
Abstract
Introduction
P
The use of fixed orthodontic appliances—particularly multi-bracket appliances—is a major component of standard orthodontic treatment. The age of the typical patient undergoing this type of treatment is 10–14 years. However, in addition to the many mechanical advantages that the appliances provide (translation, controlled force movement, etc.), they lead to increased accretion of plaque on the brackets and greater difficulty in maintaining oral hygiene, and reducing the self-cleaning process. The plaque configuration observed in bracket recesses differs in terms of its chemical and biological parameters from that seen in regular plaque. 22 In addition to a reduced pH and increased amounts of calcium, phosphates, and carbohydrates, the plaque is characterized by larger numbers of bacteria, which are associated with the development of gingivitis. 22 –25 Studies have shown that even patients with good oral hygiene who are treated with fixed orthodontic appliances can develop gingivitis. 26,27 Gingival epithelial cells represent the first physiological barrier against periodontal pathogens. Bacterial metabolic products are able to penetrate the epithelium and disturb its functional and structural integrity. 28,29
The aim of gingivitis treatment is based on professional tooth cleaning to reduce etiological factors such as biofilm and dental calculus. This procedure initiates gingival healing. Another treatment method is to use PBMT, which reduces inflammatory processes and normalizes local immunity and microcirculation in the periodontium. 30 Studies have described a statistically significant improvement in the healing process in gingivitis when adjuvant PBMT is used in addition to conventional treatment procedures. 30 PBMT is entirely painless and noninvasive and does not lead to any harmful effects. 31 Using adjuvant PBMT may therefore improve the healing process in patients with gingivitis during multi-bracket treatment and after bracket removal.
Therefore, the aim of this study was to assess a possible effect of PBMT as an adjuvant treatment for gingivitis in patients after removal of multi-bracket appliances, testing the hypothesis of PBMT accelerating wound healing after treatment of gingival inflammation.
Material and Methods
Study design
This was a patient blinded split-mouth randomized controlled trial.
Patients, inclusion and exclusion criteria
The study included 13 patients (six female, seven male; mean age 16.15 years; standard deviation ±2.12 years). The patients were recruited on a randomized basis in the Department of Orthodontics of the University of Marburg (Germany) in 2015. Exclusion criteria were any conditions that might influence the periodontal healing process and thus distort the results of the PBMT treatment. These included the presence of systemic diseases, a need for antibiotic prophylaxis, contraceptives, anti-inflammatory medication or anticoagulant drugs, tobacco consumption, local infections, pregnancy, and periodontitis or presence of periodontal pockets. Patients with intellectual or physical disabilities were also excluded. The inclusion criteria were as follows: completion of active treatment with a multi-bracket appliance that needed to be removed; receipt of at least 18 months of orthodontic treatment with brackets; age 12–19 years; and brackets present on the teeth 16–26 in the first and second quadrants. All of the patients and their guardians were informed verbally and in written form about the study procedure and related treatment procedures and had provided informed consent to participation in the study by obtaining signatures. Consent forms of participants less than 18 years of age were signed by a parent and the patient. Patients who did not want to participate in the study received the standard treatment. The study was conducted in full accordance with the ethical principles set out in the World Medical Association Declaration of Helsinki (2008 revision) and was approved by the Local Institutional Ethics Committee (Ref. no: 33/15).
Stopping guidelines
The procedure was stopped by the request of the patient or parent.
Clinical parameters
All of the patients had received at least 18 months of orthodontic treatment with self-ligating brackets (SPEED System™; Strite Industries Ltd., Cambridge, Ontario, Canada). When treatment with the multi-bracket appliance has been completed, the device needs to be removed. As recommended by the manufacturers, the brackets were removed using appropriate bracket removal pliers (Dentaurum, Ispringen, Germany). Residual adhesive material on the enamel surface was removed using a rotating fraise (red ring; Komet Medical, Lemgo, Germany). The removal procedure was followed by professional tooth cleaning; all of the teeth were polished with a rotating brush and polishing paste (Zircate Prophy Paste®; Dentsply DeTrey Ltd., Constance, Germany). After removal of the multi-bracket appliance and professional tooth cleaning, but before PBMT (T0), bleeding on probing (BOP) and the papilla bleeding index (PBI) were assessed by a blinded investigator (M.S.) who had not been involved in the patient's orthodontic treatment (Fig. 1). BOP was assessed in the first and second quadrants, with four measurement points (distal, mesial, buccal, and palatal) assessed at each tooth from tooth 16 to 26, by gentle probing of the gingival sulcus with a pressure-calibrated periodontal probe (Viva TPS Probe®; Ivoclar Vivadent Ltd., Schaan, Liechtenstein) with a probing force of 20 g. Bleeding points were assessed 30 sec after probing and the BOP was calculated in percentage. 32,33
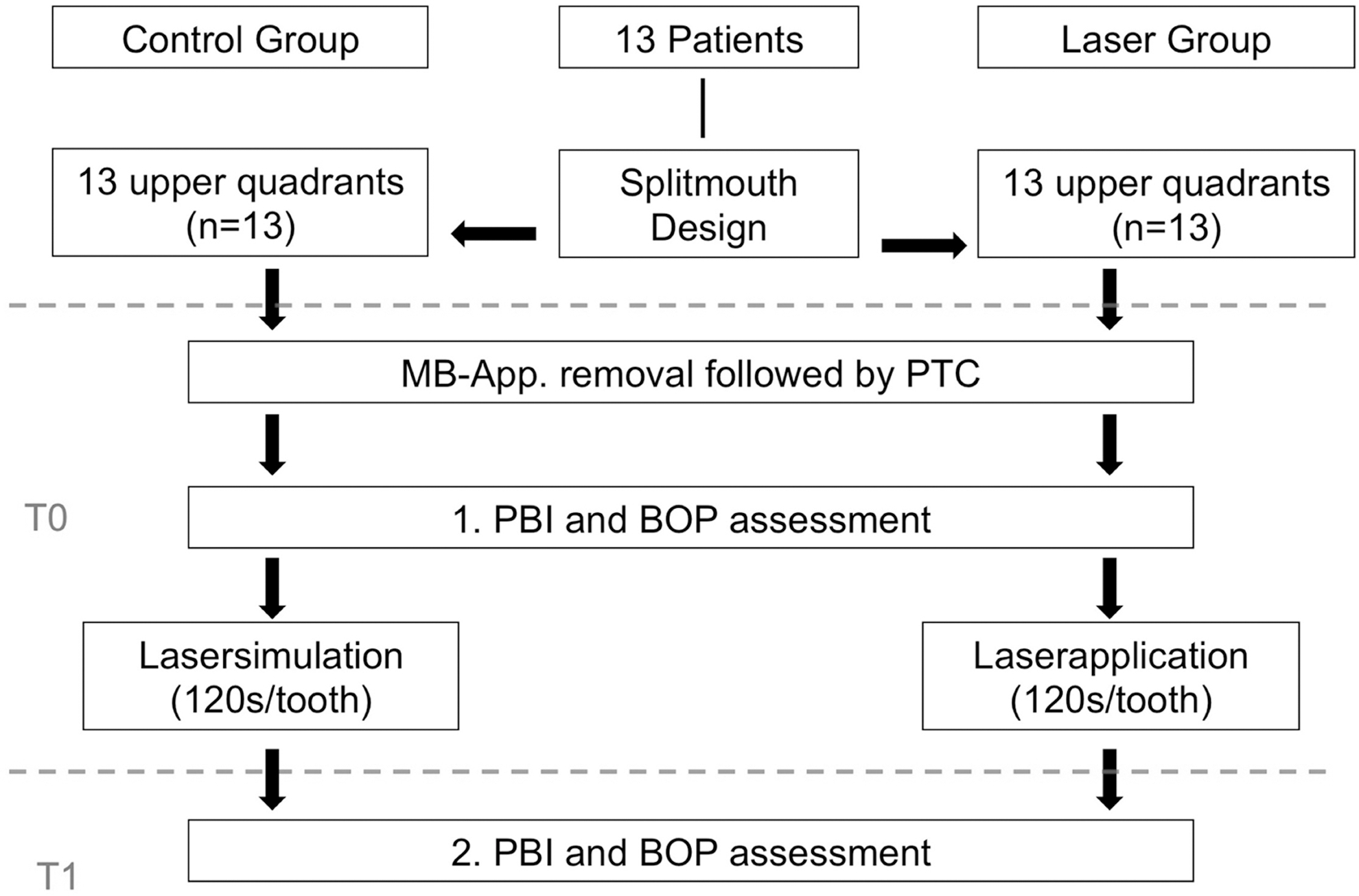
Study design with group assignment. MB-App: multi-bracket appliance; PTC: professional tooth cleaning; PBI: papilla bleeding index; BOP: bleeding on probing; T0: day of MB-App. removal, first PBI and BOP assessment, laser application (laser group) and laser simulation (control group); T1: second PBI and BOP assessment 5 days after laser application (T0). Dotted line objects study relevant procedures at T0 and T2.
The PBI was assessed at the same time point (T0) by the same blinded investigator (M.S.) by evaluating two measuring points per tooth (mesial and distal papilla) from tooth 16 to 26. The PBI was assessed using the same periodontal probe as the BOP. The PBI score ranges from 0 (no bleeding/inflammation-free gingiva) to 4 (diffuse bleeding/serious inflammation of the gingiva). 32 –34
BOP and PBI were assessed again by the same examiner (M.S.) 5 days after PBMT (time point T1). The investigation at T1 was again performed on a blinded basis, as the investigator (M.S.) was not aware at any time of which quadrant PBMT had been administered in. To allow comparison between the values measured, all of the measurements were performed by the same experienced practitioner (M.S.) in all of the patients. The examiner received calibration training at the start of the study.
Treatment procedures, randomization, and blinding
The study was conducted using a patient-blinded split-mouth design, with treatment being administered in the maxilla alone. On a randomly assigned basis, each patient received adjuvant PBMT in one maxillary quadrant (laser side; n = 13), but not in the other (control side; n = 13). The patient did not know at any time, which quadrant received laser treatment and which not. A computer generated random table was used to allocate both the respective treatment procedure and sequence of treatment performance to each patient. Photomodulation therapy on the laser side was performed using a diode laser (power = 100 mW, Helbo®; Bredent Medical Co., Walldorf, Germany) with a wavelength of 660 nm and a power density of 100 mW/cm2. Power density is defined as a spot size of 1 cm2 at tissue, and calculated from the beam divergence from the laser aperture (Fig. 2). On the basis of results from preliminary tests, the irradiation time per laser application point was set to 20 sec with an energy density per application point of 2 J/cm2 (Energy per application point = 2 J). The definition of application points is based on a recently published study (Fig. 2). 31 The laser was applied to teeth 1–6 on the laser side, perpendicular to the upper third of the buccally and orally attached gingiva in the central region and in the mesial and distal papilla. With 26 application points, a total irradiation time of 8 min 40 sec was reached with a total dose of 52 J/cm2 (Total energy = 52 J). As the laser system does not have an integrated timer, the exposure times per application point were checked using a stopwatch. To avoid distortion of the results as a result of the patients' oral hygiene behavior, the laser application was simulated on the control side in the same way as on the laser side, but with the laser turned off. A sterile single-use laser head (Helbo 2D Spot Probe; Bredent Medical Co.), equipped with a built-in spacer to keep the laser source 8 mm away from the gingiva, was used in each patient (Fig. 3). According to the manufacturer, the fixed distance of 8 mm from the exposed gingival surface ensures optimal effectiveness of the laser application. The PBMT procedures were always performed by the same experienced practitioner (S.S.), who could not be blinded.

Representative example of a patient with buccal laser application positions (30) marked in the upper right quadrant.

Example of rectangular laser application with the integrated distance control appliance after bracket debonding and professional tooth cleaning.
Statistical analysis
A power-analysis was performed before the study. Therefore, the effect size was set to 0.8 according to Cohen. 35 For an alpha-error of 0.05 and a power of 0.8 a sample size of at least 12 subjects was calculated.
Statistical analysis was carried out using SPSS Statistics for Windows, version 17.0 (2008;SPSS, Inc., Chicago). Normal distribution was tested using the Shapiro–Wilk test. As a normal distribution was not present in any cases, nonparametric tests were then used for further analysis: Mann–Whitney U tests were performed to test intergroup differences (control side vs. laser side) and Wilcoxon tests were used to analyze changes in the corresponding intragroup BOP measurements (T0 vs. T1). The distribution of the PBI values was analyzed using the chi-squared test. The significance level for all tests was set at p < 0.05.
Results
All of the included patients were monitored throughout the entire duration of the study. No adverse effects were observed, and none of the patients reported any discomfort during or after the laser application. For both assessed clinical parameters (BOP and PBI) changes could be observed with respect to the treatment procedure and evaluated time points (p < 0.05).
Bleeding on probing
No statistically significant differences were observed when the BOP values for the control side were compared with those for the laser side at time point T0 (p = 0.335). The BOP values decreased to statistically significant values on the laser and control side between time points T0 and T1 (laser: p = 0.001; control: p = 0.005) (Fig. 4 and Table 1). When the control side was compared with the laser side at T1, the BOP values were found to be significantly lower on the laser side (p < 0.034) (Fig. 4 and Table 1).

Box plot showing BOP values in the control group and laser group at T0 and T1 (5 days after laser application). BOP values decreased significantly between T0 and T1 in both groups (p < 0.05). BOP values were significantly lower in the laser group in comparison with the control group at T1 (p < 0.05).
Different indices (a*; b*; c*) indicate statistically significant differences (p < 0.05).
T0: before low-level laser therapy.
T1: 4–6 days after low-level laser therapy.
Papilla bleeding index
No statistically significant differences were observed when the distribution of the PBI values for the control side was compared with that for the laser side at time point T0 (p = 0.235). The PBI values decreased to statistically significant values on the laser and control side between time points T0 and T1 (laser: p = 0.000; control: p = 0.002) (Fig. 5 and Table 2) with statistically significant lower values on the laser side at T1 (p = 0.028) (Fig. 5 and Table 2).
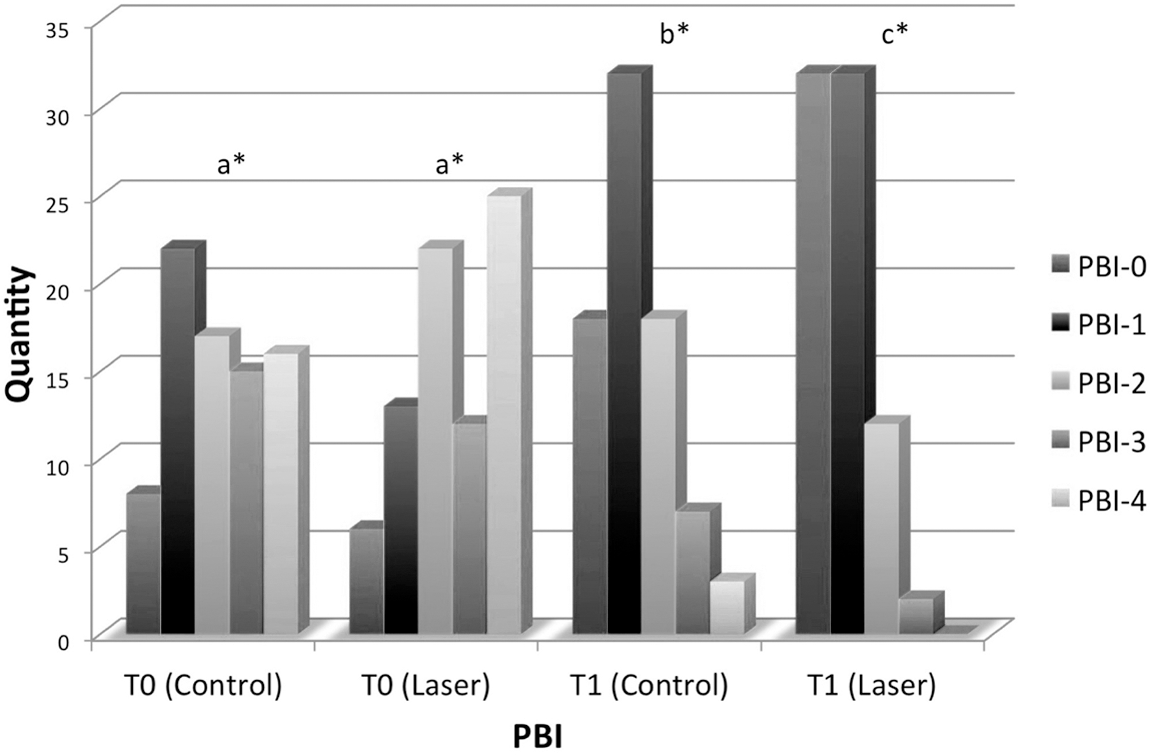
Bar chart comparing PBI values in the control group and laser group at T0 and T1 (5 days after laser application). PBI values decreased significantly between T0 and T1 in both groups (p < 0.05). PBI values in the laser group were significantly lower than those in the control group at T1 (p < 0.05). Different indices (a*, b*, c*) indicate statistically significant differences.
Different indices (a*; b*; c*) indicate statistically significant differences (p < 0.05).
T0: before low-level laser therapy.
T1: 4–6 days after low-level laser therapy.
PBI, papilla bleeding index.
Discussion
No statistically significant differences were noted when the BOP and PBI values on the laser side and control side were compared at time point T0. The initial situation was the same on both sides. A statistically significant improvement in the BOP and PBI values were observed after removal of the brackets and the biofilm on both sides between time points T0 and T1 (Fig. 5). Other studies have also confirmed that the healing process in gingivitis is directly associated with reduction of the biofilm. 36 Gingivitis is thus a curable disease, based on the elimination of etiological factors (brackets and biofilm). 37,38 The statistically significant decrease in BOP and PBI values between T0 and T1 thus corresponds to the natural healing process of the gingiva after removal of the brackets and the professional tooth cleaning carried out.
When the BOP and PBI values were compared at T1, the values for the laser side were found to be statistically significantly lower than those for the control side. The use of adjuvant PBMT, in combination with mechanical removal of the brackets and the removal of the biofilm through professional tooth cleaning, thus leads to significantly better and faster healing of gingivitis induced by a multi-bracket appliance (Fig. 5). There are no statistically significant differences between PBI-values on the laser and control side at T0. Nevertheless, Fig. 5 shows tendentially higher PBI-values on the laser side at T0. Thus, the statistically significant lower PBI-values of the laser side at T1 underline the positive effect of PBMT in this study again. The hypothesis for the study was confirmed. A study by Igic et al. also supports this result; the authors concluded that adjuvant PBMT leads to an improvement in the healing process in chronic gingivitis in children. 31
The precise biological effects of PBMT at the cellular level are still a matter of controversy, but in the last years much progress has been made in elucidating signaling pathways and chromophores. 39,40 It has been observed that PBMT irradiation has anti-inflammatory, analgesic, and cell-stimulating effects. PBM reduces levels of proinflammatory cytokines in activated inflammatory cells. 39 The increase in blood flow induced by PBMT does not result from a heating effect, but is rather the result of increased or normalized homeostasis in the tissue metabolism. 31,39,40 It has also been claimed that PBMT leads to stimulation or correction of disturbed cell function or an increased production of basic fibroblast growth factor could be one of the mechanisms by which PBMT wound healing. 41 The cellular effects of PBMT cannot be explained on the basis of the present study's results, but they do confirm the positive effect on the gingival healing process.
The split-mouth design used in this study was preferable to a parallel design, as it enables a balanced distribution of across- or within-patient confounders in the randomization units with regard to oral hygiene and the degree of gingivitis present.
According to the manufacturer's instructions, optimal effectiveness is achieved with the laser at a distance of 8 mm from the gingiva. This distance is ensured by using the spacer integrated into the device. A pain-reducing effect during use of orthodontic separators in early mixed dentition has also been identified using the same laser system with the integrated spacer. 21 Use of a spacer with a defined distance can be recommended on the basis of the reproducibility of the present study procedure and the results. Due to the large distance and lack of direct irradiation on the control side, it is not possible for the PBMT to have any local effects on the gingiva on the control side. It was not investigated in this study whether or to what extent greater or smaller distances between the laser and the gingiva may influence the efficacy of PBMT treatment with the present laser system.
The various experimental parameters used in different studies on PBMT tend to differ. No potential injuries due to PBMT have been reported in the literature. Different laser systems with different wavelengths and energy levels were used in the published studies. The only study that investigated the effect of adjuvant PBMT in children with gingivitis used a different laser system with a different wavelength and energy level. 31 The issue of which wavelength and energy level is most effective in gingival treatment has not yet been resolved. The laser system used in this study operates at a wavelength of 660 nm with an output power of 100 mW. This corresponds to the wavelength and power range used in other studies that have already led to pain reduction during orthodontic tooth movement and orthodontic separation. 21,42,43 A tissue response has thus already been demonstrated. On the basis of the present study results, it is not possible to determine whether repeated PBMT or an increase in the output power used might lead to further improvement of the healing process in patients with gingivitis. This would be an interesting issue for further studies to investigate.
Conclusions
It can be concluded that, on the basis of these results and study parameters, adjuvant PBMT is able to accelerate the healing process in patients with gingivitis induced by multi-bracket appliances.
Footnotes
Acknowledgments
The authors thank Helbo for providing the laser device.
Author Disclosure Statement
No competing financial interests exist.