
Abstract
Introduction
D
Diode lasers, with a wavelength range of 810–980 nm, are primarily absorbed by melanin and hemoglobin, which are both known as chromophores and aid in the absorption of light. 12 Since the diode laser energy is absorbed well by pigmented tissues (melanin) and hemoglobin, it makes the laser a very good hemostatic agent in soft tissue surgery. Initiation of the diode laser fibers increases the efficiency of the soft tissue incisions produced by the laser because it results in the concentration of energy at the tip of the laser fiber, “hot tip,” which comes in contact with the tissue. 13 It has been shown that several different types of initiators can be used, including articulating paper, cork, and SureStep®. 6,13 The initiation of the fiber tip is achieved when the tip of the laser touches a dark chromophore. As soft tissue absorbs energy, it results in heat production and thus a rise in tissue temperature. It has been shown that initiators are effective for activation. However, there are no studies on this topic and there is no comparative study today, demonstrating the effects of initiators on soft tissue incisions using the same fiberoptic for tissue ablation. Therefore, the aim of this study was to determine the effect of various initiators on the thermal changes that occurred during incisions performed in soft tissues using a diode laser.
Materials and Methods
In this ex vivo study, incisions were made (10 mm in length and 3 mm deep) in fresh chicken breast (without skin) at room temperature (21°C). The incisions were performed by the same, calibrated, well-trained surgeon. A 975 nm diode laser (Alta; Dental Photonics, Walpole, MA) was used to make all of the incisions. All individuals involved in this study wore proper 975 nm goggle lens protection. The laser had a 320 μm fiber diameter. The glass fiber was cut with a ceramic scissor before every incision in accordance with the manufacturer's guidelines. Each incision occurred over a 10-sec irradiation period. Thermal changes that occurred during each incision, starting at 21°C, room temperature, were recorded by a T-Type MLT 1406, thermocouple device (ADInstruments Inc., Colorado Springs, CO). The thermoelement was placed 2 mm away from the incision site to avoid damage to the thermocouple tip and to accurately detect the temperature changes that occurred during each procedure. The thermoelement was inserted 3 mm deep into the soft tissue and was stabilized by a small piece of wax to avoid any movement during the incisions. The thermocouple was connected to two ML312, T-Type Pod conditioners (ADInstruments, Inc.) connected to a bridge amplifier, FE221 (ADInstruments, Inc.), which in turn was connected to a Power Lab-4/35 channel recorder (ADInstruments, Inc.). This enabled the continuous reading of the temperature changes that occurred during the soft tissue incisions.
Incisions were performed with and without an initiator. Cork, red and blue articulating paper (Bausch Articulating Papers “Arti-Check®” micro-thin-40μm; Bausch Articulating Papers, Inc., Nashua, NH), and SureStep methodology were the initiators used in this study (Fig. 1). The articulating papers consist of paper impregnated with oil, pigment, wax mixture, and following consistencies: pigment blue (10%), pigment red (10%), white mineral oil (50%), and natural waxes (10%). These products contain no hazard ingredient and there are no unusual hazards expected from normal use. 14
Initiators: blue articulating paper, red articulating paper, cork, and SureStep®.
The SureStep initiation was performed using the initiation tablet containing a carbon and TiO2 powder in an organic matrix. The initiation process occurred after deposition of the particles on the distal part of the fiber (first step) and the second step (“annealing”), when the fiber tip was kept in air with a temperature of quartz melting (up to 1800°C) for several seconds. In this final step, the carbon nanoparticles sintered with quartz, creating a robustly absorbing distal end.
Incisions made without an initiator were used as the control group (Fig. 2). The soft tissues were irradiated in a continuous wave mode at 3 and 6 W. Ten incisions were made for each group, resulting in a total of 100 incisions. In chicken breast, 10 incisions were made per group without an initiator (control group) at both 3 and 6 W, and 10 incisions were made using the cork, red and blue articulating paper, and SureStep initiators at 3 and 6 W (Figs. 3 and 4). Thermal changes (from room temperature to the maximum reached temperature determined as “delta T”) that occurred during each incision were recorded (Table 1), in degrees Celsius, by real-time thermography by thermocouples via LabChart computer software (ADInstruments, Inc.). A statistical comparative analysis between the groups was performed using Dunn's multiple comparison test with a p-value of 0.001 indicating a statistically significant difference.

Experimental design: two groups of 50 incisions, with a total of 100 incisions, were performed under 3 and 6 W power settings using no initiator and each of the four initiators.

Incisions in chicken breast without skin, 3 W power setting with no initiator and the different initiators. From left to right: 3 W no initiator, 3 W blue articulating paper, 3 W red articulating paper, 3 W cork, and 3 W SureStep.
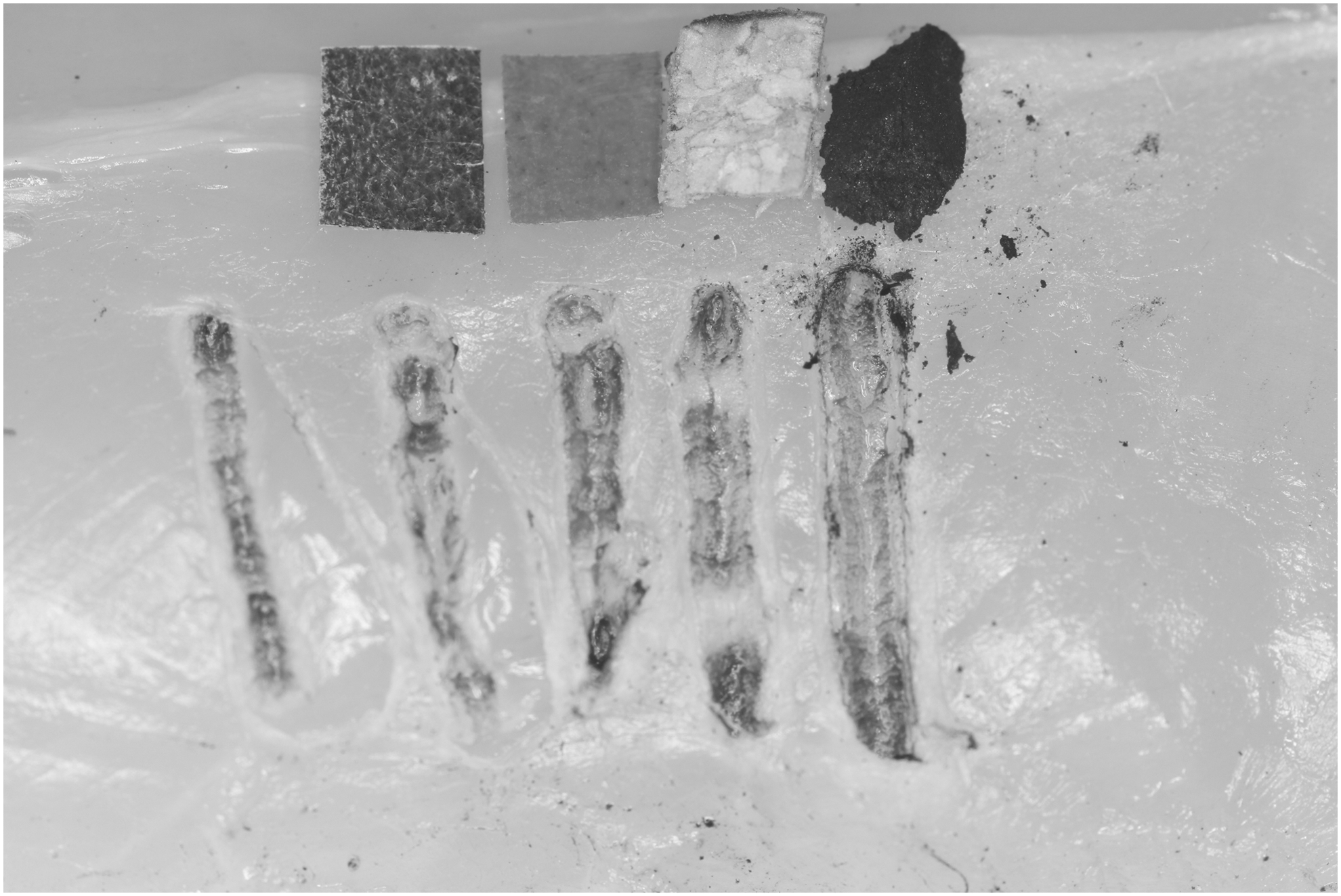
Incisions in chicken breast without skin, 6 W power setting with no initiator and the different initiators. From left to right: 6 W no initiator, 6 W blue articulating paper, 6 W red articulating paper, 6 W cork, and 3 W SureStep.
CW, continuous wave; SD, standard deviation.
Results
At a power of 3 and 6 W without any initiator, the soft tissues mean temperature increased by 5.7°C versus 12.4°C, respectively. Cork initiation at 3 and 6 W resulted in temperature increase by 4.88 versus 6.21°C, respectively. Incisions made using the blue/red articulating paper-initiated tip resulted in temperature increase by 2.9/5.8°C versus 8.2/7.6°C at 3 and 6 W power settings, respectively. With the SureStep initiator at 3 W, the temperature increased by 2.3°C and at 6 W by 4.1°C (Table 1). Statistical analysis via Dunn's multiple comparison test showed that when using a 3 or 6 W power setting, there was not a statistically significant difference between the groups (p > 0.05), but a statistically significant difference (p < 0.01) between the control (no initiated tip) group and the SureStep in 6 W. Higher power settings were associated with greater temperature rise and sometimes a temperature increase was found over the critical temperature threshold when the laser was used without initiator; however, the lowest temperature rise was recorded using the SureStep-initiated tip.
Discussion
The results of this study showed variability in the thermal effects of different initiators with the use of a 975 nm diode laser for soft tissue incisions. Using a continuous mode of 3 and 6 W, diode lasers can be used safely without damaging soft tissues when following appropriate guidelines and with tip initiation. 13 Such powers may be used, for instance, for efficient coagulation of hemangiomas and other vascular tumors, and removal of soft tissue tumors and gingival hyperplasias. It is important that the temperature increase does not exceed the critical threshold above body temperature to avoid irreversible tissue changes and collagen denaturation (peaks of denaturation at 42°C and 68°C). 15,16 This threshold (42–37°C = 5°C, considering that 37°C is the body temperature) was reached very rarely using 3 W power (without initiator or red articulating paper) and almost every time using the 6 W power (except in the use of SureStep). There are different temperature increases that result when different initiators are used at different power settings. This is of clinical significance in situations, where diode lasers are used to create tissue incisions of various depths and consistencies without proper initiation of the fiber tip. Manufacturers have the responsibility to provide clinicians with information and inform them of the effects of different initiators used for tissue ablation to best control overheating and prevent tissue necrosis.
In our study, the noninitiated tip was not efficient in cutting and showed temperature rise due to the deep penetration and absorption from the tissue chromophores. Specifically, the heat transfer is diffused within the tissue and not selectively absorbed by the superficial tissue layers.
In contrast to this, it seems that blue articulating paper or the SureStep is the safest method of fiber initiation, at 3 W, compared with the other initiators and no initiator providing the best cutting efficiency. Using the higher power of 6 W, it seems that SureStep is the safest method of fiber initiation since it reached the lowest mean maximum temperature. In addition, the SureStep initiator method reproduces predictable temperature changes during incisions and minimal temperature increases in soft tissues. Due to lack of statistical significance when comparing blue or red articulating paper to cork using a 3 or 6 W power, it seems that either of those options would result in similar effects if used to initiate a diode laser fiber before soft tissue incisions.
In addition, blue and red articulating papers, cork, and SureStep as initiator methods are nontoxic products, 14,17 and have FDA approval for clinical use.
Based on the experimental protocol used in this study, thermocouples were placed to record temperatures at 2 mm laterally and 3 mm deep to avoid damage of the thermocouple. Without doubt, the temperature increase is higher at the incision area. All this should be considered in clinical environment.
Further studies must be performed to develop the best method of diode laser tip initiation for soft tissue surgery to improve incision quality without tissue damage due to overheating.
Conclusions
Within the limitations of this study, all of the initiators are safe according to our experimental model. The power settings of the diode laser and type of initiator used both effect the degree to which the temperature of the soft tissue increases during incisions. At a higher power setting, there is a greater temperature increase. Using a continuous wave mode at both 3 and 6 W, the thermal increase was greatest when no initiator was used, whereas there was the least amount of temperature increase at 3 W when the blue articulating paper or the SureStep initiator was used and at 6 W when SureStep initiator was used.
Footnotes
Author Disclosure Statement
No competing financial interests exist.