
Abstract
Introduction
M
Phototherapy is a noninvasive nonpharmacological form of treatment that, according to some researchers, has demonstrated positive results when used to prevent and/or control muscle fatigue. 1,2,4,5 The therapeutic effects of phototherapy include modulation of the inflammatory process, analgesia, and the modulation of cell activity. 6,7 Some authors, such as Martens, 8 Melis et al., 9 and Ahari et al., 10 state that the increase in the production of adenosine triphosphate may be related to muscle relaxation and an increase in local blood microcirculation, which accelerates the removal of catabolites from tissues. Phototherapy also acts on C fibers, diminishing the permeability of the membrane for Na and K, which results in a slower conduction of the nerve stimulus and is associated with the anti-inflammatory effect.
Despite the growing number of studies evaluating the effect of phototherapy on muscle fatigue, a small number of investigations have specifically addressed the masticatory muscles, 11 –13 which raise doubts with regard to the dosage to be used and the effectiveness of this form of treatment on these muscles. Thus, the aim of the present study was to evaluate the effect of phototherapy on bite force, mandibular range of motion, sensitivity to palpation, and fatigue in the masseter and anterior temporal muscles of young patients when administered before the induction of fatigue.
Materials and Methods
This study was conducted in compliance with the regulatory norms guiding research involving human subjects and received approval from the Plataforma Brasil national review board under process number 1.463.519. This trial is registered with
The sample was composed of healthy, young, male, and female adults enrolled at University Nove de Julho–Vergueiro Campus, São Paulo, Brazil (Fig. 1).
• Inclusion criteria: age 18–23 years, absence of a diagnosis of temporomandibular disorder (TMD) and signed statement of informed consent.
• Exclusion criteria: currently undergoing orthodontic treatment, currently undergoing orthopedic jaw treatment, psychological therapy or physical therapy, and use of muscle relaxant, anti-inflammatory agent, or bite plate. In total, 28 patients were excluded.
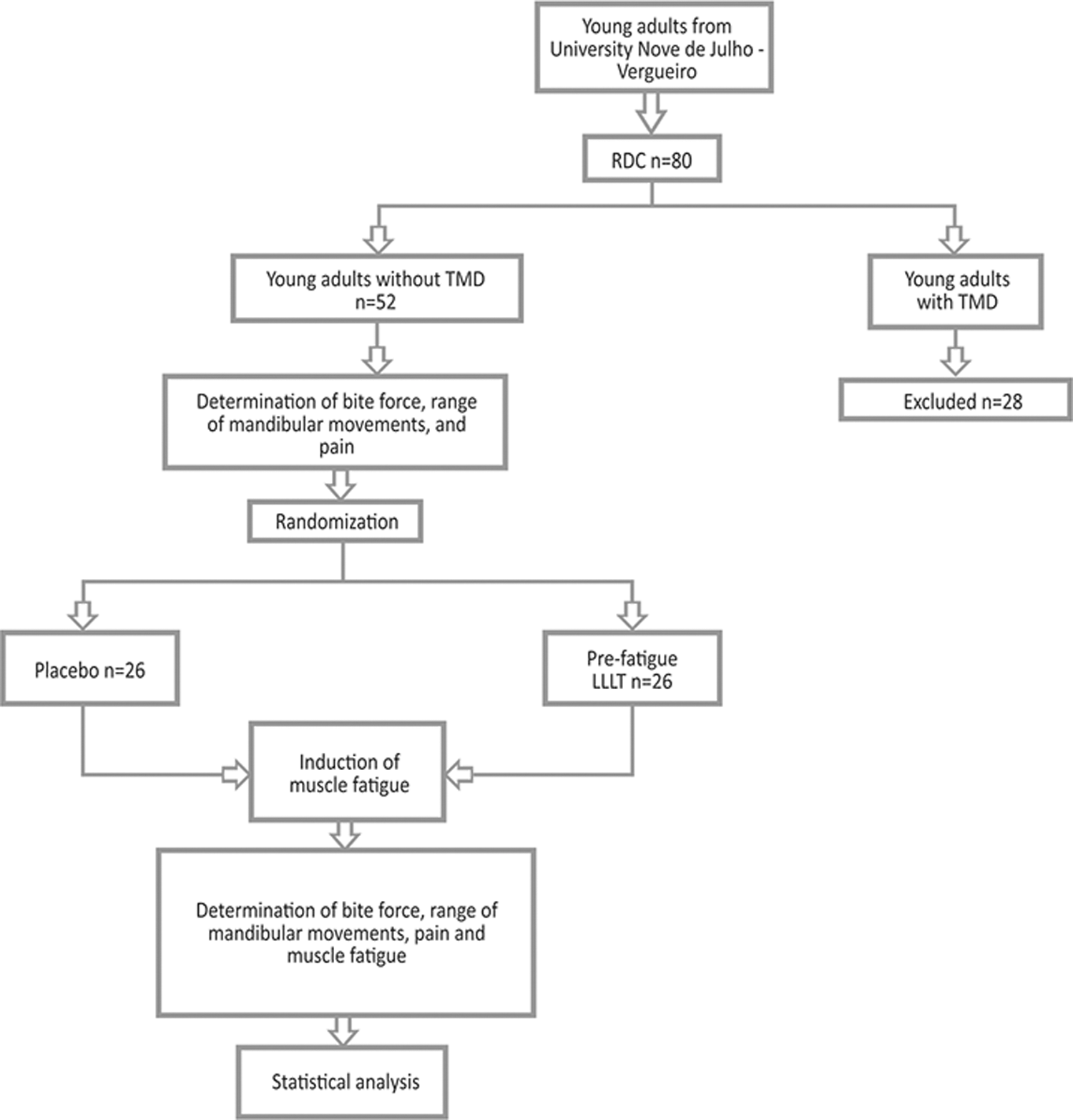
Methods fluxogram.
The volunteers were divided into two groups (active and sham laser therapy) based on a randomization method involving opaque sealed envelopes stipulating to which group a given volunteer would be allocated. The envelopes were opened at the beginning of the evaluation session. All volunteers were submitted to evaluations before and after the induction of fatigue. The null hypothesis of the study was that phototherapy is not effective on bite force, mandibular range of motion, sensitivity to palpation, and fatigue in the masseter and anterior temporal muscles of young patients when administered before the induction of fatigue.
Questionnaire
The participants filled out the Research Diagnostic Criteria for Temporomandibular Disorder (RDC-TMD) questionnaires for the diagnosis of TMD. A specific clinical examination was also performed by a single examiner who had undergone a training exercise. The examination involved palpation of the trapezius, sternocleidomastoid, temporal, masseter, digastric, and medial pterygoid muscles, palpation of the temporomandibular joints, analysis of mandibular movements with the aid of digital calipers, and the determination of joint sounds with the aid of a stethoscope. Frequent headache, facial pain, fatigue/difficulty when chewing, bruxism, psychological aspects, and parafunctional habits were also investigated. 13 Individuals with a diagnosis in group I, II, or III of the RDC-TMD were excluded from the study.
Bite force
Bite force was determined using a digital dynamometer (DMD model, Kratos Equipamentos Industriais Ltda, Cotia, SP, Brazil), which is an electronic force meter composed of a bite fork and digital device connected by a wire. Measures were taken in the first molar region. The participants first received instructions and training to become familiar with the device. Six readings were made—three on each side, alternating sides between readings. Each reading lasted 5 sec, with a 1-min rest between readings. 14 These data were collected at both the initial and final evaluations.
Mandibular range of motion
The guidelines of the International Association for Dental Research were followed for the RDC-TMD, which recommends a single measure of each movement. 13 The volunteer was instructed to open the mouth as wide as possible, and maximum voluntary vertical mandibular movement was measured as the distance between the incisal edge of the maxillary and mandibular central incisors with the aid of digital calipers. The volunteer was then instructed to repeat the movement, while pressure was applied to the maxillary and mandibular teeth with the aid of the calipers for the determination of maximum passive vertical mandibular movement. These procedures were performed during the initial and final evaluations to record the mandibular range of motion before and after the administration of phototherapy.
Assessment of pain
The visual analog scale (VAS), which is a numeric scale ranging from 0 (absence of pain) to 10 (most intense pain), 15 was administered during the initial and final evaluations to record pain upon palpation of the masseter and anterior temporal muscles.
Assessment of fatigue
The fatigue visual analog scale (VAS-F) was used to quantify the subjective sensation of fatigue before and after the induction of fatigue. The VAS-F consists of a 10-cm line with 0 (absence of fatigue) printed at one end and 10 (maximum fatigue) printed at the other end. 16,17 The volunteer was instructed to mark a line between the two extremes of the scale corresponding to the sensation of fatigue in the masseter and anterior temporal muscles during the initial evaluation, as well as after having completed 6 min of chewing.
Photobiomodulation
Photobiomodulation was performed with the Twin Flex Evolution® device (MM Optics, Brazil). The patient was seated comfortably in a soundproof room with the Frankfurt plane parallel to the ground. The irradiation sites were cleaned with 70% alcohol. The active tip of the laser was covered with transparent plastic wrap to avoid cross-contamination and for the purposes of hygiene. Three points on the masseter muscle (upper, middle, and lower bundles) and one point on the anterior temporal muscle were irradiated on each side of the face. The active laser parameters were wavelength = 780 nm, energy density = 25 J/cm2, power = 50 mW, power density = 1.25 W/cm2, and exposure time = 20 sec per point, resulting in a total energy of 1 J per point and 8 J per volunteer. The laser was applied in point mode with a conventional tip and in contact with the skin (spot area: 0.04 cm2) (Table 1). The same procedures were conducted during sham therapy, but the device was not activated, and a recorded sound was emitted to give the volunteer the sensation of active therapy. 18,19
Induction of fatigue
The gum chewing protocol employed in the study by La Touch et al. 16 was used to induce fatigue. The volunteer was seated comfortably in a chair with back supported by the back rest, no support of the neck and head, feet supported on the ground, and hands resting on thighs. The volunteer was given two pieces of gum and instructed to position one on each side of the mouth, chew the gum for 60 sec, and rest for 70 sec. The volunteer was then given a signal to chew for 6 min at the pace of a metronome set at 80 bpm.
Sample size calculation
A G* Power software (v.3.1.9.2, Franz Faul, Universität Kiel, Germany) was used to estimate sample size. The calculus was based on a pilot project in which two groups [sham (n = 11) and laser (n = 8)] were evaluated before and after treatment. The n was estimated by a t-test, comparing sham and laser groups before treatment and sham and laser groups after treatment. Among the variables evaluated, mouth opening was the one with the highest standard deviation, so based on a worst-case scenario, this was the variable of choice for the sample calculation. The mean of both groups post treatment was divided by the highest standard deviation among groups. The measurements before and after intervention were calculated with significance of 5%, power of 80%, and the following effect size:
To detect differences between means, two groups with 26 patients each were required.
Statistical treatment of data
The data were tabulated and treated using the SPSS 21.0 for Win program, and a descriptive statistics was performed. The variables bite force, mouth opening, maximum mouth opening, lateral excursion, and protrusion were analyzed by t-test between groups and by paired t-test before and after treatment. The pain variable was analyzed by the Wilcoxon test. A significance level of 5% (p < 0.05) was considered in all analyses.
Results
Eighty volunteers signed the statement of informed consent and completed the RDC-TMD questionnaire, of which 28 were excluded and the other 52 were randomized to sham group and laser group.
The descriptive analysis was performed for both groups and it was observed that the highest recorded mean values were for the maximum opening movement and the lowest for the protrusion movement. When comparing the means between groups (sham and laser) it was possible to observe that the means of the sham group, both initial and final, are slightly higher than the treated group in all variables and that in both groups there was a discrete increase in the final mean in relation to the initial one, with the exception of mouth opening, as described in Table 2.
F value = Statistic “F”; Pr > F = “p” value; SD, standard deviation; SE, standard error.
The t-test shows a difference for the main factor TIME, for the right bite force, Pre<Post (p = 0.047). For the other conditions, the comparisons were not significant, being the data described in Table 3.
Significance, p < 0.05.
The visual analog scale scores, used to evaluate the muscle sensitivity to palpation and the sensation of fatigue, are described in Table 4, where it is possible to observe an increase in the means of the evaluated variables, of both groups, after the induction of fatigue.
Significance, p < 0.05.
Discussion
Muscle fatigue is characterized by the incapacity of the musculature to maintain high levels of force and is seen as a defense mechanism of the organism that is activated to prevent irreversible cell damage and muscle injuries. 20 Studies have demonstrated that fatigue is associated with a decline in muscle strength during and after maximum effort exercises, the inability to maintain the intensity of exercise over time, a reduction in contraction velocity, and an increase in muscle relaxation time.
Phototherapy has been widely used in different health fields as a noninvasive therapeutic modality that can provide pain relief, a reduction in the inflammatory process, and the enhancement of the tissue regeneration process. As the indication of phototherapy for cases of muscle fatigue remains a new field of research, adequate parameters and effectiveness have not yet been determined. Some studies involving different muscles of the human body suggest that phototherapy administered before the practice of exercise may reduce fatigue, increase muscle torque, increase endurance, diminish the accumulation of lactate, and improve muscle performance. 1,2,5,12,21,22
In the present study, no statistically significant differences were found with regard to mandibular range of motion. These findings are in agreement with data described in a clinical trial by Muñoz et al., 11 who used laser with wavelengths of 685 and 830 nm, a dose of 30 mW, and energy density of 4 J/cm2 on eight points of the masseter muscle for 5 sec per point, concluding that the parameters used did not prevent fatigue. In our study, a total of 1 J per point was used.
In contrast, Silva et al. 23 found an increase in resistance to fatigue using 830 nm, 6 J/cm2, and 0.035 W for 7 sec per point on eight equidistant points of the master muscle. Likewise, Vieira et al. 1 used laser at a wavelength of 808 nm on the vastus medialis, vastus lateralis, and rectus femoris muscles and concluded that resistance to fatigue increased when laser was administered during rest intervals (thrice in the same day).
Leal Junior et al. 22 evaluated low intensity laser administered to the anterior tibialis muscle and concluded that laser had no effect on fatigue, but led to an improvement in muscle performance, which is in agreement with data described by Vanin et al. 2 In contrast, evaluating the effect of photobiomodulation on the rectus femoris muscle of elderly women, Vassão et al. 24 found that low intensity laser did not result in an increase in muscle performance, but was effective at reducing the degree of fatigue.
In contrast, in the present study, the muscle sensitivity to palpation presented a statistically significant difference for the anterior temporal, superior, middle, and lower masseter muscles for both groups. In these cases, the final evaluations had an increase compared to the initials, different from what is reported in previous studies, where the sensitivity is controlled or even reduced after the use of the laser. However, in these cases of sensitivity control the protocols had a greater number of applications. 6,10,19,25
Several studies combining TMD and phototherapy have been conducted. 26,27 However, there is a shortage of trials that focus specifically on the prevention of muscle fatigue in masticatory muscles. Regarding the sensation of fatigue, the results of this study presented a statistically significant difference when comparing the final scores with the initials in both groups and in both muscles, suggesting that the application of phototherapy at the dose proposed in this study was not effective in controlling the intensity of fatigue, being recommended the evaluation of other doses for this purpose in a single application.
With the obtained results from different preliminary studies, such as the one from Vassão et al., 24 Vieira et al., 1 Leal Junior et al., 22 and Nampo et al., 4 in different muscles of the body, it can be said that fatigue control, the improvement in muscular performance, and retardation in the installation of fatigue are important results that reinforce the need for new studies, to determine effective preventive protocols.
As study limitations we can cite the lack of more than one section of treatment and of periodic controls. In contrast, the clinical relevance of this article lies in the fact that phototherapy could be a good option to prevent muscle fatigue during dentistry procedures in which patients need to keep their mouths open for a long time. Longer treatments could be done in one session and discomfort could be avoided during and after these procedures. It is necessary to conduct more clinical trials, with different laser parameters, to achieve more satisfactory results in the prevention of fatigue.
Conclusions
With the protocol proposed in the present randomized, sham-controlled blind clinical trial, phototherapy administered before the induction of muscle fatigue did not lead to any changes in bite force and mandibular range of motion. The final muscle sensitivity and muscle fatigue presented an increase in relation to the initial evaluation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.