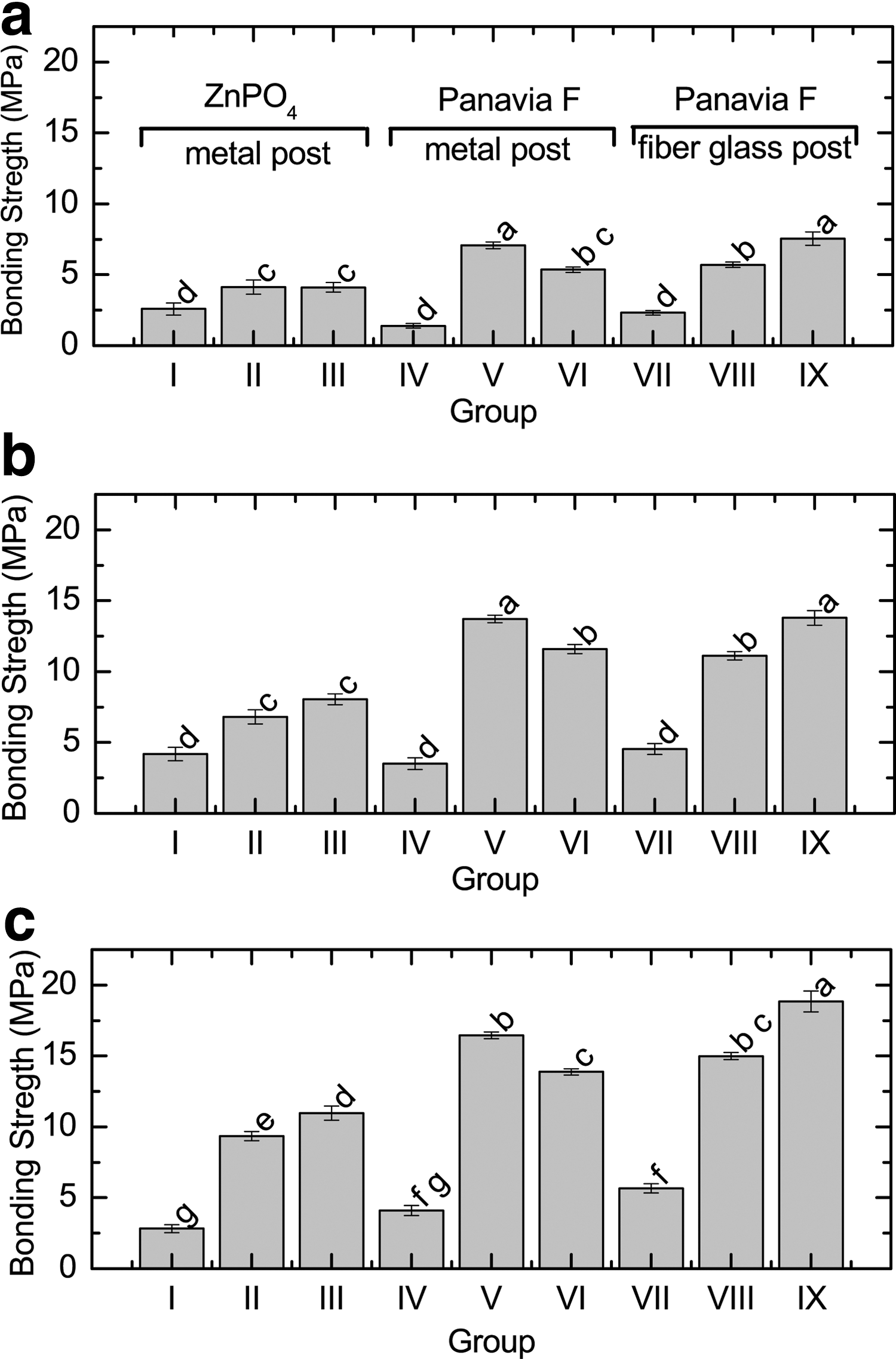
Figure 1 presents the mean and standard error of the bond strength value for all groups at each tooth third (Fig. 1a: Apical, 1b: middle, and 1c: cervical). Pairwise comparison at the different teeth third regions is also shown in Fig. 1 as different letters.
Bond strength values obtained from the push-out tests on
Control groups I, IV, and VII did not present statistical difference (p > 0.05) for the apical and middle third. For the cervical third, the group I that uses metal post had statistical lower bond strength value compared with glass–fiber group VII (p < 0.001).
The apical third presented the lowest absolute bond strength value for all groups compared with the middle and cervical thirds. The highest bond strength values were obtained by the cervical third, especially for the post cemented with Panavia F (groups V, VI, VIII, and IX). The only exception was the control group I, where the middle third had a mean value higher than the cervical third.
On laser irradiated groups, the groups cemented with Panavia F (groups V, VI, VIII, and IX) presented a bond strength statistically higher than the group cemented with ZnPO4 (groups II and III) for all thirds (p < 0.05). The only exception was for the apical third groups III and VI, which were not statistically different (p = 0.053).
For the apical and middle thirds, there has been no statistical difference between groups II and III (p > 0.3). The cervical third group III presented a higher bond strength value compared with group II (p = 0.043). However, the bond strength of the samples irradiated was statistically enhanced for all thirds compared with control group I (p < 0.01).
For all thirds, the groups V and VI presented an enhancement compared with control group IV (p < 0.001). In addition, the group V presented statistically higher bond strength values when compared with group VI for all thirds (p < 0.001).
Groups VIII and IX presented an enhancement compared with their control group VII (p < 0.001). Moreover, group VIII presented a statistically smaller bond strength value compared with group IX for all thirds (p < 0.001).
Discussion
Posts dimensions were standardized for experimental control and to allow comparison between groups to eliminate possible bias at the present study.
We observed that the bond strength values between cement and root canal dentin were higher for the irradiated root canal groups, evidencing the positive effect of the diode laser. This was associated with the removal of smear layer and remaining gutta-percha from the root preparation and endodontic sealers from the dentine root canal surface. This result corroborates a study that evaluated the bond strength of fiber posts cemented to the intraradicular dentine surface previously irradiated with high-intensity diode laser emitting at 980 nm. 44
The number and orientation of dentinal tubules is a fundamental principle of bond strength, once the higher is the number of dentinal tubules the higher is the bond area. The cervical and middle thirds have about 40,000 tubules/mm2, providing a larger area for adhesive system penetration, thereby increasing the potential mechanical tags between cements and dentin. 44,45 The present study specifically analyzed the cervical third compared with the medial and apical thirds and results showed that a statistically significant higher bond strength occurs on the cervical third according to the dentin tubules density of the area that allows a higher mechanical imbrication of the cementing agent into the tubules.
The different materials applied at the post placement process have different bond characteristics and, consequently, different elasticity modulus. Cement characteristics cause differences into the bond strength due to its mechanical and clinical behavior, which may reflect into statistical difference between control groups when an in vitro study is performed. However, the statistical difference between control groups (I, IV, VII) was only observed for the cervical third, where the density of dentin tubules is higher than the other thirds analyzed. The main statistical differences of the results are associated with the laser irradiation and, in this case, the differences on bond strength for metal and fiber posts seem to be related to the laser regime of operation. The laser mode used is related directly to the debris removal, and its inherent microbial reduction, within the root canal allowing the maximum contact between posts' cementing agent and dentin.
The results show that no matter what the post material used, the diode laser significantly improves the bond strength. However, the use of Panavia F as cementing material associated to diode laser irradiation showed more effectiveness on increasing of the bond strength. It is important to note that the bond strength values obtained for the group when metal post is cemented with Panavia F had a higher value when root canal dentine was irradiated on CW (group V), whereas fiber post cemented with Panavia F had the higher bond strength value when dentine was irradiated on pulsed mode (group IX). These results highlight the importance of different protocol for different posts and the appropriate cement selection for each clinical situation. Additionally, the push-out values obtained for Panavia F with fiber post after diode laser irradiation at the present study, were higher than the values obtained for the same post and cement, but irradiated with Er,Cr:YSGG laser described in the previous work. 37 This corroborates that different diode laser irradiation protocol should be adopted to different post and cement material.
Conclusions
The mechanical push-out bond strength of posts in dentin previously irradiated with high-intensity diode laser (emitting at 830 nm) in both continuous and pulsed mode, presented higher bond strength values in comparison with nonirradiated groups. The cervical and middle thirds had the highest values on bond strength associated to diode laser irradiation. The use of continuous mode of laser irradiation improved the bond strength of the Panavia F and the metal post more than the pulsed mode, whereas for the Panavia F and fiber post association, the highest bond strength value was obtained when the pulsed mode was used. At these conditions, the diode laser provided a higher bond strength compared with the use of Er,Cr:YSGG laser. The use of diode laser at 830 nm irradiation showed to be a promising technique to improve the longevity of endodontic treated tooth allowing the maximum contact between post cementing agent and dentin increasing the bond strength demonstrated in this work.
Footnotes
Acknowledgments
This work was supported by FAPESP/CEPID proc. 05/51689-2, Capes/PROCAD proc. 88881.068505/2014-01; CNPq INCT proc. 465763/2014-6 and CNPq proc. PQ 312397/2013-5
Author Disclosure Statement
No competing financial interests exist.