
Abstract

S 1. Percentage of colony-forming efficiency (CFE) 2. Percentage of relative WH/burn healing 3. Collagen concentration 4. Tensile strength
Laser therapy started with clinical applications, and was followed by a number of animal and human research studies, which produced positive, as well as no effects. Our consistent research in biomodulation has established numerous findings.
Cell Culture
Several studies were created to determine the effects of lasers and WH drug doses for the stimulation and to inhibit normal and neoplastic cells in vitro. Medical use of laser biomodulation has been used for decades for tissue healing and inflammatory conditions. The use of laser photons to modulate the regeneration and differentiation of early cellular precursors has been a valuable endeavor to discover novel and efficient methods, and was seeded with 400 cells/dish of normal cells (CHO, 3T3, CCL-226, and HSF), and neoplastic cells (EMT-6, RIF-1), with cell cultures stained, determining the percentage of CFE.
A trend of stimulation, zero bioactivation, and inhibition or zero bioactivation, stimulations, and inhibitions in all cell lines was observed at different levels 1 : specifying a significant increase in CFE over the control indicates stimulation, a significant decrease indicates inhibition, and an insignificant difference indicates zero bioactivation. Colonies with <50 cells were excluded and no correction for cell multiplicity was done.
Laser irradiation is believed to enhance cellular respiration. Karu et al. 2 proposed a chain of molecular events that commences with the absorption of photon by photoreceptors to stimulate the primary photochemical and photo physical events within the mitochondria. The photon produces a change in the redox state of the respiratory chain that generates more energy as adenosine triphosphate (ATP). The heightened availability of ATP triggers cellular metabolic processes necessary during cell division. This is relevant to our observation. 1 This means that different photochemical pathways occur when given similar energy doses and that irradiation with low power laser induces cell proliferation. The biostimulatory effect of laser irradiation may, therefore, explain an enhanced WH at the level of the whole organism.
Cellular proliferation is influenced by the type of cells involved. The risk occurs when laser irradiation is performed on patients with undiagnosed neoplasms, and during pregnancy, wherein the cell culture alone established the dose dependency of cell growth to laser treatments.
The ability of laser irradiation to regulate embryonic fibroblasts and human skin fibroblast in vitro suggests possible laser biomodulatory effects on embryonic and adult stem cells directed for tissue regeneration. 1 This shows the vulnerability and unwanted effects of laser for cancer patients and pregnant women. Further studies are needed to determine the effects of light treatments that explore different laser parameters for the cloned expansion and the differentiation of stem cells.
Laser, LED, and Drugs
Male Sprague-Dawley (SD) rats (N = 893) were used for normal diabetic wound and normal diabetic burns (induced diabetic-streptozotocin). SD was prepared according to the normal protocol. Continuous wave (CW) lasers 632.8 nm were used to irradiate tissue culture dishes. HeCd, argon, HeNe, krypton, GaAlAs, CO2, and diode lasers (532, 633, 670, 785, 810, 980, and 10,600 nm) were used in vivo. 3 An array of 25 LED cluster 510–872 nm [visable (V) to infrared (IR)] was used for comparison 1,3 with a 3- to 2-week schedule as optimum treatment, using 5, 10, 20, and 30 J/cm2 as incident energy density (I. dose) and C. dose (corrected dose from skin and Plexiglas cage absorption). Wound area was plotted. A linear fit determined the trend. The percentage of rate of wound healing divided by original burn (RWH/B) healing acceleration or deceleration was computed and skin samples collected from each laser were used for analysis. Samples were snap-frozen in liquid nitrogen until a measurement was performed for tensile strength. Biomechanical analysis was done by material testing system, 4 and total collagen content was calculated. SD skin and Plexiglas cage absorption was determined for dose correction. Solcoseryl™ (SS), Polygen™ (PG), and Regranex™ (RG) agents were used in vivo to compare or were combined with lasers. The effect of laser biostimulation in combination with SS and PG was used in the enhancement of WH.
Wound and Burn
Many in vivo studies have demonstrated that laser healers can promote. WH and burn healing on animals. Our studies elaborated on the usefulness of laser therapy and searched for the parameters that control this phenomenon using a model of animals to optimize on their advantage for human use. Our results showed that laser therapy, used with appropriate treatment parameters, accelerates burn healing on diabetic rats through the use of both visible and IR. The effects of visible lasers worked better than those of invisible lasers for diabetic rats. The WH on control rats with diabetes was slower than on control without diabetes. Laser therapy can enhance the WH on diabetic rats. The optimum wavelength was 632.8 nm and the optimum incident dose was 20 J/cm2 (4.71 J/cm2) (Fig. 1).
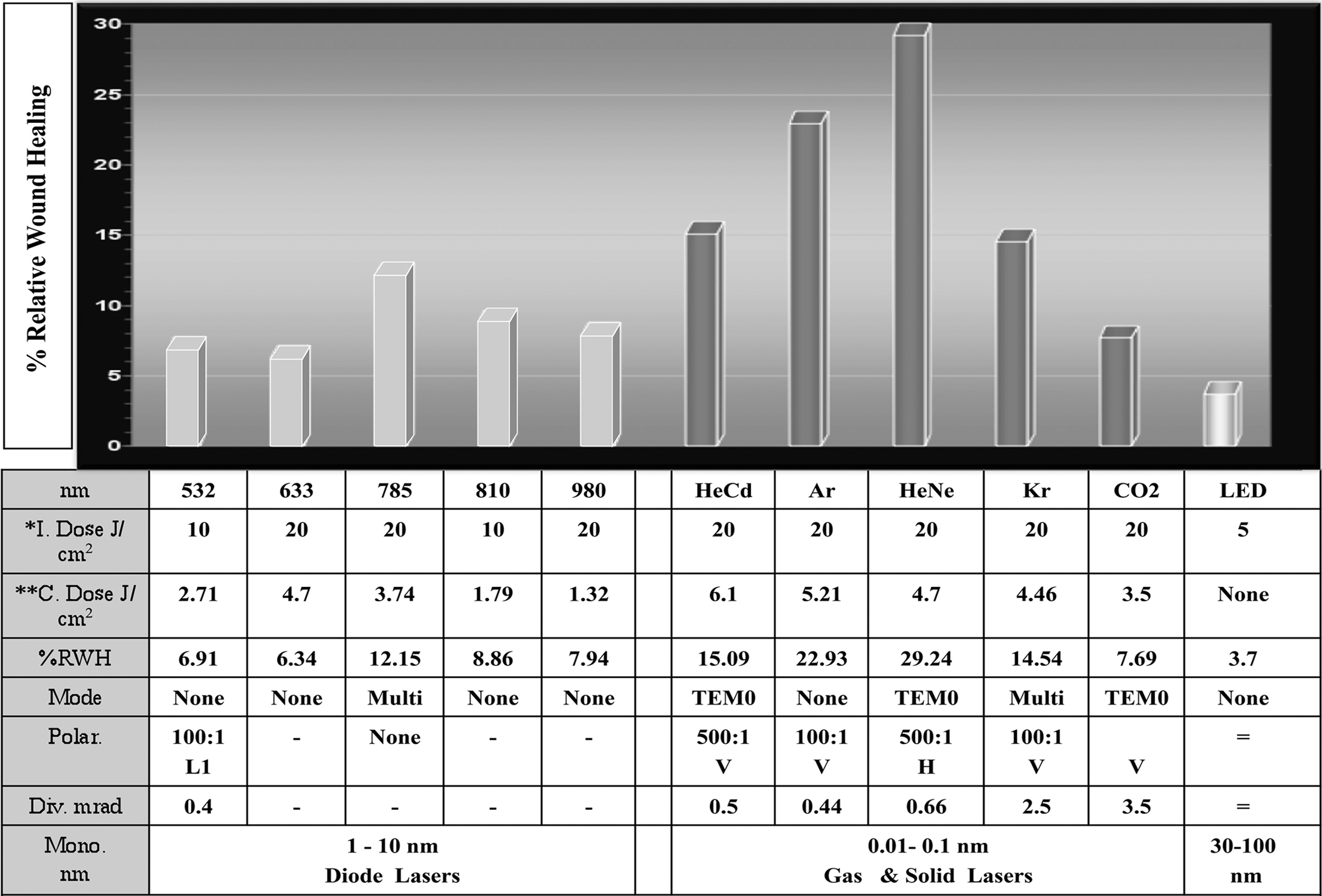
% RWH comparison of different lasers and LED. RWH, rate of wound healing.
Using laser, LED, and drugs, results suggest that further stimulation can be achieved (+10%) by using 633 nm laser with SS and PG. This could be used as a new treatment modality (Fig. 2). Although agents were manufactured for human use, experiments with our models were performed to determine their efficacy for rats.

The best % RWH/B using lasers and LED and pharmaceuticals drugs. RWH/B, rate of wound healing divided by original burn.
Using different lasers is difficult, and simpler, cheaper, less bulky devices would work better. The resurgence of LED as a source of photons makes multi-wavelength exposure possible. An array of 25 LED cluster emitting light from V-IR was used. The use of LED in micro or zero gravity has been espoused by Whelan. 5 The NASA Marshal Space Flight Center-SBIR Program seeks to develop an effective alternative to lasers for typically elevated total atmospheric pressure in undersea environments, where a decrease in oxygen impairs healing. LEDs' simplicity and ruggedness make them a good choice for space flight and for use as submarine standard medical equipment. The comparisons of the efficacy of various lasers with LED produced inferior results within earlier studies. 5
The use of a diode laser that is smaller and more convenient for applications is an alternative.
Biomodulation depends on laser wavelengths, doses, and treatment schedules, and not on dose rates and laser skin transmissions. 1 –5 Dose dependency trend is stimulation, zero bioactivation, and inhibition for in vitro and in vivo. CW lasers are better than the pulse (CW chopped), with more healing enhancement from visible lasers than invisible laser. 2
The gas laser reading effects (29.24-% RWH) superseded the diode laser reading effects (6.34-% RWH), which could be related to laser monochromaticity (0.01–0.1 nm), with diode laser (1–10 nm) (Fig. 1).
Biomodulation could stimulate healing for diabetic wound and decubitus ulcers. Moreover, biomodulation can be used as an inhibitor for scar(s) and keloid, or as a stimulator for organ transplant controlling no/or excessive healings. The use of laser therapy to accelerate normal wound closure is a great tool for use by the astronauts in outer space where gravity is almost zero, and in navy submarines where the air pressure is high, replacing traditional drug remedies.
These are the percentage results of RW/B acceleration:
Laser converts healing days in diabetic burn from negative 45% to positive 8%, with gain of 53.4%, and diabetic WH from negative 40% to negative 5%, with gain of 38.5%.
An impaired WH condition, such as diabetes, was alleviated by the use of low power laser and LED therapy. The 633 nm laser, used at incident dose 20 J/cm, 2 was good for enhancing cicatrization in the normal wound; 633 nm, used at 10 (2.35 J/cm2), was best in diabetic wound, with the normal burn at 30 (7.06 J/cm2), and at 20 for diabetic burn healing. This series of studies also showed that 20 and 10 J/cm2 doses were consistent with the increase in tensile strength and total collagen content of the scar.
Conclusions
Normal or impaired WH/burn healing can be improved through the use of lasers, LEDs, drugs treatment, or combination therapy through enhanced tensile strength, and total collagen of scarred skin, healing acceleration, and collagen content. Tensile strength is important with newly formed scars that are wavelength and dose dependent.
Results showed that although effects were minimal in normal model, the effects in the diabetic model were promising. This implies the utility of phototherapy enhances the success of skin grafting during reconstructive surgeries and impaired healing, and can be applied for deep sea and space travel.
Clinical trials using the computed corrected doses for each laser, and incident dose for LED should inspire further advances for phototherapy in the mainstream of clinical practice.
Photons emitted by lasers effect the biological system. Earlier studies indicate a side effect of low power laser 1 –5 of the biomodulation of normal and neoplastic cells. With optimum parameters, cellular proliferation can be modulated, microcirculation improved, and fibroblast rapidly developed. Because the laser in use is low in power, the biological effects are biochemical and not thermal in nature; therefore, no events of increased temperature occur that could damage living tissues.
The use of phototherapy with lasers/LED in diabetic wound model is astounding. Normal WH is a natural response, designed to restore tissue integrity after tissue injuries.
The more the results we have from studying the use of phototherapy in diabetic burn healing, the greater will be the appreciation for various lasers/LEDs as simple, yet effective tools for those with diabetes suffering with burns.
Our research results show that phototherapy increases the collagen concentration, which is the building block of the wound matrix. Despite the fact that collagen content and tensile strength were minimal in the normal model, the results in the diabetic model are truly promising.