
Abstract
Introduction
T
SGB has commonly been performed to alleviate pain and blood flow in patients with various diseases. However, SGB has not been widely accepted because of the risk of severe complications, lack of scientific evidence, and technical difficulties. Thus, xenon light irradiation has been used in clinical practice as an alternative to injection of agents for SGB, owing to its minimal tissue invasiveness, biopermeability, and optimal-range stable light energy. 3,4 In our previous study, we reported the usefulness of a treatment using xenon light (xenon phototherapy of the stellate ganglion, XPSG) for patients with tinnitus. 5
In the present study, we further evaluated the therapeutic effects of XPSG on tinnitus using the tinnitus handicap inventory (THI) and a numerical rating scale (NRS), in comparison with patients without XPSG.
Subjects and Methods
Subjects
XPSG group and non-XPSG group were defined as patients treated with XPSG for 3 months and those with 3 months of sham treatment followed by XPSG for 3 months, respectively. Subjects of XPSG group included 43 patients, consisting of 26 males and 17 females, with chronic tinnitus who visited the Department of Otorhinolaryngology of Fukushima Medical University Hospital or the Hoshi General Hospital between April 2014 and November 2016. Subjects of the non-XPSG group included 18 patients, consisting of 10 males and 8 females, with chronic tinnitus occurred between January and November 2016. Patients with pulsatile or objective tinnitus were excluded. Patients with physical conditions, such as auditory nerve tumor and inner ear malformations were also excluded.
Methods
This study was approved by the Ethics Committee of Fukushima Medical University (approval No. 1961). Patients were fully informed of the clinical efficacy and side effects of XPSG before consenting to participate in the study. Conventional medicine for tinnitus, such as vitamin supplements, drugs to improve blood circulation, and Chinese herbal remedies, were avoided during the study period. The dose of anxiolytics or sleeping aids for anxiety or sleep disorders was gradually reduced to zero while duly consulting with the patient.
The xenon phototherapy device, PHOS-01 (NIHON IKO Co., Tokyo, Japan), was used to perform XPSG by applying xenon light once every 4 sec for 10 min toward the area around the stellate ganglion bilaterally in a supine position in a bright room (Fig. 1). Xenon light was applied for every 1 sec for first 1 min, and every 4 sec for following 9 min. In principle, XPSG was performed once a week for 3 months with an amount of 18 J/cm2 energy per illumination session, resulting in 3510 J/cm2 in total 24 illumination sessions per phototherapy course. Similar procedure with emission of nonxenon light and beep, but not irradiation, was applied for the non-XPSG group. Patients in non-XPSG group were further treated with XPSG for 3 months after sham treatment periods.
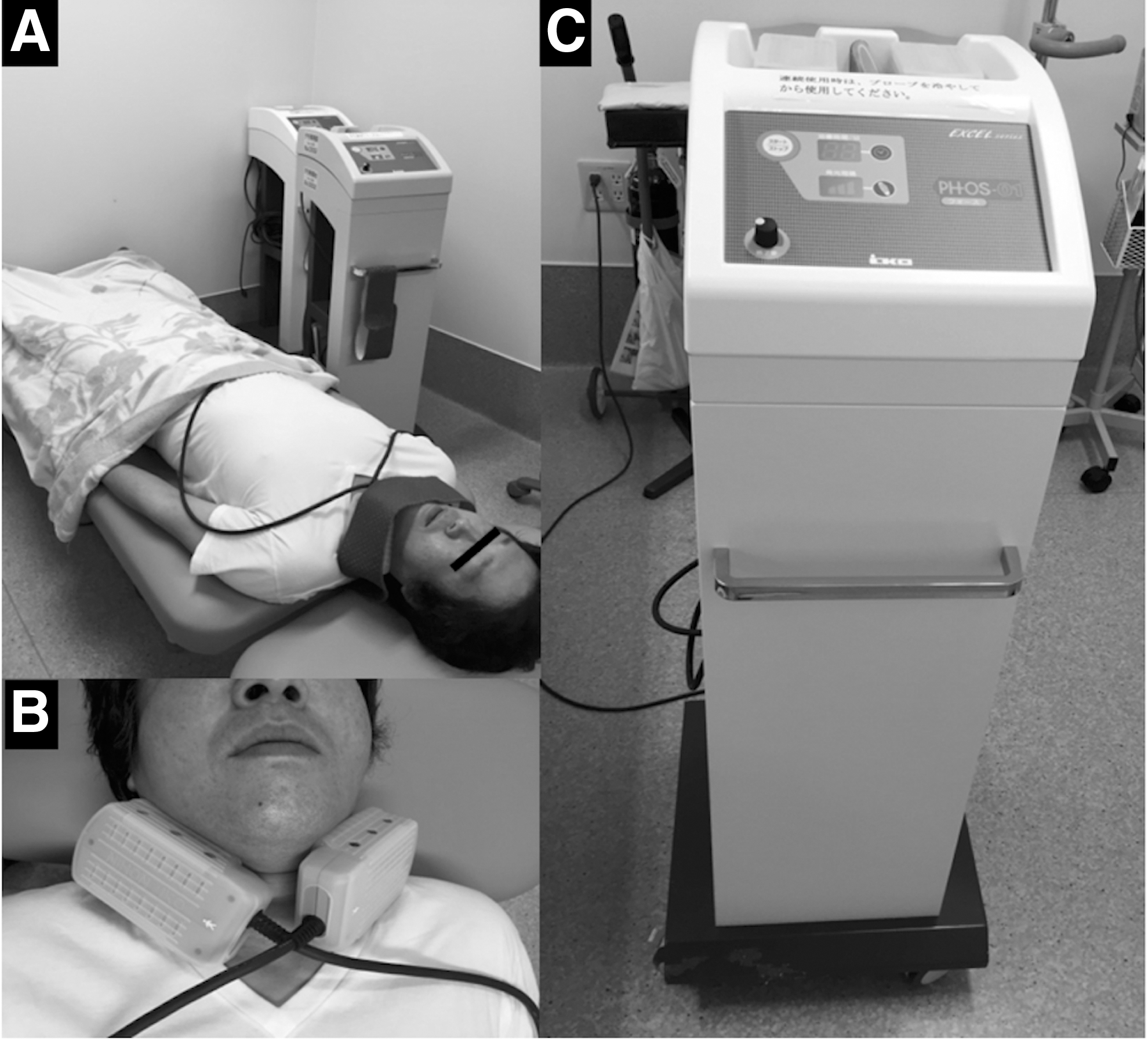
Treatment was performed in a supine position
Assessment
The effect of XPSG on tinnitus was subjectively evaluated at 3 months after therapy initiation using THI and NRS. The severity of tinnitus was rated as a scale between 0 and 100, and was classified into 4 grades based on THI scores: no handicap (0 to 16), mild (18 to 36), moderate (38 to 56), and severe (58 to 100). The degree of agony was rated from 0 to 10 on a 11-point NRS. Higher score means severer symptom.
Statistical analysis
Data were shown in mean ± standard error of the mean. Differences in scores between paired and unpaired two groups were compared using the Wilcoxon signed–rank test and Mann–Whitney U test, respectively. All analyses were carried out using SPSS 24.0 software (SPSS, Inc., Chicago, IL). In all tests, p < 0.05 was considered statistically significant.
Results
Patient characteristics
Mean age of subjects of XPSG group and non-XPSG group were 64 ± 2.2 and 63 ± 3.0 years old, respectively. Mean duration of the symptom in subjects of XPSG group and non-XPSG group were 38 ± 6.9 and 63 ± 11 months, respectively. No statistically significant differences were observed between two groups with respect to both age and disease duration of the symptom.
Tinnitus handicap inventory
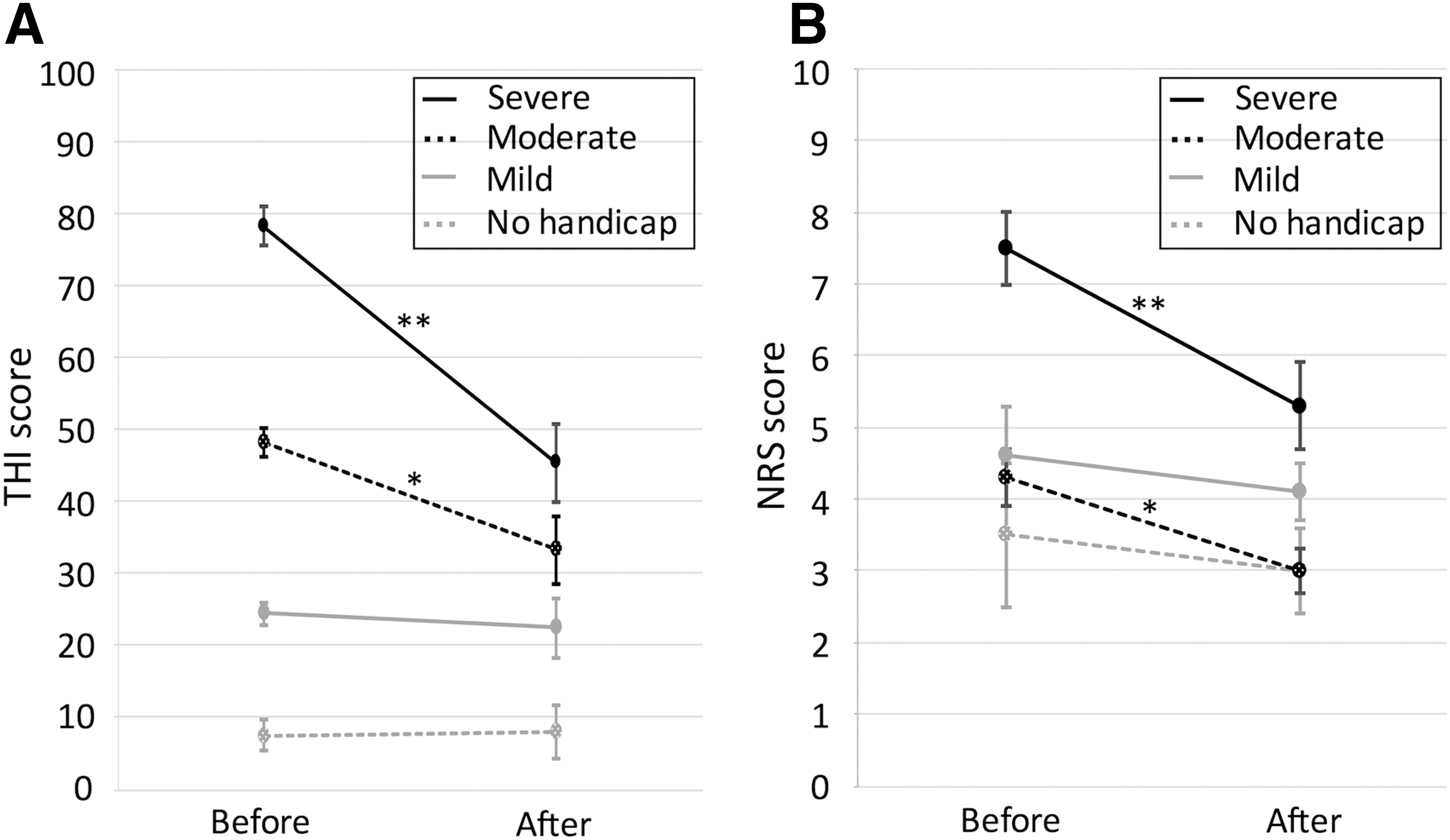
In XPSG group, mean scores of THI before and after XPSG for 3 months were 54.1 ± 4.3 and 34.6 ± 3.5, respectively, and the difference between them was statistically significant (p < 0.01) (Table 1). Statistically significant improvements of the score of severity after 3 months of XPSG were observed in patients with moderate (p < 0.05) and severe (p < 0.01) THI scores (Table 1, Fig. 2A). On the other hand, mean scores of THI before and after sham treatment in non-XPSG group were 54.4 ± 6.2 and 51.6 ± 6.7, respectively, showing no statistically significant improvement (Table 2). Mean score of THI after XPSG following sham treatment in non-XPSG group was 43.4 ± 6.1, without a statistical significance but with a tendency toward improvement (p = 0.06) (Table 2). Comparison of THI score improvement after treatment in XPSG group and after sham treatment in non-XPSG group demonstrated statistically significant difference (p < 0.01), confirming a therapeutic effect of XPSG.
THI
NRS, numerical rating scale; THI, tinnitus handicap inventory; XPSG, xenon phototherapy of the stellate ganglion.
p < 0.05; ** p < 0.01.
NRS, numerical rating scale; THI, tinnitus handicap inventory; XPSG, xenon phototherapy of the stellate ganglion.
Numerical rating scale
In XPSG group, mean scores of NRS before and after XPSG for 3 months were 5.8 ± 0.4 and 4.4 ± 0.3, respectively, and this difference was statistically significant (p < 0.01) (Table 1). According to severity grade, statistically significant improvement of NRS scores after XPSG for 3 months were observed in patients with moderate (p < 0.05) and severe (p < 0.01) THI scores (Table 1, Fig. 2B). On the other hand, mean scores of NRS before and after sham treatment in non-XPSG group were 5.8 ± 0.6 and 6.1 ± 0.6, respectively, showing no statistically significant improvement (Table 2). Mean score of NRS after XPSG following sham treatment in non-XPSG group was 5.3 ± 0.5, without a statistical significance, but with a tendency toward improvement (p = 0.07) (Table 2). Comparison of NRS score improvement after treatment in XPSG group and after sham treatment in non-XPSG group demonstrated a statistically significant difference (p < 0.01), confirming a therapeutic effect of XPSG.
Discussion
The phototherapy was reported as a treatment of the intractable skin ulcer for the first time in 1973. 6 There have been many reports with respect to phototherapy since then. 4 Xenon light is generated using xenon gas as a medium and containing multiwavelength light with broadband wavelength ranging from ultraviolet to infrared light. 7 The xenon light we used this time reached ∼7 cm in depth, and the irradiation energy per one emission of light was 18 J/cm2 at the skin surface. There are 195 times of emitted light by irradiation for 10 min, and the total irradiation energy became 3510 J/cm2. The irradiated area by the probe is about 27 cm2, which allowed xenon light to illuminate a wide area. Xenon light peaks around 700–900 nm, and thus has excellent water and blood permeability, penetrating not only the surface layer, but also deep layers of biological materials. Due to its high energy, xenon light promotes vasodilation through the sympathetic nervous system and facilitates tissue restoration. 7
The stellate ganglion is located anterior to the transverse process of the seventh cervical vertebra and posterior to the vertebral artery, and is ∼2 cm in depth from the anterior surface of the neck. 8 Xenon light irradiation is expected to increase blood flow through functional suppression of stellate ganglion, suggesting that this technique is simple and safer than conventional SGB. However, local low temperature burns and malaise may occur as adverse effects. Actually, although the spectral range of xenon light is 260–1100 nm, the current device provides the light peaks around 700–900 nm, which is readily absorbed into the skin. However, in the present study, we did not observe any XPSG-related adverse events, except for mild vertigo with prompt spontaneous recovery in one patient, suggesting that XPSG is a safe treatment approach even for elderly individuals. With regard to the effect on tinnitus, overall THI and NRS scores improved statistically significantly after 3 months of XPSG, especially in patients with severe tinnitus.
Psychological factors, such as mental vulnerability, anxiety, and stress, aggravate tinnitus. 9 Accordingly, it is debatable whether xenon light improved tinnitus only by increasing blood flow through vasodilation. In the non-XPSG group, which is served as control in the present study, we used a special probe that allows emission but inhibits illumination by the light. This was designed to reveal possible placebo effects, specifically the involvement of mental control mechanisms on the improvement of tinnitus. We found no significant difference in THI or NRS scores between the XPSG and non-XPSG groups. XPSG was subsequently performed under the same conditions after sham treatment in non-XPSG group, showing significant improvement of THI scores after 3 months of XPSG.
The clinical efficacy of other treatment modalities for tinnitus was reported to be 50% with cognitive behavioral therapy, 10 and 60–80% with tinnitus retraining therapy. 11 In the present study, 22 (51%) of 43 cases demonstrated improvement of THI score by 20 or greater points, which was shown to be 95% confidence intervals, 12 suggesting that XPSG is comparable with those methods.
The above findings showed that XPSG provided high levels of satisfaction to patients by significantly improving THI and NRS scores. However, our investigation of XPSG is still in the early phase. Identification of predictive factors for responder to this treatment may be also useful. In 22 responders showing improvement of THI scores 20 or greater points, a notable but not significant shift toward lower pitch, was observed using pitch match (data not shown). In remaining 21 nonresponders, no obvious change of pitch was observed (data not shown). Therefore, pitch match may be a possible way to identify a responder. Apart from neuro-otological assessment, conventional factors, including thickness of the neck and body weight may be a candidate. However, those are not included in the present study. Further studies are required to establish this procedure as a potent treatment for severe tinnitus.
Conclusions
In conclusion, we demonstrated statistically significant improvements of both THI and NRS scores after XPSG for 3 months in patients with subjective tinnitus. Severe cases with high THI or NRS score showed greater improvements. On the other hand, no significant difference was observed between before and after sham treatment in non-XPSG group. XPSG is a possible treatment modality for patients with tinnitus.
Footnotes
Author Disclosure Statement
No competing financial interests exist.