
Abstract
Introduction
O
Laser irradiation can result in excessive destruction of tissue due to heat accumulation. 3,4 Therefore, irradiation techniques such as short pulsed irradiation and cooling devices have been developed to control heat accumulation. 4 However, wounds in the oral cavity heal faster with less scar formation or resultant contracture, compared to skin wounds, 5,6 and ulcer formation in the oral cavity often tends to be neglected. 7 However, deep or wide intra- or postoperative ulcer formation can induce trismus, 8 a narrow and shallow oral vestibule, 9 reduced tongue mobility, 10 and reduction of a subsequent treatment effect, in addition to the side effects for cutaneous lesions. Therefore, such side effects must also be avoided as much as possible in the oral cavity.
To achieve safe therapy, there is a need to control laser-induced heat, 2 –4 thereby sparing the covering mucosa (the “epithelium”) as much as possible. 8,11 –13 To prevent heat accumulation and resultant side effects, we have used a multiple pulsed spot irradiation technique, the so-called “leopard technique (LT)” (Fig. 1), for superficial vascular lesions. 13 This technique was originally proposed by Ohshiro 13 for laser treatment of nevi, in which the irradiation spots are separated (like a leopard marking) using a defocused beam in single-pulsed wave mode. This avoids thermal concentration at the same spot and spares the epithelium. 13
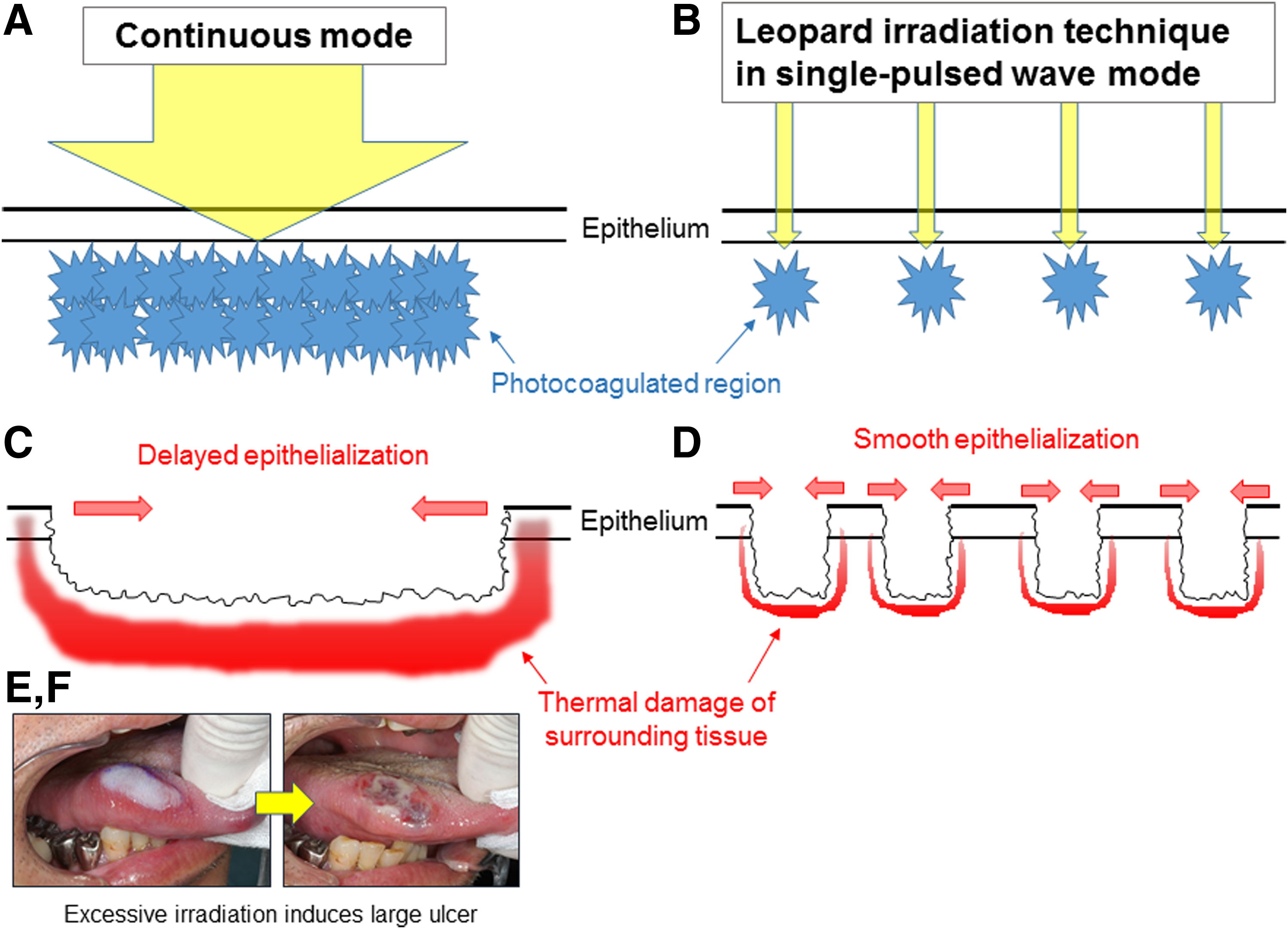
Schema of thermal effects of laser irradiation in continuous conventional mode
LT could provide less invasive and safe treatment with satisfactory outcomes and a lower incidence of adverse events compared to continuous mode irradiation. Further, we have also found that effective resolution could be achieved for massive lesions using a combination of LT for the superficial layer and intralesional photocoagulation (ILP) for the deep layer. 14,15 ILP is originally effective and safe for treatment of a massive vascular lesion. 14 –19 In this technique, laser energy is delivered directly into thick deep lesions through a bare fiber delivery system, thereby maximizing the effect on deep components and minimizing epithelial damage without direct contact with the cutaneous or mucosal surface.
In this study, we report our surgical procedures and review the results of treatment using these approaches.
Patients and Methods
Patients and lesions
The protocol used in this work was reviewed by the institutional review board (IRB) in each facility. The study was performed as a retrospective review of clinical records for 63 Japanese patients (18 male, 45 female, age 5–81 years) with 64 vascular lesions treated using the LT (Table 1), at Tokyo Medical and Dental University, and National Center for Global Health and Medicine. Written informed consent was obtained from all patients before the operation.
Diagnosis was made according to the classification of the International Society for Study of Vascular Anomalies, 20 based on physiological findings, medical history, and findings on magnetic resonance imaging (MRI) and ultrasonography. Fifty-seven patients had venous malformation (VM), four had non-involuting congenital hemangioma, and three had capillary malformation.
Leopard technique
The outline of the lesion was first marked on the mucosa with a safety margin of 1–2 mm with ink, and 2% lidocaine without epinephrine or with epinephrine 1:200,000 was injected to more than 1 cm around the lesion. First, the power and pulse duration were adjusted in test irradiation to give optimal irradiation conditions that gave slight shrinkage and decolorization, but not blanching. 13 –15 A Nd:YAG laser of wavelength 1064 nm (VersaPulse Holmium/Nd-YAG Laser Dual Wave length model; Lumenis Ltd., Yokneam, Israel) with a 0.55 mm fiber was applied to the lesion at power of 10 W and pulse duration 20 ms, which were then changed gradually. Nd:YAG laser energy was delivered in a “spot” manner, with each spot made with single-pulsed wave irradiation. 13 –15 The margins for each application were separated by at least 3 mm to avoid overlap due to scattering and resultant necrosis. 13 –15
Combination technique of LT and ILP
For massive lesions of thickness >1 cm or those with a thick covering mucosa, LT was combined with ILP to increase the efficacy of lesion removal because of the limited energy penetration of the laser. 14,15 The superficial layer was first treated by LT as described above and then the deep layer was treated by ILP, as described by Miyazaki et al. 14,15 In ILP, the mucosa adjacent to the lesion was punctured with a needle, and bare fiber (0.55 mm) was inserted submucosally into the lesion. ILP was performed in continuous mode with power from 10 up to 15 W with or without ultrasound (US) navigation and repeated in fan-like pattern until all the areas of the lesion had been treated. 14 –19 The treatment session was finished when visible shrinkage of the induration was palpable, and/or all parts of the lesion showed an increase in the echo level on US scan.
Patients were followed closely for 1 month and then monthly to determine the response and assess complications. In cases of unsatisfactory regression, one or more additional treatment sessions were conducted. A course of antibiotics was administered for 3 days to prevent infection, and painkillers were administered as needed.
Assessment
The response to treatment was determined by clinical examination by one observer and from photographic records, ultrasonography, and MRI findings. Outcome was assessed by change of color, change in size of the lesion, presence of postoperative deep ulceration, presence of paresthesia, and the number of painkillers required per session. The change in size was classified by Vlachakis et al.s' criteria 4 as excellent, good, moderate, and poor for a reduction of 90–100%, 50–89%, 20–49%, and 0–19%, respectively. Ulceration was defined as a defect that was not epithelialized within 2 weeks or in which a submucosal or muscle layer could be seen after necrotizing tissue was detached.
Results
The results are summarized in Tables 2 and 3. All treated lesions were reduced in size, with no increase in size observed after initial edema subsided. Of the 63 patients, 46 patients with 47 lesions completed the whole schedule as initially planned and had a follow-up period of more than 1 year (Table 2). The 46 patients were followed for a minimum of 14 months after receiving their final treatment. Multiple sessions were needed in many cases. Outcomes were satisfactory with respect to the volume reduction (Table 3); low incidence of postoperative deep ulceration of 6.38% (3/47) (Table 4), including cases treated with a combination of LT and ILP; smooth healing with inconspicuous scars, and disappearance of preoperative hemorrhage or pain in all cases in which the initially planned treatment schedule was completed. Five cases showed transient taste or sensation disturbance, but all resolved within 6 months. Four of these cases were treated using the combination technique. In 24 cases treated by noncontact leopard irradiation alone, the patients did not need to take a painkiller. The following sections provide details of four typical cases.
Average number of sessions per case.
ILP, intralesional photocoagulation.
Case 1
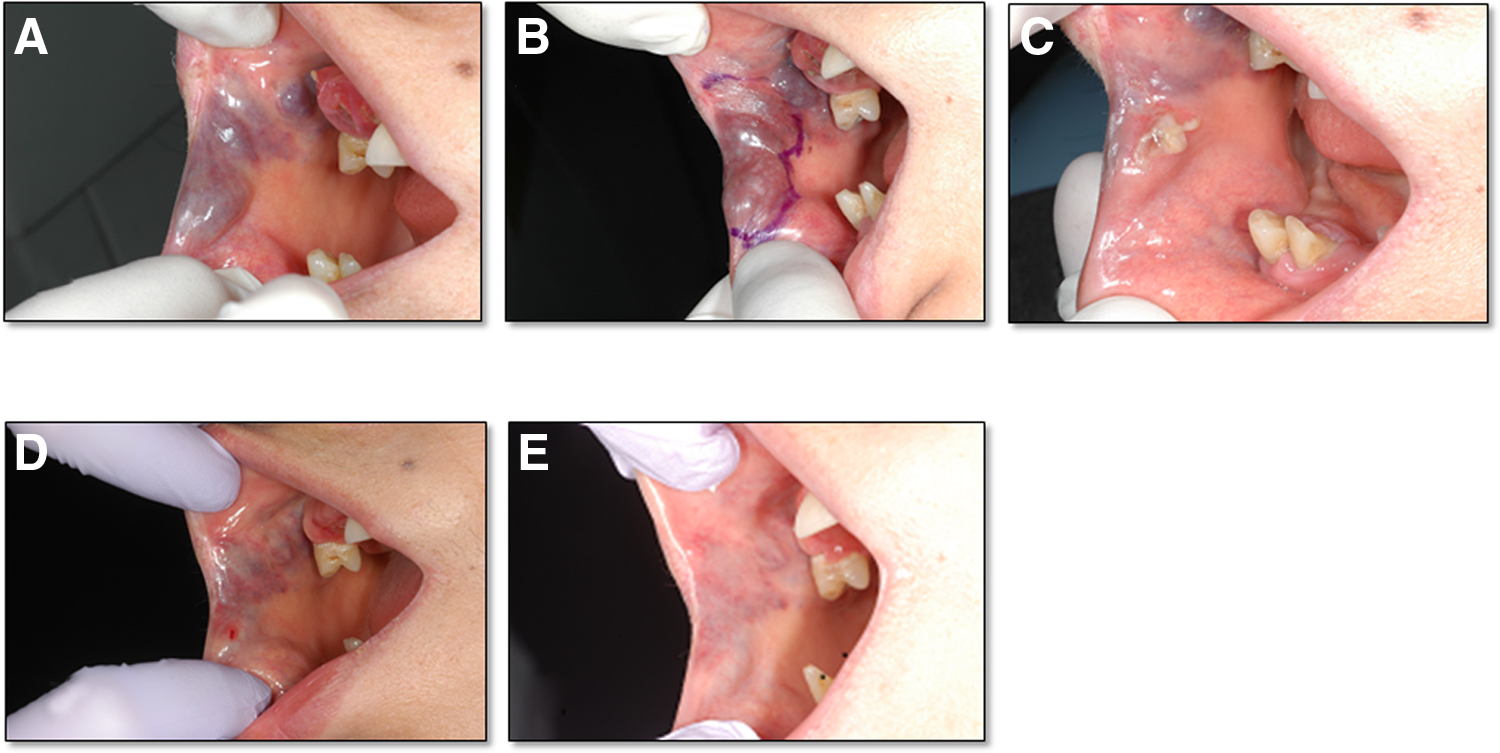
The patient was a 57-year-old man who presented with VM of the tongue (Fig. 2A). The lesion was superficial and ∼25 × 10 mm in diameter. The LT at 569 J was used for treatment in single-pulsed wave mode (power 15 W, power fluence at the lesion surface of ∼823 W/cm2, pulse duration 100–200 ms) with slide glass compression technique to increase the treatment efficacy of deep layer by reducing the dimension from the surface to the deep layer (Fig. 2B). 21,22 The session was finished when visible shrinkage of the lesion was apparent, and irradiated spots were barely observed just after irradiation (Fig. 2C). Only a small area developed superficial erosion at 1 week after treatment at a site where the mucosa covering the vascular lesion was very thin (Fig. 2D), and this healed without scarring. The patient did not need to take a painkiller. The lesion gradually reduced in mass over several months and showed incomplete regression at 6 months after the first session (Fig. 2E). The residual lesion was treated in the same manner in the second session and was completely resolved (Fig. 2F). The patient experienced slight postoperative pain and swelling, but did not need to take painkiller in either session. A year after the second session there was no residual lesion or scar formation, and underlying tissue remained soft to palpation. We estimated 100% resolution, and our final assessment was “excellent.”

Case 2
The patient was a 54-year-old female with a wide VM extending from the submucosal area of the right buccal mucosa to the angle of the mouth and further into the vermilion (Fig. 3A). She was treated in the same manner as case 1 using LT (power 15–20 W, power fluence approximately 823–1097 W/cm2, and pulse duration 200 ms). The lesion was treated with 215 J of total energy. Multiple inconspicuously decolorized dots were observed just after treatment (Fig. 3B). No significant complications were noted during and after the operation. The patient experienced only slight postoperative pain and swelling. Only a small area developed superficial erosion with fibrin deposition at a site (Fig. 3C) where the mucosa covering the lesion was very thin, and this healed without scarring. The lesion gradually reduced in mass over several months. Optical findings 6 months after the first treatment showed incomplete regression of the mass (Fig. 3D). The residual lesion was treated in the same manner in the second session. Six months after the second session, there was incomplete but satisfactory regression of the mass (Fig. 3E), which was estimated at about 80% resolution. Our assessment after the two sessions was “good.”
Case 3
The patient was a 13-year-old girl who presented with a painful and enlarging VM (45 × 35 × 20 mm3) on the left buccal mucosa (Fig. 4A). As the lesion was thick, it was treated with a combination of LT and ILP. At first, the superficial layer was treated by LT (power 15–20 W, pulse duration 200 ms, and power fluence approximately 1310–1747 W/cm2). Then the mucosa was pierced directly by a 0.55-mm fiber adjacent to the lesion, and a fiber was inserted into the lesion. ILP was performed for the deep layer of the lesion (power 15 W, total energy 970 J) (Fig. 4B). The patient experienced moderate postoperative pain and swelling, but optical findings 1 week after treatment showed superficial erosion only in a very small area (Fig. 4C). There was no delay of wound healing and no other significant complication, such as paresthesia or paralysis of the lips, scarring, and resultant contraction. The lesion gradually reduced in mass over several months. Clinical examination 4 months after the first session (Fig. 4D) showed marked regression of the mass. The residual lesion was treated in the same manner as the first session (Fig. 4E). A total of three sessions were performed, and clinical observation 1 year after the third session (Fig. 4F) showed satisfactory regression of the mass, estimated at more than 90% resolution, and our assessment was “excellent.” The patient had relief from spontaneous pain.

Discussion
The Nd:YAG laser or diode laser has high penetration, but the degree and extent of tissue coagulation are not immediately obvious. Since this often becomes clear only when tissue sloughing occurs within 3–7 days and can be more extensive than expected, 1 –4 precautions are required. 1 –4 Ohshiro proposed the concept of multiple spot irradiation focusing on sparing the epithelium in the 1980s. 13 In this technique, separating irradiation spots from one another with single pulse can spare the epithelium between spots. Epithelialization of the treated areas then takes place smoothly from the margins of the remaining untreated normal skin. Once the new epithelium has matured and stabilized, the remaining untreated area can be treated, which in turn is successfully epithelialized from the new epithelium covering the previously treated area. 13
We applied LT to oral vascular lesions and achieved satisfactory results in all cases. In contrast to irradiation in continuous wave mode, which caused ulceration in all treated cases, LT resulted in a marked decrease in the incidence of postoperative ulceration and the need for painkillers, without loss of the therapeutic effect. Another advantage of LT is that the amount of energy can be adjusted as needed while observing the status of the lesion. Thus, irradiation can be terminated based on a color change or slight shrinkage of the lesion. Further, even if erosion occurs in the irradiated area, the erosion is shallow and limited, and smooth epithelialization can occur.
Dixon et al. 1 and Suen 23 subsequently reported similar techniques to that described by Ohshiro, as the “spot fashion” and “multiple pulsed spots” techniques, respectively. The fundamental differences between our LT and these techniques are the setting of optimal irradiation conditions by titering in test irradiation. This allows excessive irradiation to be avoided. To avoid loss of therapeutic efficacy, we use a Nd:YAG laser (1064 nm). The wavelength is less absorbed by melanin or hemoglobin compared with that of a dye laser or KTP laser; is not absorbed at the surface, which spares covering mucosa; and has good tissue penetration. However, there is a concern in treatment of deep and massive lesions using the LT. Despite the use of a Nd:YAG laser, the deep layer cannot be reached by transmucosal irradiation like LT because tissue penetration is limited. Some thick lesions can be treated transmucosally by slide glass compression, but complete resolution of a deep lesion using only a transmucosal technique is likely to require many sessions or excessive irradiation in each session, which can induce ulceration.
Apfelberg first described the clinical use of ILP for treatment of deep vascular anomalies, 16 and many surgeons have subsequently reported successful results using this method. 14 –19,22 To date, we have obtained satisfactory results in all cases in which we have used ILP for treating large or deep vascular lesions in the oral cavity. In a series of the treated cases, we recently found that addition of LT to ILP increased lesion regression. 14,15 The combination of LT and ILP enables treatment of the superficial and deep layers of massive lesion in the same session. The results of this approach are more effective in terms of removal of the lesion, and the incidence of postoperative ulceration in our cases treated with the combination technique was 12.5% (3/23), 17 which was similar to the rate using ILP alone. Smooth healing without scarring occurred in all cases. Thus, some lesions may be treated more effectively using the combination technique than by LT or ILP alone.
Compared with conventional transmucosal irradiation in continuous mode, the number of treatments required for sufficient removal of a lesion is likely to be increased using the LT. However, safety, reduced discomfort, and prevention of scarring take precedent over reduction of the treatment period. The patients are provided detailed information on the treatment, and none refused several sessions, since they felt only minimal discomfort in each session. Our new approach is simple and safer than the conventional technique in continuous mode. The treatment is generally well tolerated, and patient satisfaction to date has been excellent. We suggest that the LT of laser therapy is a promising approach for safe and minimally invasive resolution of vascular lesions without scarring and loss of normal shape, sensory feel, and function of oral tissue.
Footnotes
Acknowledgments
Funds were from institutional sources only.
Author Disclosure Statement
No competing financial interests exist.