
Abstract
Introduction
S
It is reported that inadvertent extrusion of the irrigant beyond the apical foramen can occur more easily if the apical constriction has been altered or disrupted during root canal preparation. 3,5 The main foramen is reportedly located 2–3 mm from the anatomical apex. This location is clinically important because many root canals are unintentionally instrumented beyond the apical foramen, and slight overinstrumentation may not be radiographically detected in every case. 6
An efficient irrigant should ideally come into direct contact with all parts of the canal system. 1 Although injection of NaOCl into a canal using a syringe and needle is the most commonly used method, 7 there is limited delivery of the irrigant to the apical third and irregular parts of the root canal system. 8,9 To enhance dispersion of the irrigant throughout the root canal, different irrigation devices have been developed. 10 However, one must remember that the type of irrigation system used may play a role in the amount of apical extrusion. 11 Accordingly, an irrigation method that enhances dispersal of the irrigant without increasing the risk of extrusion is desirable. Several irrigation methods, including needle irrigation (NI), laser-activated irrigation (LAI), ultrasonic, sonic, and negative apical pressure irrigation, have been evaluated with regard to the risk of apical extrusion. 11 –15 However, the effects of irrigant activation methods on irrigant extrusion from overinstrumented root canals still remain unclear.
EndoActivator (EA; Dentsply Tulsa Dental Specialties, Tulsa, OK) is a sonically driven irrigation system comprising a portable handpiece and three polymer tips of different sizes that do not cut dentin. 16 It reportedly activates fluids safely and has been demonstrated as an effective tool for cleaning root canals. 15,17
LAI using an Er,Cr:YSGG laser is another method for irrigant activation. 18 The efficacy of erbium lasers is based on the formation and implosion of water bubbles, which causes rapid fluid movement in the canal. 19,20 It is also believed that laser energy may increase the reaction kinetics of NaOCl. 21 Studies 22,23 have reported the positive effects of LAI on the distribution and cleaning ability of NaOCl in areas that are difficult to access.
The aim of the present study was to evaluate and compare the relative safety of NaOCl irrigation using NI, EndoActivator irrigation (EAI), and LAI in overinstrumented root canals by measuring the amount of apically extruded NaOCl with each technique.
Materials and Methods
The Ethics Review Board of Yuzuncu Yil University approved this study protocol.
Thirty mandibular, single-rooted teeth with straight canals that were extracted for periodontal reasons were used. The absence of resorption, calcification, and curvature in the canals was confirmed using radiographic imaging from both the buccal and proximal aspects. The teeth were cleaned, disinfected, and stored in 10% formalin solution at room temperature (23°C) until use.
The teeth were decoronated and the root lengths were adjusted to 19 mm. Under ×16 magnification, a #10 K-file (Dentsply Maillefer, Ballaigues, Switzerland) was inserted into the canals until it was visible at the apical foramen, and the working lengths were recorded for each root.
The coronal third of the canals was enlarged using #4 Gates Glidden drills, and the roots were divided into two groups of 15 roots each. The group 1 samples were prepared 0.5 mm short of the premeasured length (i.e., 0.5 mm short of the apical foramen) with a WaveOne Primary file [(size 25, taper 0.08), Dentsply Maillefer, Ballaigues, Switzerland] using the recorded WaveOne program of the X-Smart Plus endomotor (Dentsply Maillefer). The group 2 samples were prepared 0.5 mm beyond the measured length (i.e., 0.5 mm beyond the apical foramen) using the same procedure. The flutes of the file were cleaned after three in-and-out movements. The patency of the apical foramen was maintained during cleaning and shaping using a #10 K-file. Each canal was irrigated using a total of 5 mL of 2.5% NaOCl during instrumentation. The preparations were defined as complete when the filing reached the predetermined length. All samples were then irrigated with 2 mL of 17% ethylenediaminetetraacetic acid and 2 mL of distilled water. The canals were dried using paper points.
Experimental setup
A modification of the experimental model described by Myers and Montgomery 24 and Altundasar et al. 25 was constructed to collect any apically extruded irrigant during the final rinse. To simulate resistance from periapical tissue, floral foam placed in a cylindrical polystyrene container (Lp Italiana Spa, Milan, Italy) was used (Fig. 1). The cap of the container was closed and weighed using an analytical balance (Sartorius Basic, Sartorius AG, Gottingen, Germany) with an accuracy of 10−4 g. This weight was recorded as the initial weight. Then, a hole was made at the center of another plastic cap using a heated metal instrument, and the root was inserted into the hole with the apex buried in the foam. To equalize the internal and external pressure, a 27-gauge dental needle was inserted into the plastic cap (Fig. 1). The connections of the root, needle, and cap were fixed using cyanoacrylate adhesive. The tooth was isolated with a rubber dam.
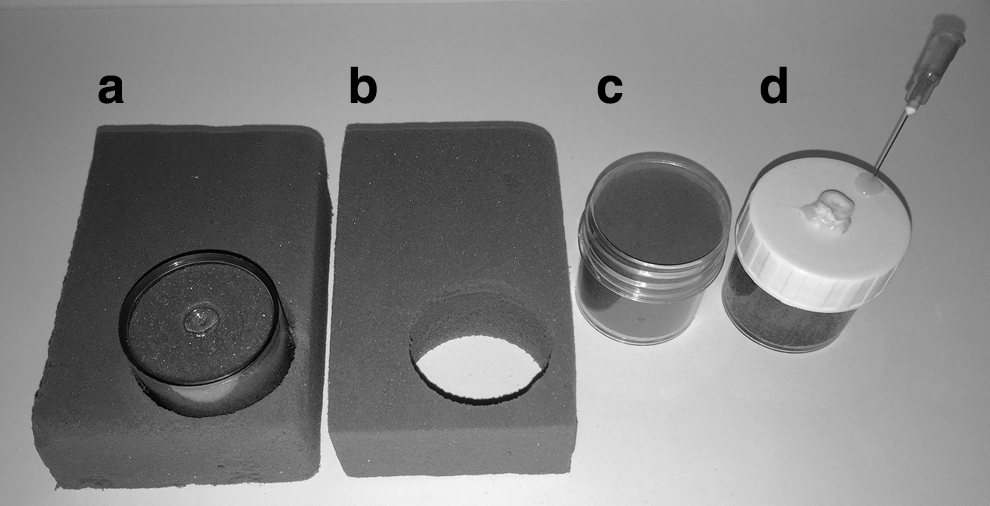
Preparation of the experimental setup for evaluating the safety of sodium hypochlorite irrigation using different techniques in overinstrumented root canals.
Irrigation procedures and laser settings
To avoid factors associated with varying anatomy, the same 30 teeth were included in all three irrigation groups using a randomized crossover design. The concentration of NaOCl was 2.5%, and the total volume of the irrigant used in each group was 3 mL. At the end of each irrigation method, external surfaces and root canals were dried in preparation for the other irrigation procedure. The experimental setup was reconstructed using new preweighed containers for the different irrigation groups.
NI group
In this group, 3 mL of NaOCl was injected (flow rate, 1 mL/10 sec) using a 30-gauge side-opening needle (Max-i-Probe; Dentsply Rinn, Elgin, IL). The tip of the needle was placed 3 mm from the working length and moved in ∼2 mm amplitudes. The procedure was completed in 30 sec.
EAI group
In this group, 1 mL of NaOCl was flushed into the root canal. The EA tip (size: 15.02) was placed 3 mm from the apex according to the manufacturer's instructions and activated at 10,000 cycles/min for 10 sec. The procedure was repeated three times.
LAI group
In this group, 1 mL of NaOCl was flushed into the root canal and activated by Er,Cr:YSSG laser (Waterlase iplus; Biolase Technology, Inc., San Clement, CA [1.5 W, 20 Hz, 75 mJ, 140-μsec pulse duration; no water or air]) for 10 sec using a stationary radial firing tip (RFT2 Endolase; Biolase Technology, Inc.) placed 5 mm from the apical preparation level. The procedure was repeated three times.
At the end of the experiment, each root had undergone all three irrigation procedures. All plastic containers containing the floral foam and irrigant were weighed; this measurement was recorded as the final weight for each container. To calculate the exact amount of extruded irrigant, the initial weight of each container was subtracted from the final weight.
Statistical analyses
All statistical analyses were performed using SPSS 13.0 for windows (SPSS, Inc., Chicago, IL). Normality of the data was approved by the Kolmogorov–Smirnov test, and two-way repeated measures analysis of variance was used to analyze the data for significant differences. Tukey's post hoc tests were used for pairwise comparisons. A p value of <0.05 was considered statistically significant.
Results
The amount of NaOCl extrusion with EAI and LAI was significantly greater in group 2 than in group 1 (p = 0.001 and p = 0.014, respectively). NI resulted in similar amounts of extrusion in both groups (p = 0.221).
In group 2, EAI resulted in significantly greater extrusion compared with NI and LAI (p = 0.008 and p = 0.012, respectively).
In group 1, there were no significant differences among NI, EAI, and LAI (p = 0.58).
Mean values and ranges for the weight of apically extruded irrigant were shown in Table 1.
Represents statistically significant differences between groups 1 and 2.
EAI, sonic irrigation with EndoActivator; LAI, laser-activated irrigation; NI, needle irrigation; SD, standard deviation.
Discussion
The primary objective of the present study was to assess the safety of different methods for NaOCl irrigation during the final rinse in overinstrumented root canals. Extrusion of NaOCl beyond the apical foramen can occur easily in teeth with wide apical foramina or destroyed apical constrictions due to inappropriate root canal preparation or resorption. 3 Complications caused by the apical extrusion of NaOCl include chemical burns, necrosis, ecchymosis, temporary or permanent neurological complications, and even upper respiratory obstruction. 4,26
The absorption of NaOCl at wavelengths between 2500 and 3000 nm, which are ideally suited for LAI, is very high. 27 Although there is considerable research investigating the effects of LAI using erbium lasers on the cleaning ability of root canal irrigants, 22,23,28,29 very few studies 14,30 have focused on the apical extrusion of these solutions with this technique, even though one of the primary goals of root canal irrigation is to minimize apical extrusion of the irrigant and avoid any iatrogenic harm to the patient. Accordingly, NaOCl activation using an Er,Cr:YSSG (2780 nm) laser was one of the techniques evaluated in the present study. Laser energy was delivered into the irrigant via a radial firing tip (RFT2) developed to emit laser light more homogeneously in root canals. Although studies have demonstrated the cleaning efficacy of these tips, 31,32 no study has evaluated the amount of irrigant extrusion.
High energy may favor a cleaner root canal by delivering high peak powers that create more violent shock waves. 33 However, this can increase the risk of apical extrusion. Blanken and Verdaasdonk 18 reported that a minimum of 75 mJ was necessary for the removal of dye-colored liquid from the apical third of the canal. In addition, De Moor et al. 22 reported favorable results with a pulse energy of 75 mJ at 20 Hz for flushing out artificially placed debris plugs. From this perspective, we preferred to use a power setting of 1.5 W and a repetition rate of 20 Hz in the present study.
It is reported that the pressure waves created by pulsed laser activation of irrigants within root canals can lead to apical extrusion of the solution if the laser tip is held too close to the apical foramen. 14,34 A distance of 5 mm between the laser tip and the apical preparation has been confirmed to be safe in previous studies. 22,35 Therefore, in the current study, the activation tip was placed 5 mm from the apical preparation level.
It has been long known that the resistance of periapical tissues has an inhibiting effect on apical extrusion of irrigant. 36 However, in several studies, empty tubes (full of air) were used for collection of the extruded irrigant. 13,37,38 The lack of simulation of periapical tissues was a methodological limitation that has been identified by previous studies as the cause for overestimation of the amount of extruded irrigant. 13,39 In more recent studies, 15,40 the root apices were immersed in a solution or a pH-sensitive gel to overcome this limitation. In the present study, floral foam was used to simulate slight tissue resistance. Similarly, Silva et al. 41 and Altundasar et al. 25 used a bare piece of floral foam with standardized dimensions. However, floral foam is not a wear-resistant material and has a surface that crumbles when picked. This can result in inaccurate measurements during the experimental process. Therefore, in the current study, we used floral foam placed in containers to minimize weight loss during the experiment.
In the present study, similar amounts of NaOCl with no statistically significant differences were apically extruded, regardless of the irrigation technique, in group 1. In this group, intact apical constrictions may have served as barriers against extrusion of the irrigant to some degree. EAI extruded significantly greater amounts of NaOCl compared with NI and LAI, which caused similar amounts of extrusion, in group 2. The 5 mm distance between the laser tip and the apical preparation level may have prevented excessive extrusion by de-escalating the pressure of the shock waves that propel the irrigant beyond the disrupted apical foramen. The close proximity of the EA tip to the apical preparation may have allowed the shock waves to bypass the large apical foramen more easily, resulting in ejection of the irrigant into the periapical tissue.
Between-group comparisons showed that EAI and LAI extruded significantly greater amounts of the irrigant in group 2 than in group 1. The disrupted apices in group 2 may have served as spillways for the pressure waves generated by the activation systems. On the contrary, NI resulted in the extrusion of similar amounts of NaOCl, regardless of the preparation level. Here, the side-vented design of Maxi-i-Probe needle may have prevented the excessive extrusion by directing the irrigant toward the canal wall than the apex.
The results of this in vitro study cannot be directly extrapolated to the clinical situation because the density of the foam has not been correlated with human periodontal tissues. The method used here can only facilitate a relative comparison of techniques under standardized conditions.
Conclusions
Within the limitations of this in vitro study, the results suggest that NI, EAI, and LAI are equally safe when the instrumentation level is maintained 0.5 mm short of the apical foramen. The risk of extrusion remains the same when irrigation was performed using a needle and syringe, regardless of the preparation level. However, overinstrumentation increases the amount of extrusion, particularly when the irrigant is activated with laser or EA. LAI and NI may be safer than EAI in overinstrumented canals. In conclusion, caution should be exercised when using activation systems in combination with irrigants such as NaOCl, particularly in overinstrumented root canals.
Footnotes
Acknowledgments
The authors gratefully acknowledge Prof Dr Sıddık Keskin for performing the statistical analysis.
Author Disclosure Statement
No competing financial interests exist.