
Abstract
Introduction
D
Phototherapy is a therapeutic method which favorably affects cell metabolism and, consequently, the healing processes by using precise parameters of light. Since Mester's discovery in 1968 that low-level laser therapy (LLLT) stimulated hair regrowth in rats, the biological and clinical aspects of low-power lasers have been increasingly investigated and demonstrated at the molecular, cellular, tissue, and systemic levels. 4 –6 For about three decades, lasers were the only source of light in phototherapy until the National Aeronautics and Space Administration (NASA) developed a new generation of light-emitting diodes (LEDs) to accelerate plant growth during space flights. 7,8 Since exposure to LEDs also enhanced wound healing, their influence on tissue was investigated and compared with LLLT. 9 The reviewed studies showed that LED can be as effective as LLLT, since both have similar biological effects with no significant difference between them. 9 –11 The exact mechanism of phototherapy is not yet fully understood. The basic mechanism is thought to be direct energy exchange between the incoming photons and their target—an intracellular chromophore.
The aim of our research was to determine whether phototherapy with LED improves and shortens the healing process of chronic wounds in diabetic patients. Our main outcome was granulation of the wound bed evaluated according to the Falanga wound bed score and reduction of the surface area. 12
Patients and Methods
The prospective randomized double-blind study included 60 consecutive patients with diabetes mellitus and chronic wounds below the knee referred to the University Medical Center Ljubljana from October 1, 2012 to December 1, 2014.
All patients included in the study were referred to our clinic after their general practitioners failed to achieve satisfactory wound healing. Exclusion criteria were patients whose wound surface was too large (over 15 × 20 cm) or patients with wounds expanding to several planes, meaning an even distribution of light through irradiation could not be guaranteed.
All patients received conventional treatment according to the guidelines for chronic wounds, including debridement of the necrotic tissue, maintenance of a moist wound bed, and control of infection.
Patients were randomized into two groups according to additional treatment with LED: an active group (LED group, n = 30) and a control group (Co-group, n = 30). The LED group received active therapy with LED (Ortholumm, Votan, Slovenia) and the Co-group received therapy with light that simulated LED—a placebo (Table 1). The LED and placebo therapies were performed at a distance of 10 cm from the wound. The treatment regime was the same in both groups: three times a week for 8 weeks. The study was double-blind, meaning that neither the patients nor the doctors evaluating the wounds knew to which group the patients belonged.
Contributing ratio of power density of corresponding wavelength.
The LED group was treated with a mixture of three wavelengths. The contributing power density of each wavelength is shown in percentages in Table 1. The LED source was a pulsed wave modulated at a frequency in the kHz range, with a 50% duty cycle. The total energy density during each 5-min exposure time was 2.4 J/cm2 in the LED group and 0.72 J/cm2 in the control group. The Co-group was irradiated with broadband spectrum (automobile light bulbs were built into the same LED housing and red filters were added) with the same 5-min exposure time. In the placebo device, the total energy was equally distributed between wavelengths 580–900 nm. This means that the energy of every wavelength was approximately 0.00225 J/cm2, which is 50–100 times less than the total energy densities in the active-LED device. Therefore, we considered this to be placebo therapy.
In both groups, blood samples were taken before treatment for a complete blood cell count and white blood cell differential, electrolytes, C-reactive protein, fibrinogen, and erythrocyte sedimentation rate at baseline, and again after 8 weeks of treatment. Wound surface, which was estimated from wound photos using the computer program ImageJ® (US National Institutes of Health, Bethesda, MD), and wound status, according to the Falanga wound bed score, were evaluated every second week. Falanga scoring is a clinical tool for the evaluation of wound healing progress considering granulation, presence of fibrin, and wound exudate (Table 2).
Statistical analysis
For statistical analysis, a paired t-test and Chi-square test were performed to compare the variables before and following treatment and between the groups. The Mann–Whitney test was also used, as well as the median and ANOVA for repetitive measures. Mean differences and a 95% confidence interval (95% CI) were calculated with two-sided probability (p) values; the level of significance was set at p < 0.05. Statistical analysis was performed using IBM SPSS Statistics, v. 19 (IBM Corp, Armonk, NY).
Ethical aspect
The study was approved by the National Medical Ethics Committee (approved on March 15, 2011, Ref No: 116/03/11). Written consent was obtained from all patients included in the study.
Results
The groups were comparable according to sex distribution (25/30 men in LED group and 21/30 in Co-group; p = 0.80). On average, the patients in Co-group were slightly but not significantly older (66.9 vs. 61.4 years; p = 0.09).
The average surface of the wound before treatment was 1315 mm2 in the LED group and 1584 mm2 in the Co-group (p = 0.80). Wound surface was evaluated as the percentage of the starting wound surface area (starting as 100%). Figure 1 shows the reduction of wound surfaces during the 8 weeks of treatment. Wound surface in the LED group showed a slightly but not significantly faster reduction compared with the control group. After 8 weeks, the mean surface in the LED group was 56% of the starting wound surface compared with 65% in the Co-group (p > 0.05).
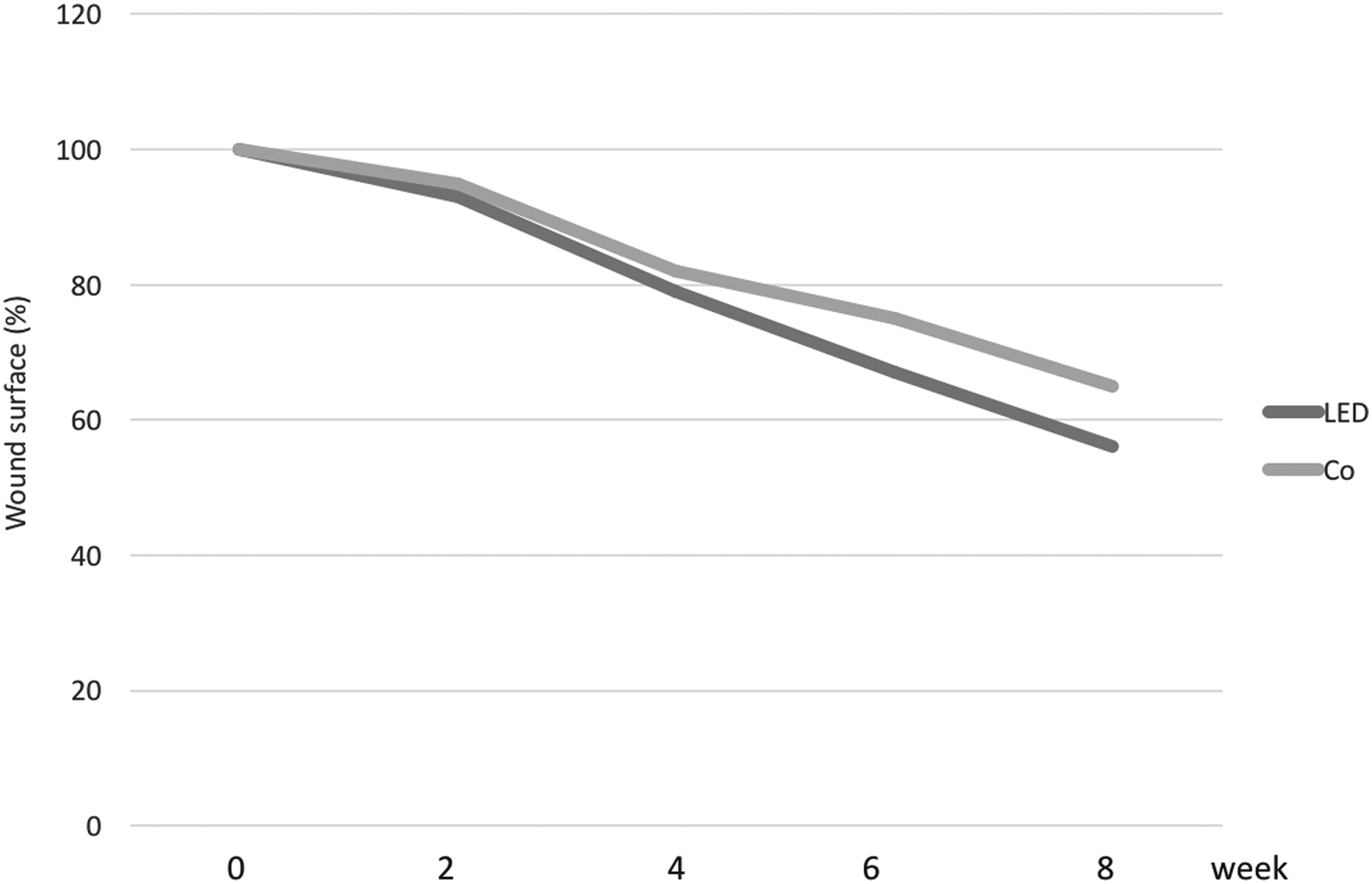
Wound surface as a percentage of the starting wound surface and its reduction during the 8 weeks of treatment.
The Falanga wound bed score before treatment was comparable in both groups, although slightly but not significantly better in the Co-group (Fig. 2).
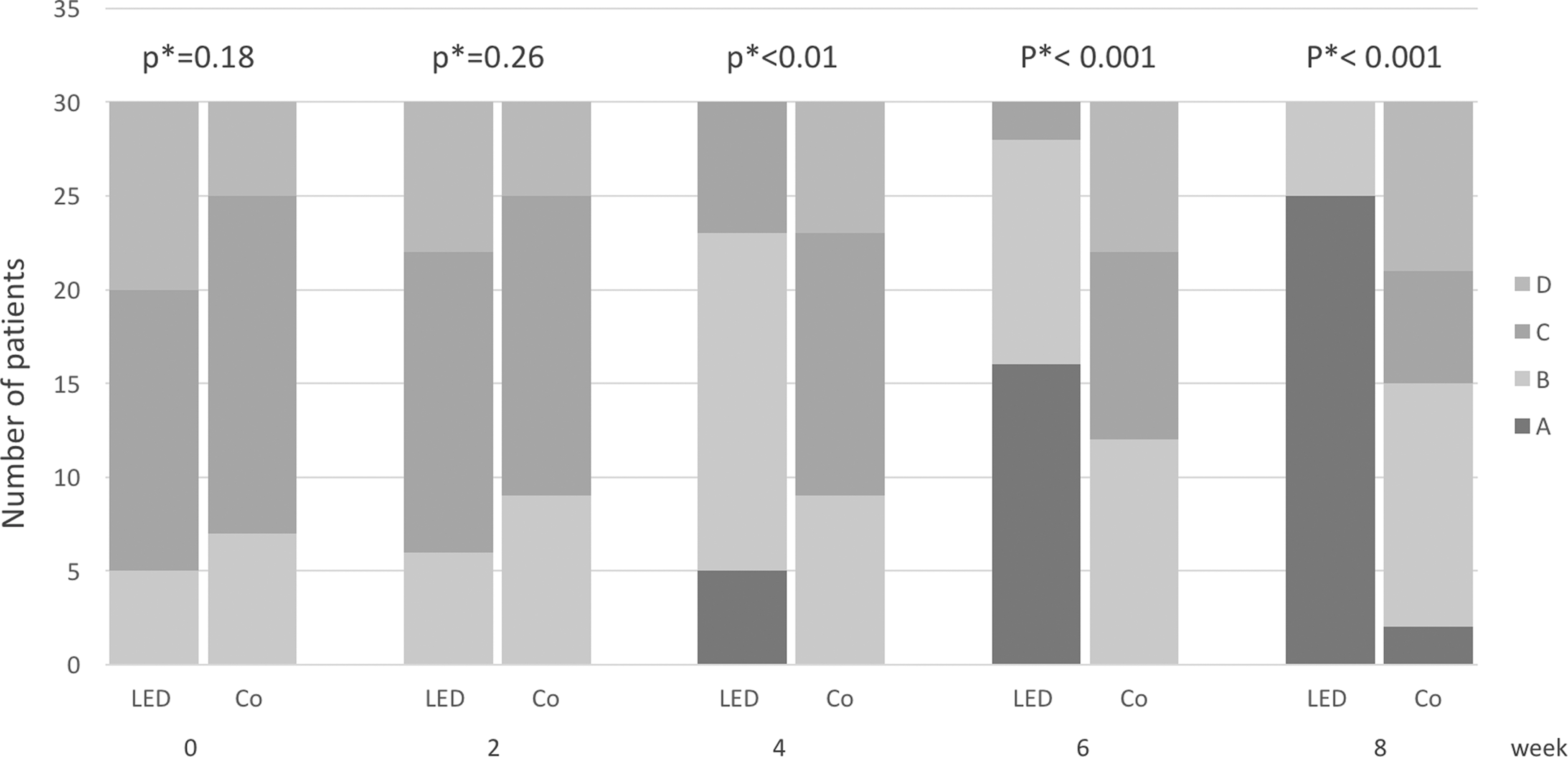
Falanga wound bed score evaluated every 2 weeks during the 8 weeks of treatment. *Student t-test.
After 2 weeks of treatment, the Falanga wound bed score was still comparable between both groups, as was the wound surface.
After 4 weeks, the Falanga wound bed score was significantly better in the LED group while wound surface was still comparable between both groups.
Between the fourth and eighth week of treatment, the LED group showed a remarkable improvement in wound bed granulation and reduction of fibrin and eschar, resulting in a significantly better Falanga score compared with the Co-group. After the fourth week, wound surface in the LED group started to reduce faster compared with the control group, but the difference was not significant.
No side effects were observed in any of the patients during treatment.
Discussion
Diabetes mellitus is one of the main causes of chronic wounds; however, standard treatment modalities often fail to achieve healing. Underlying conditions such as peripheral vascular disease, neuropathy, and poor blood glucose control contribute to slow healing rates and recurrence of diabetic wounds. Wound healing is a complex mechanism. In diabetic patients, various factors of healing are impaired: a decreased production of growth factors, decreased production, migration, and proliferation of fibroblasts, keratinocytes, and endothelial cells. 12,13 Diabetic ulcers increase the risk of wound chronicity, infection, and amputation. 13 Conventional therapeutic methods include debridement of necrotic tissue, infection control, and maintenance of the moist wound bed with various dressings, but the results are often unsatisfactory.
Phototherapy, a noninvasive and pain-free method, offers a new possibility of adjuvant therapy. Although most findings about phototherapy come from LLLT research, the source of light (laser or LED) is not as important as wavelength, total energy density, time intervals of irradiation, and duration of treatment. 9
Our results confirm previous findings that granulation of the wound bed was significantly faster in the LED group, although it was not as expressed in our study as in the research conducted by Minatel. 14 In his study, significantly faster granulation was noted after 15 days of treatment, compared with 4 weeks in our study. Moreover, Minatel found that the healing rate (calculated from wound surface) was significantly faster in the LED group after 15 days, whereas in our study, the difference in wound surface remained insignificant even after 8 weeks of treatment. It seems that Minatel's light regime was more successful than ours. Minatel's total energy density per week was 6 J/cm2 (3 J/cm2, twice per week), which is similar to ours with 7.2 J/cm2 (2.4 J/cm2, three times per week). But the ratio of wavelengths used was different. In our study, 71% of total energy density was from 660 nm and only 5% from 850 nm, whereas in Minatel's study, 89% of energy was from infrared light (32/36 diodes were 890 nm).
The decision to use the described regime with the highest ratio of 660 nm light was based on our previous findings and literature suggesting that the light of 660 nm stimulated the transcription of genes involved in the electron transport chain and stimulated Cytochrome C oxidase in stressed fibroblast cells. 15 –17 In addition, the wavelength of 660 nm is supposed to be the safest for clinical use since, according to Nussbaum, it suppresses bacterial growth far more efficiently than 630, 810, or 905 nm laser light, especially if low doses (around 2 J/cm2) are used. 18 According to Huang and his theory, low doses are supposed to be more effective since higher doses have an inhibiting effect. 19
In our previous research, we confirmed that the same regime improved microcirculation in the healthy skin at the border of the wound and led to faster granulation of the wound bed. 15 Therefore, we expected the wound surface in the LED group to reduce faster compared with the control group. The wounds heal from the edges when the granulation tissue in the wound bed provides a satisfactory basis for epidermal and fibroblast overgrowth. If our observation period had been longer, it is possible that the positive influence of LED on wound closure would have been noted. Landau confirmed faster wound closure of chronic diabetic wounds when using a broadband light device (400–800 nm at 180 mW/cm2, twice a day), but the follow-up time was twice as long as in our study (16 weeks). 20 Kaviani reported significantly faster reduction of chronic diabetic wounds after 4 weeks in patients who were treated with LLLT (685 nm, 10 J/cm2). 21 In Kaviani's research, power density was much higher than in ours and patients received treatment six times per week, meaning that the complete light dose per week was at least five times higher than in our case. El Deen compared the influence of polarized light therapy and LED on chronic diabetic foot ulcers. 22 In this study, broadband polarized light with a bandwidth from 480 to 3400 nm was used, with total energy density of 19.2 J/cm2 per session. The energy density of LED was 4 J/cm2, where the wavelengths of 850, 880, and 950 nm contributed 92% of total energy and 670 nm only for the remaining 8%. The results showed improved healing in both groups, although polarized light was found to be more effective. Vitse conducted a double-blind, randomized study on effects of LLLT on venous leg ulcers. The treated group received laser light of 635 nm and energy density of 2.95 J/cm2 twice a week. 23 After 12 weeks of treatment, no difference in ulcer area reduction or the ratio of complete ulcer closure was observed.
All mentioned studies that confirmed faster wound healing used longer wavelength light and/or higher energy doses. Despite Nussbaum's findings that light of 810 and 905 nm stimulates bacterial growth at most energy densities, this influence did not hinder wound healing. Of course, infected wounds require antibiotic treatment first, but we have to be aware that all wounds are contaminated and bacteria stimulating light therapy could theoretically cause a wound infection and slower healing, which was not the case in any of the mentioned studies. 14,21 –23 Obviously, in vitro conclusions cannot always be directly applied to in vivo situations.
According to in vitro experiment results, our treatment regime (where light of 625 and 660 nm was predominantly used) should shorten wound closure time. Brondon confirmed increased cell proliferation in human epidermal cell lines irradiated with LED 670 nm, 5 J/cm2, especially when pulsed wave (as in our case) was used. 24 Zhang confirmed that human fibroblasts in vitro showed faster proliferation when treated with 628 nm laser at energy density 0.88 J/cm2. 25 Energies above 4 J/cm2 yielded an inhibitory effect. Similarly, Hawkins confirmed a positive influence of LLLT with 632.8 nm and energies as a single dose of 5.0 J/cm2 or multiple doses of 2.5 J/cm2 on human fibroblast proliferation and cell migration in vitro. 26 Higher doses (16 J/cm2) yielded an inhibitory effect. Both studies confirm the dose-dependent effect described by Huang. 19 Lev-Tov, who succeeded in suppressing fibroblast proliferation using high energies (633 nm at energies 160, 320, 640 J/cm2 and 830 nm at energies 80, 160, and 320 J/cm2), additionally confirmed Huang's theory in his study. 27
Although our study did not substantiate that LED therapy shortens wound closure time with the regime described, it nevertheless established a beneficial influence for clinicians. Complete healing is the final goal that can take, especially in the case of large wounds, weeks or months. Therefore, preparing the wound bed to enable coverage options with surgical techniques can importantly shorten the time required to complete healing. But to get the most out of phototherapy, perhaps the parameters that we use should be adjusted during the healing phase of the wound?
The phototherapy regime that we used improved granulation of the wound and, as described in our previous report, also the microcirculation that is mandatory for wound healing. 15 But different cell types respond to different wavelengths, as demonstrated by Moore on mice fibroblast and endothelial cell lines. 28 Belleti demonstrated a positive influence on human dermal fibroblast cell lines when irradiated with 915 nm, 5 J/cm2, especially when pulsed wave was used. 29 In addition, Basso confirmed better migration of epithelial cells using LLLT at 780 nm and energies 1.5 and 3.0 J/cm2. 30
The conflicting results of the published studies leave a lot of room for skepticism. It is, however, undeniable that phototherapy has an influence, but we have to learn how to take full advantage of it when used in clinical practice. As has been shown, findings from in vitro experiments cannot always be directly applied to clinical use. Cell lines grow in one layer, but live tissue is multilayered and structured from various cell types. Thus, the dose that reaches deeper layers is undoubtedly smaller compared with the dose received in cell lines. Obviously, the used energies should be higher, similar to those reported in studies where wound closure time was significantly shorter. 14,20 –22 The wavelength most stimulative for cell types is also not easy to define and perhaps this is why the broadband or a combination of multiple wavelengths give better clinical results. 20,21 An additional problem is that most studies do not define whether continuous wave or pulsed wave irradiation was used. As described by Belletti, the light of 915 nm and 45 J/cm2 in pulsed mode has a positive effect, compared with continuous wave, which has a slightly negative effect on human dermal fibroblast metabolism. 29
Chronic wounds are very difficult to treat. Since they often fail to respond to conventional treatment, adjuvant treatment options are needed. Despite conflicting results, phototherapy remains a promising field as most studies report a beneficial influence and none report any adverse effects. In addition to in vitro studies and animal experiments, clinical studies, where all parameters of phototherapy are well defined, are needed to identify the optimal treatment regime.
Conclusions
Wound healing is a complex multistage mechanism in which phototherapy has a beneficial role. Considering our results, phototherapy with LED prepares the wound bed for further treatment options and gives diabetic patients a better chance of full recovery. Continued research is necessary to determine the best parameters and the true value of phototherapy with LED in routine wound care.
Footnotes
Acknowledgments
The authors thank all patients for their participation, nurses of the Department for Surgical Infections for their additional work, and Votan for donating the LED for the purpose of this study.
Author Disclosure Statement
No competing financial interests exist.