
Abstract
Introduction
F
Conventional techniques for de-epithelialization include scalpel, abrasion with diamond bur, or a combination of the two. However, despite being simple, inexpensive, and effective, these techniques are invasive and may produce unwanted side effects such as uncontrolled hemorrhages (scalpel) or unwanted abrasion or pitting of the tissue. 2 The rationale for laser de-epithelialization stems from the need for a minimally invasive technique, which guarantees efficacy. Application of laser in de-epithelialization procedure ensures effectiveness, precision, minimal or no side effects, and time efficiency in terms of both the procedure duration and wound healing. 3
Laser de-epithelialization is beneficial in shaping gingival tissue layer by layer in a minimally invasive way. This has been utilized in gingivoplasty, 4 implantology for emergence profile management, 5,6 vaporization of oral leukoplakia, 7 periodontal pocket debridement, 8 and gingival depigmentation. 9 Another common procedure in periodontal therapy is tooth recession coverage in which the epithelium is removed on the palatal side before connective tissue grafting. 10 These therapies can be done conventionally with a surgical blade 11 or alternatively with a diode laser. 12
In all these procedures, Er:YAG laser can be successfully applied with beneficial effects on the healing process. 8 This type of laser generates laser beam at 2940 nm wavelength, which is very well absorbed by water. Moreover, the beam of Er:YAG laser is absorbed in the superficial layer of the tissue and does not penetrate or scatter more than several microns. 13 The speed, direction, and type of movement are usually generated by the operator's hand. However, a new Digitally Controlled Laser Handpiece (DCLH) allows ablating the tissue layer by layer without operator's hand movement.
DCLH allows you to choose the pattern shape, for instance circular, rectangular (line or square), and hexagonal, with a size of the treatment area from 2 to 6 mm in increments of 0.5 mm. Also, this handpiece allows selecting the treatment surface or only its border as well as the number of laser passes. Other parameters of the laser beam (energy, frequency, and mode) are set at the same way as with other standard laser handpieces. The scanning technique for layered and uniform ablation of soft tissue may be used for de-epithelialization during periodontal surgery. Particular attention should be paid to preventing overheating of the bone when applying high-power lasers during surgical procedures in both soft and hard tissues. Due to low thickness of the palatal mucosa, the heat is being transmitted by the subepithelial connective tissue to the bone. Eriksson and Albrektsson 14 found that increasing the temperature of bone tissue by 10°C for 60 sec causes permanent changes in the bone structure. Therefore, a tissue temperature gradient (ΔTa) below 10°C should be regarded as optimal and safe.
The aim of the present study was to measure the temperature increase after de-epithelialization of soft tissue with Er:YAG laser by a conventional or a new DCLH scanning handpiece. Thermal injury of the samples has been assessed by histological analysis.
Materials and Methods
The study was performed on six cadaver mandibles of 10-month-old pigs. Porcine mandibles were chosen due to similarity to human physiological structure. The used specimens were homogeneous in viability and in quality of gingival tissues. Two different Er:YAG laser handpieces were used to remove the epithelium: DCLH X-Runner and HO2 (Fotona, Slovenia) (Fig. 1).

Digitally controlled laser handpiece X-Runner and HO2 (Fotona, Slovenia). Red arrow indicates DCLH, white arrow indicates laser beam passage.
Samples preparation
The research included a total number of 114 samples (n = 114) sized 6 × 6 mm and diameter 1.5–2 mm (measured using periodontal probe), which were collected from the attached gingiva of the alveolar process of the porcine mandibles, using 15°C scalpel blade. Next, the samples were randomly divided into six groups (n = 19) according to various laser parameters and types of handpieces (Table 1). Ethical approval was not required for this animal ex-vivo study.
Surgical procedure
The samples were de-epithelialized by means of Er:YAG laser (LightWalker, Fotona, Slovenia) that operates in noncontact mode. The specimens were irradiated with water spray at a distance of 10 mm using HO2 handpiece moved by the operator from side to side of the collected samples for 16 sec. The operator used 2.5 × magnification loupes (Sandy Grendel Swiss Loupes) for visual examination of the process. For the X-Runner handpiece, the samples were irradiated with water spray by holding the handpiece at a distance of 13 mm from the specimen with no movement of the operator's hand. The time of single irradiation of each sample sized 6 × 6 mm was 6 sec (one laser beam passage) (Fig. 2). The speed of samples irradiation was 2.25 and 6 mm2/sec for HO2 and DCLH, respectively. The lasing time was controlled by the operator with HO2 handpiece or by Er:YAG laser software when using X-Runner.

The time of single irradiation of each sample (a one laser beam passage).
Temperature measurement
The specimens were placed in a container with water at a temperature of 22°C for 20 min, the temperature was monitored with a Medicare Clinical Products Gold mercury thermometer (Medicare Products, Inc., New Delhi, India). Each sample was removed from the container with water and placed on a K Thermocouple Probe P1, type TP-01 (Zhangzhou Weihua Electronic Co., Fujian, China) attached to the wooden plank. The temperature of the samples during de-epithelialization was measured by means of a calibrated digital Thermometer CHY802 W (CHY Firemate Co., Tainan City, Taiwan). The thermocouple was covered with thermal conductive paste ART.AGT-057 with conductivity of 0.243 Cal/g K to ensure good thermal flow. This paste was used by two coauthors of this study in their previous research (AG Termopasty, Sokoly, Poland). 6
Study groups
The study specimens (n = 114) were divided into six groups: G1 (n = 19), G2 (n = 19), G3 (n = 19), G4 (n = 19), G5 (n = 19), and G6 (n = 19).
G1 Group: Er:YAG laser, 2940 nm (LightWalker, Fotona, Slovenia), tipless handpiece: HO2, operation mode: pulsed wave (PW), power: 1.6 W in noncontact mode, energy: 80 mJ, frequency: 20 Hz, distance: 10 mm, power density: 176.12 W/cm2, spot diameter: 0.9 mm, and air/water spray: 2/2.
G2 Group: Er:YAG laser, 2940 nm (LightWalker, Fotona, Slovenia), tipless handpiece: HO2, operation mode: PW, power: 2 W in noncontact mode, energy: 100 mJ, frequency: 20 Hz distance: 10 mm, power density: 220.08 W/cm2, spot diameter: 0.9 mm, and air/water spray: 2/2.
G3 Group: Er:YAG laser, 2940 nm (LightWalker, Fotona, Slovenia), tipless handpiece: HO2, operation mode: PW, power: 2.8 W in noncontact mode, energy: 140 mJ, frequency: 20 Hz distance: 10 mm, power density: 308.14 W/cm2, spot diameter: 0.9 mm, and air/water spray: 2/2.
G4 Group: Er:YAG laser, 2940 nm (LightWalker, Fotona, Slovenia), tipless handpiece: X-Runner, operation mode: PW, power: 1.6 W in noncontact mode, energy: 80 mJ, frequency: 20 Hz distance: 13 mm, power density: 75.48 W/cm2, spot diameter: 0.9 mm, and air/water spray: 2/2.
G5 Group: Er:YAG laser, 2940 nm (LightWalker, Fotona, Slovenia), tipless handpiece: X-Runner, operation mode: PW, power: 2 W in noncontact mode, energy: 100 mJ, frequency: 20 Hz distance: 13 mm, power density: 94.23 W/cm2, spot diameter: 0.9 mm, and air/water spray: 2/2.
G6 Group: Er:YAG laser, 2940 nm (LightWalker, Fotona, Slovenia), tipless handpiece: X-Runner, operation mode: PW, power: 2.8 W in noncontact mode, energy: 140 mJ, frequency: 20 Hz distance: 13 mm, power density: 132.06 W/cm2, spot diameter: 0.9 mm, and air/water spray: 2/2.
Histological preparation
Thirteen samples (12 after de-epithelialization, 1 control) were randomly assigned for histopathological examination. Three samples were irradiated by HO2 handpiece at 80, 100, and 140 mJ/20 Hz. Nine samples were irradiated with X-Runner handpiece at 80, 100, and 140 mJ/20 Hz.
For the samples irradiated with DCLH, we have used three different settings, which resulted in removing one to three layers of the soft tissue. All samples were cut through the whole thickness of mucous layer. Microscopic slices were placed in 10% neutral-buffered formalin, dehydrated, and embedded in paraffin. The sections were stained with hematoxylin and eosin and evaluated by a general pathologist using BX51 optical microscope at 100 × magnification. The depth of the de-epithelialization was estimated in three categories: total destruction of the epithelium layer, partial de-epithelialization, and lack of lesions in the epithelial layer.
Statistical analysis
The obtained outcomes were analyzed statistically by means of Statistica 12 (StatSoft®, Tulsa) software. The mean increase in temperature of the implants has been assessed using one-way ANOVA test. Pair comparisons were carried out based on the Tukey's post hoc test at significance levels p = 0.05.
Results
Er:YAG laser irradiation results in inconsiderable thermal increase during the de-epithelialization
To examine the temperature rise in the specimens, the T01 thermocouple was used and placed below each sample. We found that DCLH has induced significantly lower temperature increase compared with HO2 handpiece at energy to frequency ratio of 80, 100, and 140 mJ/20 Hz. (p < 0.01) (Table 2).
Digitally control laser handpiece on Er:YAG laser results in lower thermal increase during de-epithelialization along with average power decrease
We obtained significantly higher mean temperature rise at 140 mJ/20 Hz in G6 group (mean 4.45°C) when compared with samples lasing at 100 mJ/20 Hz (G4 group, mean 1.72°C) or at 80 mJ/20 Hz, (G5 group, mean 2.62°C) group, respectively (p < 0.05). However, we found no differences in temperature increase for the HO2 handpiece regardless of lasing parameters used in this study (p > 0.05) (Fig. 3).
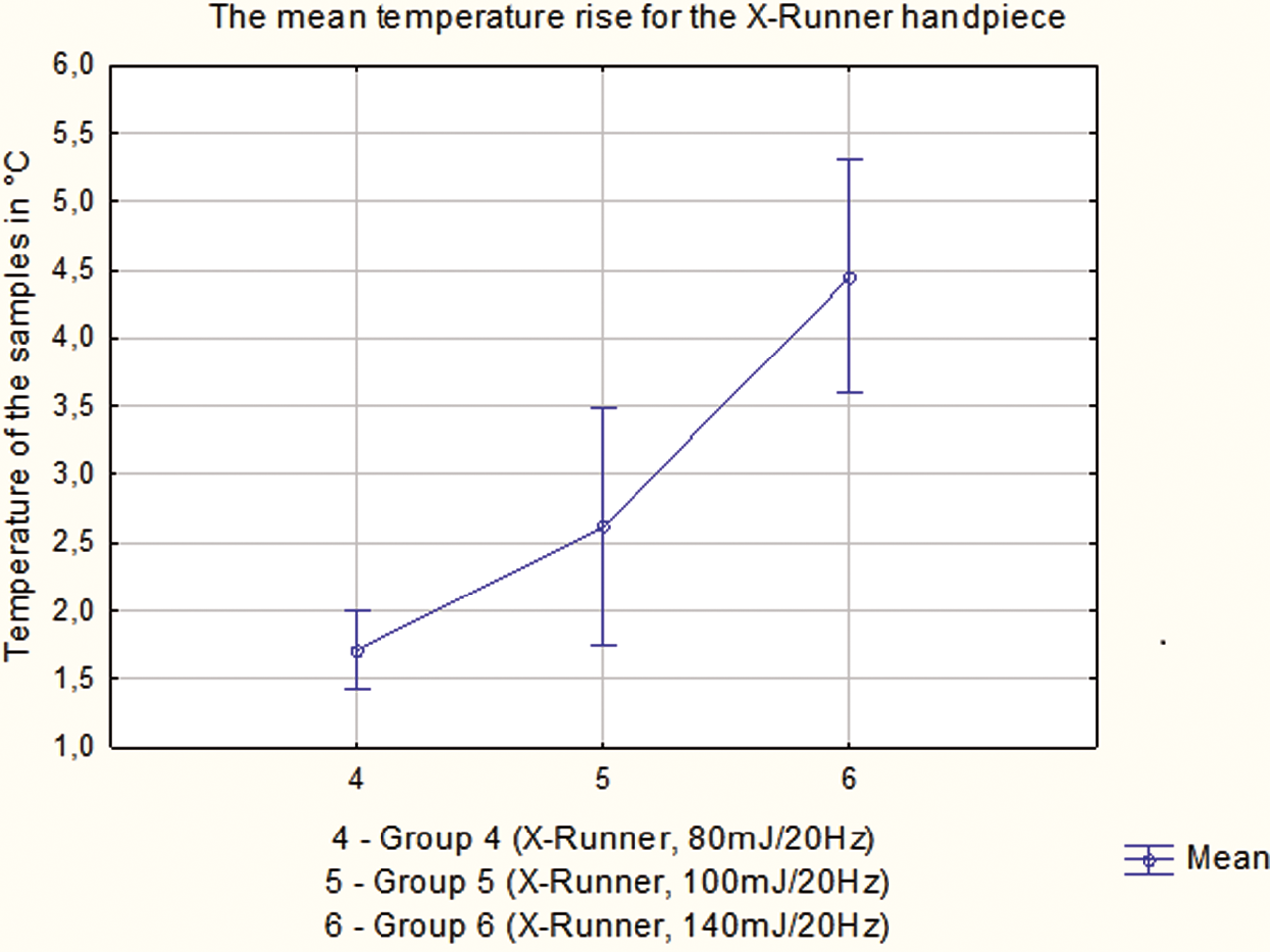
The mean temperature rise in Celsius (°C) measured by TP01 P1 k-thermocouple during de-epithelialization by means of Er:YAG laser with X-Runner handpiece.
Er:YAG laser allows to remove the epithelium with only superficial thermal damage
The results of histological examination highlighted total epithelium removal using HO2 handpiece at 100 and 140 mJ/20 Hz. Similar results were found after irradiation using DCLH X-Runner for two- and threefold lasing at 80, 100, and 140 mJ/20 Hz. Single lasing of the sample by means of X-Runner at all energy parameters used in this study left some part of the epithelium on the samples surface (Table 3).
H&E test, haematoxylin and eosin test.
The surface of the specimens lased with X-Runner tends to be smoother and more uniform compared with the samples irradiated with HO2 handpiece. Furthermore, thermal injury recorded in the target tissues was only superficial (Fig. 4).

The results of histological examination.
Discussion
Soft tissue de-epithelialization is performed in such therapies as periodontal pocket debridement, gingivoplasty, gingival depigmentation, or oral leukoplakia vaporization. The goal of periodontal therapy in periodontal pocket treatment is to enhance connective tissue growth to increase clinical attachment level. 15 Our study aimed at testing the temperature increase after de-epithelialization of soft tissue with Er:YAG laser by a conventional or a new scanning handpiece and a histological analysis of lased samples. The major finding of the study was that Er:YAG laser application at the indicated parameters for the tested handpieces allows de-epithelialization without significant damage to soft tissue. Compared to classical irradiation using traditional handpiece, significantly lower increase of temperature in treated samples was recorded when DCLH was used. Furthermore, the surface of the specimens lased with X-Runner tended to be more uniform and smoother compared with the samples irradiated with HO2 handpiece. These findings indicate higher efficiency and safeness of DCLH with Er:YAG laser at the indicated parameters.
For several decades now, lasers have been utilized to remove epithelium and proved more efficient than hand instruments. 1 Removal of the outer epithelium of the periodontal pocket provides sufficient time for connective tissue reattachment, as was described by Aoki et al. 16 The advantages of inflamed epithelium removal by Nd:YAG laser have been histologically reported by Nevins et al. 17 and Yukna et al. 3 The results of our study of Er:YAG laser de-epithelialization show a significantly lower temperature rise during epithelium removal after irradiation using X-Runner compared with HO2 handpiece at energy to frequency ratio of 80, 100, and 140 mJ/20 Hz. Moreover, we obtained the increase in temperature below 10°C for all tested samples, and observed no signs of carbonization or thermal injury, which corroborates the results reported by Romeo et al. 18 In this regard, our results confirm the outcomes obtained in other studies, which concluded that a tissue temperature gradient (ΔTa) below 10°C should be regarded as safe. 6,14
Our review of the available literature provides no record of comparison of ex vivo studies to evaluate histological and thermometric examination of soft tissue de-epithelialization using DSCH in periodontal tissues. The histological analysis revealed no stratified squamous epithelium after laser irradiation at fluence of 15.72 and 22.01 J/cm2 with HO2 handpiece after 16 sec, and similarly at fluence of 15.72 with DCLH after twofold lasing (12 sec). During the study, we found that scanning handpiece allows better control during soft tissue vaporization. Furthermore, the evaporated surface seems smoother compared to this irradiated surface with HO2 handpiece. Noncontact irradiation at a distance of 13 mm provides better visibility of the treated area. Superior effectiveness of Er:YAG laser operated in noncontact over a contact mode has been confirmed by Stubinger. 19
Layered vaporization of soft tissue with Er:YAG laser with DCLH constitutes a promising treatment in surgical and periodontal therapy for its predictability and improved visibility of the treated area. Determining the scope of vaporized soft tissue using the scanning head of Er:YAG laser could have positive clinical implications, reducing the depth of vaporization of tissue and improving postoperative healing, improving management of the most frequent potential malignant disorder, leukoplakia. Namour et al. 7 used superficial scanning with CO2 laser for complete superficial vaporization of oral leukoplakia. The results showed that laser vaporization constitutes a minimally invasive surgery and ensures significantly higher success rate. Histological analysis revealed that total removal of the epithelium is possible when the specimens were lased at ratio 100 and 140 mJ/20 Hz with water/air supply. Furthermore, the irradiated surface was vaporized evenly; both in the center part of the scanned target and at the border, which is a key factor in decreasing the risk of thermal injury of adjacent tissues.
Irradiation using lasers with a wavelength near 3000 nm allows vaporizing the soft tissue only superficially. The photons of Er:YAG laser are absorbed in the superficial layer of a soft tissue and do not penetrate or scatter more than several microns. 13,16 The shallow vaporization of the epithelium with only minimal thermal rise when using cooling system induces fast healing of the soft tissue because of minimal thermal damage. However, the other explanation of healing mechanism pathway could be found in ameliorating adenosine triphosphate (ATP) synthesis, which was suggested by Santana-Blank and Rodríguez-Santana. 20 The chromophore of Er:YAG laser is water present in biological membranes and body cells, so, Santa-Blank and Rodríguez-Santana 20 assumed that the interaction of light with nanoscopic layers of water may be essential to the photobiomodulation process. Moreover, water provides a pathway for near-, mid-, and far-infrared absorption and transportation, which increases the synthesis of ATP by facilitating Cox energy transfer in mitochondria. 21 The laser wavelength at 3000 nm corresponds to symmetric and asymmetric vibration of oxygen-hydrogen particles due to a high resonance frequency at this wavelength. 21 We would like to underline also a possible biostimulation of the epithelium using Er:YAG laser, despite that at higher wavelengths, photon energy and penetration are decreased.
Safe distribution of heat in tissues is of paramount importance when operating with high-power lasers in soft tissues. 22,23 However, temperature rise is conjunct with many laser- and operator-related variables (e.g., energy, power, pulse duration and repetition rate, duration of irradiation, tip type and size, distance to the target, and tip angulation). 24 The speed of operator's hand and the duration of irradiation have an impact on temperature gradient. These two variables could be regulated by using DCLH, which allows application of proper dose of energy in time on the target surface. Thanks to DCLH, temperature increase could be regulated in a predictable way. DCLH seems to offer many benefits in various fields of dentistry, especially in oral surgery and periodontology. Previously, Ozcelik et al. 12 described the use of a diode laser during a coronally advanced flap with de-epithelialized gingival grafts for root coverage. They showed the effectiveness of root coverage at 6 months and decrease in postoperative morbidity associated with palatal donor-site surgery performed using the wavelength of the diode laser. However, a superficial vaporization of the soft tissue with less thermal damage using Er:YAG laser compared with near infrared lasers 16 seems to be a better choice in de-epithelialization procedure. Additional studies using Er:YAG laser with DCLH are required to confirm the results of our study to evaluate clinical application in such procedures as root recession treatment, soft tissue depigmentation, or oral leukoplakia removal in human clinical studies.
Conclusions
It is well established that the use of erbium laser irradiation is a safe and effective method of soft tissue treatment. The use of Er:YAG laser with DCLH for soft tissue de-epithelialization is a relatively new procedure.
Our study showed that Er:YAG laser allows removal of stratified squamous epithelium after 16 or 12 sec at fluence over 15 J/cm2 with HO2 or DCLH handpiece, respectively. Although using both scanning and conventional handpieces helps to remove epithelium without excessive thermal damage, we found that temperature increase during irradiation by a scanning method was lower when we used DCLH. In this preliminary study, we achieved some promising results of suggesting that this procedure may be of much use in future. However, further trials on larger study groups are required.
Footnotes
Acknowledgment
This study was self-funded.
Ethical Approval
Separate ethics committee approval was not required for this animal ex-vivo study.
Informed Consent
The Informed Consent was not required for this animal ex-vivo study.
Author Disclosure Statement
No competing financial interests exist.